Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Oral histoplasmosis associated with hiv infection: a comparative study
J Oral Pathol Med (2004) 33: 445–50ª Blackwell Munksgaard 2004 Æ All rights reserved
Oral histoplasmosis associated with HIV infection:a comparative study
S. L. Herna´ndez1, S. A. Lo´pez de Blanc1,2, R. H. Sambuelli3,4, H. Roland3, C. Cornelli3, V. Lattanzi1,M. A. Carnelli4
1Clinical Stomatology B, School of Dentistry, National University of Co´rdoba, Co´rdoba; 2Department of Oral Pathology, HeadProfessor of Clinical Stomatology B, Faculty of Dentistry, National University of Co´rdoba, Co´rdoba; 3Rawson Hospital Co´rdoba,Co´rdoba; 4Department of Pathology, Catholic University of Co´rdoba, Co´rdoba, Argentina
OBJECTIVE: Histoplasmosis is a granulomatous fungal
river valleys of the world between latitudes 45° north
disease caused by Histoplasma capsulatum. The objective
and 30° south of the equator (1, 4, 6–15). In Argentina,
of the present paper was to describe the prevalence
the endemic region is around the central, east and
of oral histoplasmosis (OH) in two services from an
endemic area in Argentina between 1991 and 2002 and to
Clinically, histoplasmosis has been classified as: (i) a
compare the clinicopathological profile of OH between
primary acute pulmonary form, (ii) a chronic pulmonary
HIV-positive and HIV-negative patients.
and (iii) a disseminated form (DH) occurring in infants,
METHODS: About 733 HIV+ (group A) and 14 260
elderly or in immunocompromised patients (6, 19–23).
patients (group B) were examined. Clinical diagnosis was
In 1985, the Centre for Disease Control added DH to
confirmed by cytology, biopsy or culture.
the spectrum of infections that characterize the acquired
RESULTS: About 21 (3%) and 10 (0.07%) cases of OH
immunodeficiency syndrome (AIDS). The main reason
were diagnosed in group A and B respectively. Most
for the delay in recognizing histoplasmosis as an
patients were male. A total of 90% of patients in group A
opportunistic infection in those patients was that early
were <45 years old whereas 70% of group B were more
AIDS cases appeared first in non-endemic areas. With
than 45 years old. Palate, gingiva and oropharynx were
spread of the disease to endemic areas, it has emerged as
the most frequent locations. The importance of including
an important opportunistic infection in patients with
histoplasmosis in the differential diagnosis of ulcerated
AIDS (8, 9, 24, 25). About 30–66% of patients with DH
have oral lesions, frequently presenting as the initial
sign. Generally lesions of histoplasmosis in the oral
cavity, are the local manifestation of pulmonary ordisseminated disease (16, 26) but rarely they may be the
Keywords: histoplasmosis; human immunodeficiency virus; oral
primary or even the only manifestation of the disease
(3, 4, 8, 10, 16, 17, 27–29). The diagnosis is usually basedon clinical signs and symptoms, organ function tests andfungal demonstration or culture from a lesion orsecretion. Serological testing may help together with
other suggestive but non-diagnostic clinical criteria (4–6,
Histoplasmosis is a granulomatous fungal disease of
11, 17). Recently, molecular typing of H. capsulatum has
worldwide distribution caused by Histoplasma capsula-
been shown to be useful in distinguishing relapse from
tum. The infecting agents are airborne spores from the
reinfection, and in defining the likely source of the
mycelial form. It is usually found in warm, humid
infection (21, 30, 31). Furthermore, molecular typing of
environments that contain bird and bat excreta (1–7).
H. capsulatum by the random amplified polymorphic
The most endemic areas for H. capsulatum are certain
method, is able to discriminate among clinical iso-lates, making it a useful tool for epidemiological investi-
Dra Silvia Lo´pez de Blanc, Ca´tedra de Clı´nica
Estomatolo´gica I y II B, Facultad de Odontologı´a, Pabello´n Argen-tina, Ciudad Universitaria, Agencia 4, (5016) Co´rdoba, Argentina.
Tel: 0351-4659564, Fax: 0351-4334179-78, E-mail: silopez@odo.unc.
Historically, amphotericin B has been the drug of choice
edu.ar, lopezdeblanc@yahoo.com.arAccepted for publication March 11, 2004
for systemic histoplasmosis (1–3, 8, 12, 16, 17, 32–37).
The options have broadened considerably since the
CD4 count in HIV+ patients was 60/mm3 and ranged
introduction of the azole compounds, ketoconazole and
Oral lesions had similar clinical presentation in both
The aim of the present paper is to describe the
groups, described as painful granulomatous ulceration.
prevalence of OH in two services from an endemic area
The lesions began as erythematous, painful red patches
in Argentina and to compare the clinicopathological
(see Fig. 1) that latter became elevated, granulomatous
profile of histoplasmosis oral lesions of HIV-infected
and ulcerated as shown in Fig. 2. The ulcerations were
(HIV+) and HIV-negative (HIV)) patients.
covered by yellowish pseudomembranes difficult toremove and tender to palpation. Most of the patientsin both groups, had more than two lesions. The most
frequent locations were hard and soft palate, gingiva
In this retrospective study, the clinical records made by
and oropharynx, followed by tongue. Gingival lesions
us in HIV+ patients of Rawson Hospital: group A, and
were associated with bone loss. Presence of histoplas-
in those attended in Clinical Stomatology B (a referral
mosis was diagnosed by cytology, culture, biopsy or
clinic for oral soft-tissue lesions): group B, between
December 1991 and December 2002 were revised inorder to analyse and compare the prevalence of OH in
both groups. Group A included 733 patients and group
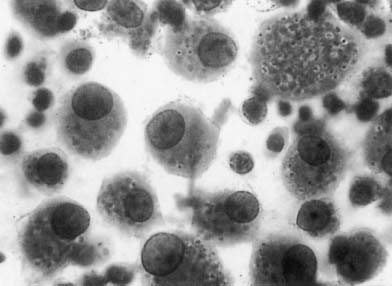
Yeast forms were quite easily visualized in cytological
B 14 260. Written consent was obtained from each
smears or biopsies. The smears revealed in addition to
patient before the study; oral examinations and the
squamous cells of the oral mucosa, several erythrocytes,
diagnosis at both centres were made by the same trained
neutrophils and macrophages-containing intracellular
professionals and supervised by the head professor. All
spherical to ovoid bodies each surrounded by a small
the patients with OH were tested for HIV infection and
light halo (Fig. 3). Biopsy specimens showed a normal
the HIV-positive excluded of group B. When an
maturing, thinly stretched and ulcerated stratified squ-
ulcerated granulomatous lesion suggesting OH was
amous epithelium. The lamina propia showed focal
found, the diagnosis was based on the demonstration
accumulations of mononuclear macrophages stuffed
of the microorganism in biopsies, cytological smears or
with 2–5 micron fungal yeasts and some isolated
culture (4–7, 11, 16). Biopsies were stained with haem-
organisms that stained highly positive with PAS and
atoxylin and eosin and with periodic acid-Schiff (PAS)
1 GSM. Yeast forms were seen intracellularly within the
stain reaction; in some cases the Grocott silver methen-
histiocytes, and as described in the literature, they had a
amine (GSM) procedure was used. Cytological smears
thin wall instead of a true capsule (39). The ulcerated
were stained with May Gru¨ndwald Giemsa (MGG) and
surface was coated with fibrin and the area beneath the
with Papanicolaou stain (EA36-Hematoxylin). Addi-
ulcer showed a moderate acute inflammatory infiltrate.
tional confirmation was obtained by isolation and
Several small microorganisms, with frequent transepi-
identification of the organism from tissue or secretion
thelial migration were found in group A, whereas in
cultures. The tissue was added to the following media:
group B they were scarce but more voluminous. On the
Sabouraud dextrose agar + chloramphenicol, ampicil-
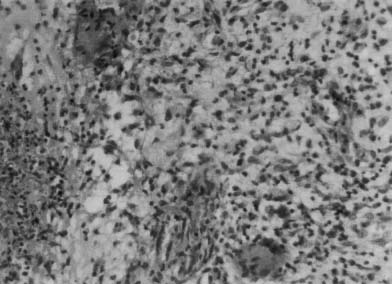
contrary, conspicuous granulomas with giant cells were
lin and gentamicin. The tubes were incubated at 28°C
observed in HIV) patients (Fig. 4), whereas in group A
to observe the mycelial and at 35°C to observe the
they were exceptional. Vasculitis phenomena were
levaduriform or infecting form. Positive colonies were
occasionally observed. Cultures were positive in seven
then transferred to blood agar plates and incubated at
35°C, eventually resulting in conversion to the yeast
The OH was marker disease in 10 HIV+ patients
form. The diagnosis was confirmed by the dimorphism
(48%). The treatment was dependant on the immuno-
logical condition of the patient, and on the availabilityof drugs in our public hospital. In 14 cases of the groupA the treatment begun with amphotericin B, and when
the infection was controlled, an azole antifungal was
In group A (HIV+ patients), 21 (3%) had OH, while
used; in six cases it was controlled only with itracon-
in group B (HIV)) only 10 (0.07%) did. The analysed
azole. This was the drug of choice in group B. The
data on age, gender, general condition, other involve-
evolution was good in all patients but three of group A
ment and diagnosis of these patients are shown in
relapsed some months later, only two died after therapy
Table 1. The age ranged from 23 to 77 years. Nineteen
but histoplasmosis was not the cause of death.
patients (90%) in group A, were <45 years oldwhereas seven (70%) in group B were more than
45 years old, indicating a positive correlation betweenage and HIV infection in patients with OH (P ¼ 0.001,
Most investigators believe that human infection occurs
Fisher’s exact test). Most of the patients were male,
via inhalation of aleuriospores in dust (5, 6, 15). Ritter
81% in group A and 90% in group B. Weight loss
(40) and Gordon et al. (41), however, suggest that at
followed by persistent cough and dysphagia, were the
least in some instances the spores gain entry to the
most frequent symptoms in both groups; in addition,
gastrointestinal tract from contaminated drinking water.
67% of the HIV+ patients had fever. The average of
On the contrary, some investigators claim that primary
Oral histoplasmosis in HIV+ patientsHerna´ndez et al.
Clinical features of an HIV+ patient. Red patch involved
Cytological smear from an HIV+ patient, showing several
the marginal and attached gingiva of the anterior area; ulcerated
macrophages containing intracellular spherical to ovoid bodies, each
lesions of the premolar area are also present.
surrounded by a small light halo (papanicolaou stain, originalmagnification ·100).
Clinical features of an HIV patient showing an elevated
granulomatous lesion in hard palate and right maxillary gingiva.
Biopsy specimen showing a granulomatous suppurated
lesion from an HIV patient and the Histoplasma capsulatum within a
OH is possible and may occur from direct inoculation of
giant cell (haematoxylin and eosin stain, original magnification ·60).
the fungus into the mucosa (4, 5, 24). The possibility ofhuman-to-human transmission between sexual partnersis still an intriguing question (42). In the cases analysed
among females was found in HIV+ patients, a
in this paper OH lesions were found 43 times more
tendency also observed by Casariego et al. (45). Most
frequently in HIV+ vs. HIV) patients; in addition all
patients had a favourable response to the therapy; only
the HIV) patients lived on a farm or worked in contact
two died after therapy but histoplasmosis was not the
with bird and bat excreta, whereas it was very difficult
to establish the source of contamination in HIV+
This report shows the importance of including OH in
patients. Clinical presentation and location of the oral
the differential diagnosis of ulcerated lesions in immu-
lesions as well as the average of CD4 count (60/mm3)
nocompromised patients. Early recognition and prompt
were similar to those reported by other authors (11,
management of these infections are of paramount
32). Although histoplasmosis is a disease that tradi-
importance in maintaining the health and prolonging
tionally affects old people (12, 16), since the appearance
of AIDS its prevalence has increased in younger peopleas in the present study (32, 43, 44). From these resultsit can be inferred that if histoplasmosis is diagnosed
in a young patient, then a search for current HIV
1. Miller RL, Gould AR, Skolnick JL, Epstein WM.
infection is justified. A higher prevalence among males
Localized oral histoplasmosis: a regional manifestation
was observed, as previously reported (4, 32, 44–47);
of mild chronic disseminated histoplasmosis. Oral Surg
nevertheless in this paper an increase in the prevalence
Oral Med Oral Pathol 1982; 53: 367–74.
Oral histoplasmosis in HIV+ patientsHerna´ndez et al.
2. Boutros HH, van Winckle RB, Evans GA, Wasan SM.
national reporting-United States. MMWR 1985; 34:
Oral histoplasmosis masquerading as an invasive carci-
noma. J Oral Maxillofac Surg 1995; 53: 1110–4.
25. Heinic GS, Greenspan D, Macphail LA, et al. Oral
3. Reddy P, Gorelick DF, Brasher CA, Larsh H. Progressive
Histoplasma capsulatum infection in association with
disseminated histoplasmosis as seen in adults. Am J Med
infection: a case report. J Oral Pathol Med 1992; 21:
4. Joklik WK, Willett HP, Amos B, Wilfert CM. Zinsser
26. Loh FC, Yeo JF, Tan WC, Kumarasinghe G. Histoplas-
Microbiologı´a, 20th edn. Buenos Aires: Me´dica Panamer-
mosis presenting as hyperplastic gingival lesion. J Oral
5. Negroni M. Microbiologı´a Estomatolo´gica Fundamentos y
27. Fowler CB, Nelson JF, Henley DW, Smith BR. Acquired
guı´as pra´cticas. Buenos Aires: Me´dica Panamericana,
immune deficiency syndrome presenting as a palatal
perforation. Oral Surg Oral Med Oral Pathol 1989; 67:
6. Bullock WE. Histoplasma capsulatum. In: Mandell GL,
Bennett JE, Dolin R, eds. Principles and practice of
28. Swindells S, Durham T, Johansson SL, Kaufman L. Oral
infectious diseases, 4th edn. New York: Churchill Living-
case report. Oral Surg Oral Med Oral Pathol 1994; 77:
7. Goodwin RA, des Prez RM. Histoplasmosis. State of the
art. Am Rev Respir Dis 1978; 117: 929–56.
29. Young SK, Rohrer MD, Twesmw AT. Spontaneous
8. Chinn H, Chernoff DN, Migliorati CA, Silverman S,
regression of oral histoplasmosis. Oral Surg 1971; 52:
Green TL. Oral histoplasmosis in HIV-infected patients: a
report of two cases. Oral Surg Oral Med Oral Pathol Oral
30. Wheat J, Marichal P, van den Bossche H, Le Monte A,
Connolly P. Hypothesis on the mechanism of resistance to
9. Oda D, McDougal L, Fritsche T, Worthington P. Oral
fluconazole in Histoplasma capsulatum. Antimicrob Agents
histoplasmosis as a presenting disease in acquired immu-
nodeficiency syndrome. Oral Surg Oral Med Oral Pathol
31. Eath EJ, Kobayashi GS, Medoff G. Typing of Histo-
plasma capsulatum by restriction fragment length poly-
10. Casariego Z, Kelly GR, Perez H, et al. Disseminated
morphisms in a nuclear gene. J Clin Microbiol 1992; 30:
histoplasmosis with orofacial involvement in HIV-I-infec-
ted patients with AIDS: manifestations and treatment.
32. Economopoulou P, Laskaris G, Kittas C. Oral histoplas-
mosis as an indicator of HIV infection. Oral Surg Oral
11. Kirchner JT. Opportunistic fungal infections in patients
Med Oral Pathol Oral Radiol Endod 1998; 86: 203–6.
with HIV disease: combating cryptococcosis and histo-
33. Go´mez BL, Figueroa JL, Hamilton AJ, et al. Detection
plasmosis. Postgraduate Med 1996; 99: 209–16.
of the 70-kilodalton Histoplasma capsulatum antigen in
12. Cobb CM, Shultz RE, Brewer JH, Dunlap CL. Chronic
serum of histoplasmosis patients: correlation between
pulmonary histoplasmosis with an oral lesion. Oral Surg
antigenemia and therapy during follow-up. J Clin
Oral Med Oral Pathol 1989; 67: 73–6.
13. Laskaris G. Oral manifestations of infectious diseases.
34. Sarosi GA, Voth DW, Dahl BA, Doto IL, Tosh FE.
Dent Clin North Am 1996; 40: 395–423.
Disseminated histoplasmosis: results of long-term follow-
14. Scully C, Almeida OPD, Warnakulasuriya KAAS, John-
son NW. Orofacial involvement buy systemic mycoses in
35. Margiotta V, Campisi G, Mancuso S, Accurso V, Abadesa
HIV infection. Oral Dis 1995; 1: 61–2.
V. HIV infection: oral lesions, CD4+ cell count and viral
15. Kok Han NG, Chong Huat SIAR. Review of oral
load in an Italian study population. J Oral Pathol Med
histoplasmosis in Malaysians. Oral Surg Oral Med Oral
Pathol Oral Radiol Endod 1996; 81: 303–7.
36. Eisig S, Boguslaw B, Cooperband B, Phelan J. Oral
16. Grinspan D. Enfermedades la Boca. Semiologı´a, Patologı´a,
manifestations of disseminated histoplasmosis in acquired
Clı´nica y Terape´utica de la Mucosa Bucal: Tomo II. Buenos
immunodeficiency Syndrome: report of two cases and
review of the literature. J Oral Maxillofac Surg 1991; 49:
17. Lynch MA. Medicina Bucal de Burket: diagno´stico y
tratamiento. Mexico: Interamericana, 1986; 191.
37. Chimenos E, Puy D, Lo´pez J. Fa´rmacos antifu´ngicos
18. Wheat J. Histoplasmosis: recognition and treatment. Clin
utilizados en el tratamiento de las micosis. Med Oral 1998;
19. Smith JW, Utz JP. Progressive disseminated histoplasmo-
38. Brooks JT, Wheat J. Histoplasmosis: update 1998. AIDS
sis. A prospective study of 26 patients. Ann Int Med 1972;
39. Koeman E, Allen S, Janda W, et al. Colour atlas and
20. Cobb C, Schultz R, Brewer J, et al. Chronic pulmonary
textbook of diagnostic microbiology. Philadelphia, PA:
histoplasmosis with an oral lesion. Oral Surg Oral Med
40. Ritter C. Studies of the viability of Histoplasma capsula-
21. Limaye AP, Connolly PA, Sagar M, et al. Brief Report:
tum in tap water. Am J Pub Health 1959; 44: 1299.
Transmission of Histoplasma capsulatum by organ trans-
41. Gordon MA, Ajello L, George LK, Reidberg LD.
plantation. N Engl J Med 2000; 343: 1163–66.
Microsporum gypseum and Histoplasma capsulatum in soil
22. Wheat LJ, Slama TG, Norton JA, et al. Risk factors for
disseminated or fatal histoplasmosis. Analysis of a large
42. Cohen PR, Held JL, Grossman ME, Ross MJ, Silvers DN.
urban outbreak. Ann Int Med 1982; 96: 159–63.
Disseminated histoplasmosis presenting as an ulcerated
23. Hiltbrad J, Mcguirt W, Winston-Sale N. Oropharyngeal
verrucous plaque in a human immunodeficiency virus-
histoplasmosis. South Med J 1990; 83: 227.
infected man: report of a case possibly involving human-
24. Center for Disease Control. Revision of the case defini-
to-human transmission of histoplasmosis. Int J Dermatol
43. Souza Filho FJ, Lopez M, Almeida OP, Scully C.
46. Warnakulasuriya KAAS, Harrison JD, Jonson NW,
Mucocutaneous histoplasmosis in AIDS. Br J Dermatol
Edwars S, Taylor C, Pozniak AL. Localised oral histo-
plasmosis lesions associated with HIV infection. J Oral
44. Swindells S, Durham T, Jhansson SL, Kaufman L. Oral
histoplasmosis in a patient infected with HIV: a case
47. Cohen PR. Oral histoplasmosis in HIV infected patients.
report. Oral Surg Oral Med Oral Pathol 1994; 77: 126–
Oral Surg Oral Med Oral Pathol 1994; 78: 277–8.
45. Casariego Z, Ben G. Manifestaciones bucales de la
infeccio´n por VIH en Argentina: estudio de 1889 casos. Medicina Oral 1998; 3: 271–6.
Soft X-ray Emission and Lithium Production in Cen X-4 duringShin-ichiro Fujimoto,1 Ryuichi Matsuba,2 and Kenzo Arai,31 Department of Electronic Control, Kumamoto National College of Technology,2659-2 Suya, Koshi, Kumamoto 861-1102, Japan2 Institute for e-Learning Development, Kumamoto University, Kumamoto 860-8555, Japan3 Department of Physics, Kumamoto University, Kumamoto 860-8555, Japan E
CLADES, CAPGRAS, AND PERCEPTUAL KINDS Jack Lyons University of Arkansas Perceptual states represent the world as being certain ways, as having certain properties. Which ways and properties are these? When I hold out my hand and look at it, it seems that Ihave a visual experience of a hand. One traditional view has held that my perceptual state is notof a hand but merely of an array of colo


 Clinical features of an HIV+ patient. Red patch involved
Cytological smear from an HIV+ patient, showing several
the marginal and attached gingiva of the anterior area; ulcerated
macrophages containing intracellular spherical to ovoid bodies, each
lesions of the premolar area are also present.
Clinical features of an HIV+ patient. Red patch involved
Cytological smear from an HIV+ patient, showing several
the marginal and attached gingiva of the anterior area; ulcerated
macrophages containing intracellular spherical to ovoid bodies, each
lesions of the premolar area are also present.