Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Atypicalhus.net
Pediatr Nephrol (2010) 25:2539–2542DOI 10.1007/s00467-010-1606-y
Neurological involvement in a child with atypical hemolyticuremic syndrome
Bérengère Koehl & Olivia Boyer & Nathalie Biebuyck-Gougé & Manoelle Kossorotoff &Véronique Frémeaux-Bacchi & Nathalie Boddaert & Patrick Niaudet
Received: 13 April 2010 / Revised: 1 July 2010 / Accepted: 2 July 2010 / Published online: 17 August 2010# IPNA 2010
Abstract We report the case of a 4-year-old boy, diagnosed
the cerebral pedunculas, caudate nuclei, putamens, thalami,
with atypical hemolytic uremic syndrome (HUS) due to a
hippocampi, and insulae suggesting thrombotic microangi-
hybrid factor H. He progressed to end-stage renal failure
opathy secondary to a relapse of HUS rather than reversible
despite plasmatherapy and underwent bilateral nephrectomy
posterior leukoencephalopathy syndrome (RPLS), usually
because of uncontrolled hypertension. Three days after, he
occipital and asymmetrical. Plasmatherapy led to a com-
had partial complex seizures with normal blood pressure,
plete neurological recovery within 2 days although hyper-
normal blood count and normal magnetic resonance
tension had remained uncontrolled. The fourth MRI
imaging (MRI), which recurred 1 month later. Eight months
10 weeks after, on maintenance plasmatherapy, was normal
later, he had a third episode of seizures, with hemoglobin of
and clinical examination remained normal, except for high
10 g/dl without schizocytes, low haptoglobin of 0.18 g/l,
blood pressure. In conclusion, brain MRI allows differen-
and moderate thrombocytopenia (platelets 98 × 109/l). He
tiating thrombotic microangiopathy lesions from RPLS in
remained hypertensive and deeply confused for 2 days. The
atypical HUS, which is crucial since lesions may be
third MRI showed bilateral symmetrical hyperintensities of
Keywords Atypical hemolytic uremic syndrome .
B. Koehl : O. Boyer : N. Biebuyck-Gougé : P. Niaudet
Cerebral thrombotic microangiopathy .
Reversible posterior leukoencephalopathy syndrome .
Hôpital Necker-Enfants Malades, Université Paris Descartes,
Hôpital Necker-Enfants Malades,Paris, France
Hemolytic uremic syndrome (HUS) is characterized by the
triad of microangiopathic hemolytic anemia, thrombocyto-
Hôpital Necker-Enfants Malades, Immunology Department,
penia, and acute renal failure. In children, atypical HUS is
Hôpital Européen-Georges Pompidou, Université Paris Descartes,
often secondary to genetic abnormalities of the complement
alternative pathway proteins. Among extra-renal complica-
tions, central nervous system manifestations are observed in
Pediatric Radiology, Hôpital Necker-Enfants Malades,
20% to 50% of cases and are responsible for increased
P. Niaudet (*)Service de Néphrologie Pédiatrique,
Hôpital Necker Enfants Malades,149 rue de Sèvres,
We report the case of a previously healthy 4-year-old boy,
75743 Paris cedex 15, Francee-mail: pniaudet@gmail.com
first admitted because of a 3-week history of asthenia and
vomiting, without diarrhea. On admission, he was anuric,
hemodialysis, and antihypertensive treatment. He presented
his blood pressure was 120/88 mmHg, and physical
neurological symptoms for 2 days, including deep confu-
examination was remarkable only for peripheral and
sion and violent agitation. The clinical and biological
palpebral edema. The first laboratory tests revealed:
symptoms were more suggestive of hypertensive encepha-
hemolytic anemia (hemoglobin 5.1 g/dl with schizocytes,
lopathy than a HUS relapse, and a third MRI was
haptoglobin 0.06 g/l), thrombocytopenia (platelets
performed 2 days after the seizures (Fig. On FLAIR
108 × 109/l), renal insufficiency (plasma creatinine
and T2 sequences, this brain MRI showed bilateral sym-
594 μmol/l, urea 42.6 mmol/l), and nephrotic syndrome
metrical hyperintensities on the cerebral pedunculas, cau-
(plasma albumin 23.5 g/l, proteinuria 23.4 g/l). Stool
date nuclei, putamens, thalami, hippocampi, and insulae.
culture, polymerase chain reaction (PCR) of Shiga-toxin
Diffusion-weighted imaging sequence and ADC mapping
(Stx) in stools and detection of serum antibodies against
displayed no abnormality. These findings were suggestive
lipopolysaccharides (LPS) were negative. CH50, C3, C4,
of thrombotic microangiopathy, probably due to a relapse
complement factor H (CFH) antigen, factor I antigen, CD46
of HUS, rather than RPLS-related abnormalities.
expression, and von Willebrandt factor (vWF) protease
He was immediately treated with daily plasma
activity were normal. Genetic analysis of complement
exchanges (PE) that led to a complete neurological
protein genes was negative at that time but a CFH hybrid
recovery within 2 days although hypertension had remained
uncontrolled. He received daily PE for 1 week, progres-
He was started on peritoneal dialysis and plasmatherapy.
sively tapered to twice a week. After a total of 10 sessions
After three plasma infusions and seven plasma exchange
within 4 weeks, plasma exchanges were replaced by weekly
sessions, urine output gradually increased and plasma
plasma infusions during hemodialysis sessions. The fourth
creatinine progressively decreased to 117 μmol/l. He
brain MRI after 10 weeks of weekly plasma infusion was
remained severely hypertensive. Two weeks later, a first
normal and clinical examination remained normal, except
relapse was treated with seven plasma exchanges, which
improved hematological parameters, but renal functionworsened. Hematological remission persisted, but despiteplasma exchanges twice a week for 4 months followed by
plasma infusions twice a week for 2 months, he progressedto end-stage renal failure. Eight months after the onset, he
Central nervous system involvement (irritability, drowsi-
was started on chronic hemodialysis. One month later, he
ness, convulsions, cortical blindness, hemiparesia or coma)
underwent bilateral nephrectomy because of uncontrolled
is the most frequent extrarenal complication in HUS, and
hypertension despite five anti-hypertensive drugs. Three
MRI findings are diverse. Two situations may be radiolog-
days after nephrectomy, he presented partial complex
ically delineated: RPLS-related lesions and microangio-
epileptic seizures of unclear etiology, without hemolysis
pathic lesions. The clinical symptoms in both situations are
or thrombopenia. The blood pressure, controlled by
antihypertensive treatment of IV nicardipine followed by
Brain MRI RPLS-related lesions are associated with a
oral labetalol and nifedipine, was at that time stable and
posterior white matter hyperintensity and sometimes poste-
normal. Brain magnetic resonance imaging (MRI) 3 days
rior cortex hyperintensity probably secondary to high
after seizures was normal. The electroencephalogram
blood pressure during the acute phase of HUS. White-
(EEG) showed a posterior basic rhythm disrupted by many
matter hyperintensity is predominant in parieto-occipital
slow and monomorphic theta and delta waves.
One month later, he had a recurrence of generalized
Another type of brain MRI lesions is also described
seizures without hemolysis (hemoglobin 9.4 g/dl without
during the acute phase of HUS, with bilateral and
schizocytes, platelet 220 × 109/l) or severe hypertension.
symmetrical thalami, brainstem, and deep white matter
The second brain MRI, 6 days after admission, was normal.
involvement but with diffusion weighted imaging
EEG was similar to the previous one, with posterior
Bilateral basal ganglia involvement is characterized by
abnormalities that could be consistent with reversible
hypersignal on T2-weighted and hypo-signal on T1-
posterior leukoencephalopathy syndrome (RPLS). He re-
weighted images, sometimes extending to the surrounding
ceived antiepileptic medication (Levetiracetam).
white matter [–Thalami and brainstem involvement
Eight months later, he had a third episode of seizures,
have also been described [, Although these lesions
with decreased hemoglobin level (10 g/dl) without schizo-
appear to be fairly characteristic of HUS, the pathogenic
cytes, low but detectable haptoglobin of 0.18 g/l, and
mechanism remains incompletely understood [
moderate thrombocytopenia (platelets 98 × 109/l). High
In our patient presenting with atypical HUS, the MRI
blood pressure persisted, despite bilateral nephrectomy,
features were not consistent with the diagnosis of posterior
Fig. 1 Brain MRI 2 days afterthe third seizures episode. a–c
Axial T2-weighted sequences,b–d coronal FLAIR sequences,a, b bilateral cerebral pedunculahypersignal (arrows), c, dbilateral hypersignal of caudatenuclei (1), putamens (2) andthalami (3)
reversible encephalopathy syndrome, although clinical and
similar neurological events were secondary to three
biological data were suggestive of hypertensive complica-
independent causes. We may hypothesize a delay between
tions. The MRI lesions were similar to those observed in
clinical signs and radiological images or a lack of MRI
typical HUS, suggesting a HUS relapse because the patient
sensitivity. Thus, the normality of the fourth MRI does not
displayed the characteristic bilateral and symmetrical basal
rule out the persistence of brain TMA lesions, but the
ganglia involvement described in the literature, with
disappearance of the MRI hyperintensities observed after
brainstem and thalami lesions also reported in a few
the third burst of seizures is reassuring.
publications. The similarity of radiological lesions between
We report the first case of atypical HUS with cerebral
typical and atypical HUS favors a common pathogenesis,
MRI images suggestive of TMA. In our patient, the genetic
i.e. cerebral thrombotic microangiopathy. In typical HUS
analyses found a hybrid CFH/CFHL1 gene. Similar to CFH
(post-diarrhea HUS), it has been suggested that vascular
point mutations, this hybrid gene is a susceptibility factor
endothelial injury caused by Stx plays a crucial role in the
for atypical HUS [Venables et al. ] described a
development of neurological involvement , Since
pedigree of eight individuals from four generations of
the MRIs following the first and the second seizures were
atypical HUS segregating with this hybrid CFH/CFHL1
normal, we cannot exclude other etiologies for the two first
gene. Two displayed neurological symptoms: grand mal
episodes, such as drug side effects (anesthetics, antibiotics)
convulsion in a 19-year-old woman who died 8 weeks after
or a hypertensive peak. However, drug doses were adapted
presentation and a short history of headaches and lethargy
to renal function, blood pressure was normal at the time of
in a 28-year-old man. However, no imaging details are
the seizures, and it seems very unlikely that the three
provided. The prevalence of neurological involvement in
this family with a hybrid CFH is not higher than that of
6. Barnett ND, Kaplan AM, Bernes SM, Cohen ML (1995)
other CFH mutation-related HUS, suggesting that the
Hemolytic uremic syndrome with particular involvement of basalganglia and favorable outcome. Pediatr Neurol 12:155–158
neurological involvement is secondary to the thrombotic
7. DiMario FJ Jr, Bronte-Stewart H, Sherbotie J, Turner ME (1987)
microangiopathy and not a consequence of the genetic
Lacunar infarction of the basal ganglia as a complication of
defect. A larger number of patients with a hybrid CFH/
hemolytic-uremic syndrome. MRI and clinical correlations. Clin
CFHL1 gene is needed to confirm this hypothesis. Brain
8. Hager A, Staudt M, Klare B, von Einsiedel HG, Krageloh-Mann I
MRI findings were very useful to guide diagnosis and
(1999) Hemolytic-uremic syndrome with involvement of basal
therapeutic strategy in our patient, as it led to the diagnosis
ganglia and cerebellum. Neuropediatrics 30:210–213
of an HUS relapse rather than hypertensive encephalopathy.
9. Jeong YK, Kim IO, Kim WS, Hwang YS, Choi Y, Yeon KM
This was confirmed by the successful intensive plasma-
(1994) Hemolytic uremic syndrome: MR findings of CNScomplications. Pediatr Radiol 24:585–586
therapy with complete clinical and radiological remission,
10. Nakamura H, Takaba H, Inoue T, Saku Y, Saito F, Ibayashi S,
although blood pressure had remained uncontrolled.
Fujishima M (2003) MRI findings of hemolytic uremic syndrome
In conclusion, brain MRI allows the differentiation of
with encephalopathy: widespread symmetrical distribution. J
thrombotic microangiopathy lesions from a hypertensive
11. Ogura H, Takaoka M, Kishi M, Kimoto M, Shimazu T, Yoshioka
complication such as RPLS in patients with atypical HUS
T, Sugimoto H (1998) Reversible MR findings of hemolytic
and neurological manifestations. Therapeutic implications
uremic syndrome with mild encephalopathy. AJNR Am J Neuro-
are important, since treatment would consist of blood
pressure control in one case and intensive plasmatherapy
12. Signorini E, Lucchi S, Mastrangelo M, Rapuzzi S, Edefonti A,
Fossali E (2000) Central nervous system involvement in a child
in the other case. An accurate diagnosis of neurological
with hemolytic uremic syndrome. Pediatr Nephrol 14:990–992
involvement is particularly important as lesions may be
13. Steinborn M, Leiz S, Rudisser K, Griebel M, Harder T, Hahn H
reversible after appropriate treatment.
(2004) CT and MRI in haemolytic uraemic syndrome with centralnervous system involvement: distribution of lesions and prognos-tic value of imaging findings. Pediatr Radiol 34:805–810
14. Theobald I, Kuwertz-Broking E, Schiborr M, Heindel W (2001)
Central nervous system involvement in hemolytic uremic syn-drome (HUS)—a retrospective analysis of cerebral CT and MRIstudies. Clin Nephrol 56:S3–S8
1. Eriksson KJ, Boyd SG, Tasker RC (2001) Acute neurology and
15. Toldo I, Manara R, Cogo P, Sartori S, Murer L, Battistella PA,
neurophysiology of haemolytic-uraemic syndrome. Arch Dis
Laverda AM (2009) Diffusion-weighted imaging findings in
hemolytic uremic syndrome with central nervous system involve-
2. Chou MC, Lai PH, Yeh LR, Li JY, Yuan MK, Liang HL, Chen C,
Pan HB, Lo YK, Yang CF (2004) Posterior reversible encepha-
16. Casey SO, Sampaio RC, Michel E, Truwit CL (2000) Posterior
lopathy syndrome: magnetic resonance imaging and diffusion-
reversible encephalopathy syndrome: utility of fluid-attenuated
weighted imaging in 12 cases. Kaohsiung J Med Sci 20:381–388
inversion recovery MR imaging in the detection of cortical and
3. Gomez-Lado C, Martinon-Torres F, Alvarez-Moreno A, Eiris-
subcortical lesions. AJNR Am J Neuroradiol 21:1199–1206
Punal J, Carreira-Sande N, Rodriguez-Nunez A, Castro-Gago M
17. Ren J, Utsunomiya I, Taguchi K, Ariga T, Tai T, Ihara Y,
(2007) Reversible posterior leukoencephalopathy syndrome: an
Miyatake T (1999) Localization of verotoxin receptors in nervous
infrequent complication in the course of haemolytic-uremic
18. Takahashi K, Funata N, Ikuta F, Sato S (2008) Neuronal apoptosis
4. Bas DF, Oguz KK, Topcuoglu MA (2008) Atypical reversible
and inflammatory responses in the central nervous system of a
posterior leukoencephalopathy syndrome in thrombotic thrombo-
rabbit treated with Shiga toxin-2. J Neuroinflammation 5:11
cytopenic purpura. Intern Med 47:1931–1934
19. Venables JP, Strain L, Routledge D, Bourn D, Powell HM,
5. Kato A, Suzuki Y, Fujigaki Y, Yamamoto T, Yonemura K,
Warwicker P, Diaz-Torres ML, Sampson A, Mead P, Webb M,
Miyajima H, Hishida A (2002) Thrombotic thrombocytopenic
Pirson Y, Jackson MS, Hughes A, Wood KM, Goodship JA,
purpura associated with mixed connective tissue disease. Rheu-
Goodship TH (2006) Atypical haemolytic uraemic syndrome
associated with a hybrid complement gene. PLoS Med 3:e431
CHAPTER 5: SAMPLE PROBLEMS FOR HOMEWORK, CLASS OR EXAMS These problems are designed to be done without access to a computer, but they may require a calculator. 1. For each scenario below, choose the most likely method of analysis and write the corresponding letter in the blank. #1 two-sample t test #5 McNemar’s test #6 two-sample test for medians A. ___ Household incomes are often extremel
de otros comportamientos antisociales y/o violentos “¿Qué hago si mi hijo está molestando o más graves. Los niños que frecuentemente molestan intimidando a otros?” Niños Que Molestan o Intimidan o intimidan a sus pares son más proclives que otros a:• Aclárele a su hijo que usted toma seriamente losactos de molestia o intimidación y que no tolerará (Children Who Bully)
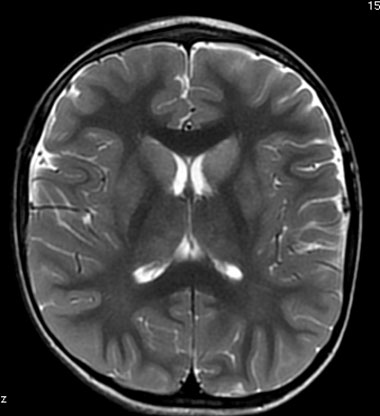
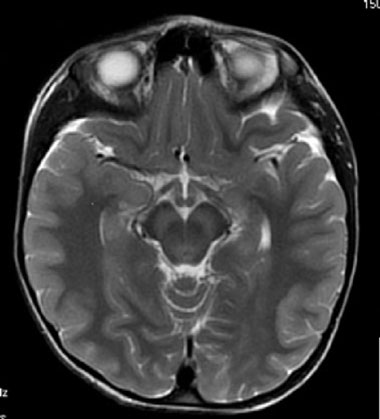

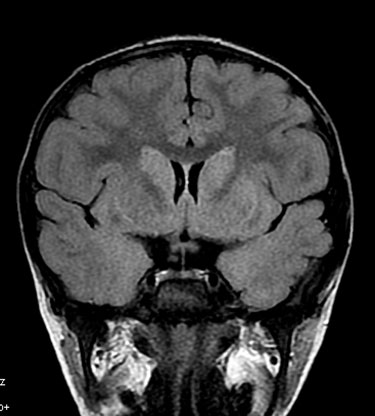 Fig. 1 Brain MRI 2 days afterthe third seizures episode. a–c
Axial T2-weighted sequences,b–d coronal FLAIR sequences,a, b bilateral cerebral pedunculahypersignal (arrows), c, dbilateral hypersignal of caudatenuclei (1), putamens (2) andthalami (3)
reversible encephalopathy syndrome, although clinical and
similar neurological events were secondary to three
biological data were suggestive of hypertensive complica-
independent causes. We may hypothesize a delay between
tions. The MRI lesions were similar to those observed in
clinical signs and radiological images or a lack of MRI
typical HUS, suggesting a HUS relapse because the patient
sensitivity. Thus, the normality of the fourth MRI does not
displayed the characteristic bilateral and symmetrical basal
rule out the persistence of brain TMA lesions, but the
ganglia involvement described in the literature, with
disappearance of the MRI hyperintensities observed after
brainstem and thalami lesions also reported in a few
the third burst of seizures is reassuring.
Fig. 1 Brain MRI 2 days afterthe third seizures episode. a–c
Axial T2-weighted sequences,b–d coronal FLAIR sequences,a, b bilateral cerebral pedunculahypersignal (arrows), c, dbilateral hypersignal of caudatenuclei (1), putamens (2) andthalami (3)
reversible encephalopathy syndrome, although clinical and
similar neurological events were secondary to three
biological data were suggestive of hypertensive complica-
independent causes. We may hypothesize a delay between
tions. The MRI lesions were similar to those observed in
clinical signs and radiological images or a lack of MRI
typical HUS, suggesting a HUS relapse because the patient
sensitivity. Thus, the normality of the fourth MRI does not
displayed the characteristic bilateral and symmetrical basal
rule out the persistence of brain TMA lesions, but the
ganglia involvement described in the literature, with
disappearance of the MRI hyperintensities observed after
brainstem and thalami lesions also reported in a few
the third burst of seizures is reassuring.