Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Ic ppw - 2014
The Offices of Roland D. Reinhart, M.D. (760) 341-2360
Date:______________ Dear: ___________________________________, This letter is to formally welcome you to the Offices of Dr. Roland D. Reinhart and to remind you of your upcoming new patient consultation appointment. Dr. Reinhart and his team of professionals are committed to providing a comprehensive and compassionate approach to patients who are suffering from pain. Our practice offers a systematic and focused approach that enables patients with chronic pain to lead an active and productive lifestyle. “Now more then ever you have options to alleviate your pain.” Just a reminder…
With: Roland Reinhart, M.D. Location: Rancho Mirage If you are unable to keep this appointment, please call us to reschedule. Also, please complete the following enclosed information and bring it with you along with the additional items listed below. Please bring: 1. A list of current medications, which includes dosage and frequency. 2. Your insurance card(s). 3. Any available records or reports that may pertain to your visit.
Should you have any further questions regarding your upcoming appointment, please call our office at (760) 341-2360.
The Offices of NEW PATIENT EVALUATION FORM Roland D. Reinhart, M.D. (760) 341-2360
In order to help us provide the best possible care for you at our office, we ask for your cooperation in providing the following information. Please bring this form with you to your first appointment. GENERAL INFORMATION Date form completed _____/_____/_____ Patient Name:____________________________________________ Date of Birth:_____/_____/_____
Referred By:_______________________________ Primary Physician:______________________________ Emergency Contact:__________________________ Relationship:____________ Tel#:_________________ Preferred Pharmacy:______________ Location:_________________________ Tel #:_________________ Chief Complaint:_________________________________________________________________________ Circle any tests you have had for your current pain:
X-Ray CT Scan MRI Myelogram Bone Scan EMG Blood Tests Other:_____________________
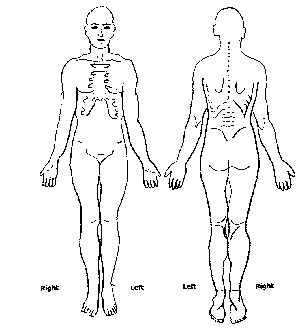
CAUSE OF PAIN:_______________________________________________________________________ DURATION: LOCATION OF YOUR PAIN
Date your pain first occurred: _________________ Unknown:
On the picture color in all your areas of pain
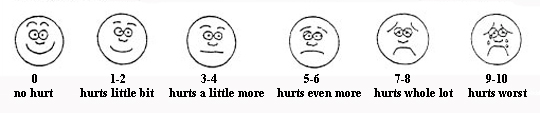
TIMING: The initial onset of pain was: ____Gradual ____Sudden ____Unknown ACTIVITIES OF DAILY LIVING SIGNIFICANTLY IMPACTED BY PAIN: □ Bathing and showering SEVERITY OF PAIN: Circle how you would describe your pain during the past week:
None Mild Moderate Horrible Excruciating
HISTO Over tRhY at iSt s worst:________ Pain at its best:________ Pain right at this moment:________ Age________ Race_______________ Sex_____ Who is completing the paperwork______________________
Patient Nam P
e: LEASE DRAW WHERE YOU
___________________________RD PA The Offices of Roland D. Reinhart, M.D. (760) 341-2360 QUALITY OF PAIN: The questions below refer ONLY to the area of pain that you are coming to our clinic for at this time Circle the word that better describes the pattern of pain: Circle the word(s) that best describe what your pain feels like:
Knifelike Spasm Jabbing Throbbing Stabbing
Cramping Shooting Aching Deep Pressure Numbness Tingling ASSOCIATED SIGNS AND SYMPTOMS: Mark all that apply. ____Headache ____ Swelling ____ Light-headedness ____ Nausea ____ Vomiting ____ Fatigue ____ Pain that wakes you up ____ Pain with the first steps in the morning ____ Pain after periods of resting ____ Weakness ____ Loss of bowel control ____ Loss of bladder control ____ Fever/Chills ____ Unexplained weight loss-How many pounds? ____lbs. ____Other:______________________________________________________________________________________________ ____Stiffness in:_________________________________Right / Left
____Tenderness in:_______________________________ Right / Left ____Weakness in:________________________________ Right / Left MODIFYING FACTORS: Circle which makes your pain better:
Activity Sitting Standing Lying Down Rest Medication Heat Ice Changing Positions Stretching Movement Walking No Movement Other:________________________________ Circle which makes your pain worse:
Walking Sitting Standing Lying Down Heat Ice Cold Weather Activity Rest Medication
Changing Positions Lack of Activity Bending Lifting Twisting Turning Movement Lights Stress Other (Explain):_________________________________________________________________________________________ MEDICATIONS: Please list all medications you currently use, the medication strength and how often you take it. Name of Medication Strength/MG Frequency The Offices of Roland D. Reinhart, M.D. (760) 341-2360 ALLERGIES: Please list any allergies to medications and the reaction experienced. Name of Medication Reaction Experienced Please list any other allergies that may be pertinent, such as Latex, IVP dye, etc.______________________________ __________________________________________________________________________________________________ PAST MEDICAL HISTORY Have YOU had any of the following conditions? (Check all that apply)
( ) Asthma ( ) Bleeding Disorder ( ) Cancer: What Area ___________________ ( ) Diabetes ( ) Emphysema
( ) Heart Attack ( ) Heart Disease ( ) High Blood Pressure ( ) Kidney Disease ( ) Mental Illness ( ) Seizure Disorder ( ) Stroke
( ) Suicidal Thoughts ( ) Thyroid Disease ( ) Tuberculosis ( ) Other_________________________
PAST SURGICAL HISTORY Please list all previous surgeries: Date (Month/Year) Procedure: ___________________________________________ __________________________________________________
___________________________________________ __________________________________________________
___________________________________________ __________________________________________________
___________________________________________ __________________________________________________
___________________________________________ __________________________________________________
SOCIAL HISTORY Do you drink alcohol? Never Rarely Occasionally Often Socially Do you drink caffeine? Never Rarely Occasionally Often Do you smoke? YES / NO If yes, How many per day? ______ How many years have you smoked?______
Educational Background (highest grade completed):
( ) Junior High ( ) High School ( ) Technical or Business School ( ) College Degree ( ) Graduate Degree
Marital Status / Family: ( ) Single
( ) Divorced How Long?_________________
Who lives with you?________________________________________________________________________________
Occupation:__________________________ ( ) Full Time ( ) Part Time ( ) Retired? How Long_________
( ) Disabled? How Long_________________________________
Have you ever been treated for depression? YES / NO If yes, when?_______________________________________ Have you been physically abused? YES / NO Have you been emotionally abused? YES / NO Are you under the care of a psychologist or psychiatrist? YES / NO If yes, who?____________________________ The Offices of Roland D. Reinhart, M.D. (760) 341-2360 FAMILY HISTORY
Mark if any (blood) relatives have had any of the following:
Who had the condition? Is the person living or deceased? PAST TREATMENT HISTORY Please check the following items you have tried and whether or not they helped decrease your pain:
( ) Acupuncture-Did it help? Y/N
( ) Biofeedback-Did it help? Y/N
( ) Chiropractor-Did it help? Y/N
( ) Spinal Cord Stimulator-Did it help? Y/N
( ) Epidurals-Did it help? Y/N
( ) Heat-Did it help? Y/N
( ) Home Exercises-Did it help? Y/N
( ) Ice-Did it help? Y/N
( ) Hypnosis-Did it help? Y/N
( ) Massage-Did it help? Y/N
( ) Intraspinal Pump-Did it help? Y/N
( ) Steroid Injections-Did it help? Y/N
( ) Physical Therapy-Did it help? Y/N
( ) TENS Unit-Did it help? Y/N
( ) Surgery-Did it help? Y/N
( ) Botox Injections – Did it help? Y/N
( ) Trigger Point Injections-Did it help? Y/N
( ) Other____________________-Did it help? Y/N The Offices of Roland D. Reinhart, M.D. (760) 341-2360 PAST MEDICATION HISTORY Please check the following medications you have tried and whether or not they helped decrease your pain: ANTI-INFLAMMATORIES MUSCLE RELAXERS
( ) Advil-Did it help? Y/N
( ) Flexeril-Did it help? Y/N
( ) Alieve-Did it help? Y/N
( ) Soma-Did it help? Y/N
( ) Celebrex-Did it help? Y/N
( ) Zanaflex-Did it help? Y/N
( ) Ibuprofen-Did it help? Y/N
( ) Skelaxin-Did it help? Y/N
( ) Mobic-Did it help? Y/N
( ) Ultram-Did it help? Y/N
( ) Other____________________-Did it help? Y/N
( ) Other_________________-Did it help? Y/N
( ) Other____________________-Did it help? Y/N
( ) Other____________________-Did it help? Y/N NARCOTICS NARCOTICS
( ) Actiq-Did it help? Y/N
( ) OxyIR-Did it help? Y/N
( ) Darvocet-Did it help? Y/N
( ) Percocet-Did it help? Y/N
( ) Demerol-Did it help? Y/N
( ) Percodan-Did it help? Y/N
( ) Dilaudid-Did it help? Y/N
( ) Roxicodone-Did it help? Y/N
( ) Duragesic Patch-Did it help? Y/N
( ) Vicodin-Did it help? Y/N
( ) Morphine-Did it help? Y/N
( ) Methadone-Did it help? Y/N
( ) Norco-Did it help? Y/N
( ) Oxycontin-Did it help? Y/N
( ) Other_________________-Did it help? Y/N
( ) Other_________________-Did it help? Y/N
( ) Other_________________-Did it help? Y/N
( ) Other_________________-Did it help? Y/N
I, the undersigned, have completed this form to the best of my knowledge. The information that I have provided is true and accurate to the best of my knowledge. I understand that this information is used in the care and treatment plan while under the care of all physicians and staff at The Offices of Roland D. Reinhart, M.D. __________________________________________
The Offices of Roland D. Reinhart, M.D. (760) 341-2360 REVIEW OF SYSTEMS DATE:________________________________
Please review the following list and mark any that apply to you for today’s visit:
Constitutional Respiratory Neurological Gastrointestinal Ear, Nose, Throat Psychiatric Genitourinary Endocrinology Cardiovascular Musculoskeletal Hematologic/Lymphatic Allergy / Immunology The Offices of Roland D. Reinhart, M.D. (760) 341-2360
Additional Information Required by the U.S. Government
Have you received an influenza immunization either during last flu season (September 2011 - February 2012) or this flu season (September 2012 - February 2013)? Y / N Date/Approximate Date: ______________________ Have you ever received a pneumococcal vaccination (for pneumonia)? Y / N Date/Approximate Date: ______________________ Have you had a total colectomy (the entire colon removed)? Y / N Date/Approximate Date: ______________________ Have you had a colonoscopy? Y / N Date/Approximate Date: ______________________ Have you had a sigmoidoscopy (partial colonoscopy)? Y / N Date/Approximate Date: ______________________
Trius Therapeutics Completes Enrollment in Second Phase 3 Trial of Tedizolid for Skin and Skin Structure Infections SAN DIEGO, Dec. 10, 2012 (GLOBE NEWSWIRE) -- Trius Therapeutics, Inc. (Nasdaq:TSRX), a biopharmaceutical company focused on the discovery and development of innovative antibiotics for life-threatening infections, announced today that it has reached its enrollment objective of 6
C U R R I C U L U M V I T A E INFORMAZIONI PERSONALI SEGALA MARCO DANIELE V. xxxxxxxxxxx MILANO 02xxxxxx 02xxxxxx CODICE FISCALE SGLMCD55C31E704U Data di nascita 31 MARZO 1955 LOVERE (BG) ESPERIENZA LAVORATIVA • Date (da – a) 2009 ad oggi • Nome e indirizzo dell’attuale datore Direzione Scientifica - Ufficio Formazione Permanete ed Aggi
 The Offices of
The Offices of