Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Glucosamine sulfate in the treatment of knee osteoarthritis symptoms: a randomized, double-blind, placebo-controlled study using acetaminophen as a side comparator
Vol. 56, No. 2, February 2007, pp 555–567
2007, American College of Rheumatology
A Randomized, Double-Blind, Placebo-Controlled Study Using Acetaminophen as
´n Ivorra,2 Marı´a del Carmen Trabado,3
Francisco Javier Blanco,4 Pere Benito,5 Emilio Martı´n-Mola,6 Javier Paulino,7
´ Luis Marenco,8 Armando Porto,9 Armando Laffon,10 Domingos Arau
Objective. To assess the effects of the prescription 108), or placebo (n ؍ 104). The primary efficacy out- formulation of glucosamine sulfate (1,500 mg adminis- come measure was the change in the Lequesne index tered once daily) on the symptoms of knee osteoarthritis after 6 months. Secondary parameters included the (OA) during a 6-month treatment course. Western Ontario and McMaster Universities Osteoar- Methods. Three hundred eighteen patients were thritis Index (WOMAC) and response according to the enrolled in this randomized, placebo-controlled, double- Osteoarthritis Research Society International criteria. blind trial in which acetaminophen, the currently pre- These outcome measures were assessed using an intent- ferred medication for symptomatic treatment of OA, to-treat analysis. was used as a side comparator. Patients were randomly Results. At baseline, the study patients had mod- assigned to receive oral glucosamine sulfate 1,500 mg erately severe OA symptoms (mean Lequesne index ϳ11 once daily (n ؍ 106), acetaminophen 3 gm/day ( n ؍ points). Glucosamine sulfate was more effective than placebo in improving the Lequesne score, with a final
ClinicalTrials.gov identifier: NCT00110474. decrease of 3.1 points, versus 1.9 with placebo (differ- ence between glucosamine sulfate and placebo [95% confidence interval ؊2.3, ؊0.8]) (P ؍ 0.032). The
Peset, Valencia, Spain; 3Marı´a del Carmen Trabado, MD: Hospital
2.7-point decrease with acetaminophen was not signifi-
Clinic, Barcelona, Spain; 4Francisco Javier Blanco, MD: HospitalUniversitario Juan Canalejo, A Corun
cantly different from that with placebo (difference ؊0.8
Hospital del Mar, Barcelona, Spain; 6Emilio Martı´n-Mola, MD:
[95% confidence interval ؊1.9, 0.3]) (P ؍ 0.18). Similar
Hospital Universitario La Paz, Madrid, Spain; 7Javier Paulino, MD:
results were observed for the WOMAC. There were more
Completo Hospitalario De Ciudad Real, Ciudad Real, Spain; 8Jose
responders to glucosamine sulfate (39.6%) and acet-
Spain; 9Armando Porto, MD: Hospital Universitario Coimbra, Portu-
aminophen (33.3%) than to placebo (21.2%) (P ؍ 0.004
gal; 10Armando Laffon, MD: Hospital De La Princesa, Madrid, Spain;11Domingos Arau´jo, MD: Hospital Conde de Bertiandos, Ponte de
and P ؍ 0.047, respectively, versus placebo). Safety was
Lima, Portugal; 12Manuel Figueroa, MD: Hospital Donostia, San
good, and was comparable among groups.
Sebastian, Spain; 13Jaime Branco, MD: Centro Hospitalar de Lisboa
Conclusion. The findings of this study indicate
Occidental, EPE/Hospital Egas Moniz, Lisbon, Portugal.
Dr. Herrero-Beaumont has received speaking fees (less than
that glucosamine sulfate at the oral once-daily dosage of 1,500 mg is more effective than placebo in treating
Address correspondence and reprint requests to Gabriel
knee OA symptoms. Although acetaminophen also had
Herrero-Beaumont, MD, Rheumatology Department, Fundacio
´nez Dı´az-Capio, Autonomous University of Madrid, Avenida
a higher responder rate compared with placebo, it
Reyes Catolicos 2, 28040 Madrid, Spain. E-mail: gherrero@fjd.es. failed to show significant effects on the algofunctional
Submitted for publication May 16, 2006; accepted in revised
indexes.
Current treatment options for osteoarthritis
PATIENTS AND METHODS
(OA) include both nonpharmacologic and pharmaco-
Study design. The GUIDE trial was conducted accord-
logic interventions (1,2). Published evidence-based rec-
ing to a prospective, randomized, placebo- and reference-
ommendations for the treatment of knee OA (3) have
controlled, double-blind, double-dummy, parallel-group de-
attributed to oral glucosamine sulfate the highest level of
sign, in 13 rheumatology referral centers in Spain and Portugal.
evidence and strength of recommendation as a pharma-
The study protocol was approved by the institutional reviewboard of each participating center, and patients provided their
cologic intervention, acknowledging the high quality of
written informed consent to participate. During the baseline
the trials performed; only 6 of 34 therapeutic interven-
period after screening, the results of routine laboratory tests
tions considered were ascribed the same degree of
were collected, radiographic assessments were conducted (if
evidence and recommendation as glucosamine sulfate
not performed during the previous 3 months), and symptom-atic medications currently being taken were discontinued.
(3). Two 3-year clinical trials have independently pro-
Patients were then randomly assigned to 1 of the 3 treatment
vided evidence of efficacy in the long-term management
arms, i.e., glucosamine sulfate, acetaminophen, or placebo.
of knee OA symptoms, and their results suggested that
Clinic visits were carried out after 15 days of treatment and
glucosamine sulfate may potentially delay joint structure
then at monthly intervals from the time of randomization until
the end of the 6-month treatment course. Patient selection. Male and female outpatients who
While the glucosamine sulfate substance and
were seen in rheumatology clinics at the participating centers
formulation used in those studies is a prescription drug
were selected if they had been diagnosed as having primary
in continental Europe and elsewhere, many glucosamine
symptomatic knee OA (in 1 or both knees) according to the
salts (e.g., glucosamine hydrochloride), formulations,
clinical and radiographic criteria of the American College ofRheumatology (14), and did not meet standard criteria for
and dosages are available as dietary supplements in the
exclusion (15). Enrollment of patients who were obese (body
US, due to different regulations (6). In some studies
mass index [BMI] Ͼ30 kg/m2) was discouraged by the study
using different glucosamine preparations (7,8), the fa-
protocol, to avoid any bias introduced by this factor. Disease
vorable results in terms of symptom modification ob-
stage was determined based on the Kellgren/Lawrence radio-graphic system (16) (either grade II or grade III as a condition
tained in former trials, in which the prescription formu-
of enrollment), and symptom severity was quantified with the
lation was used, were not replicated. This drew attention
algofunctional indexes selected as outcome measures (see
to the pharmaceutical and pharmacologic differences, as
noted in a recent Cochrane review (9), and to the limita-
Treatment, blinding, and randomization. Crystalline
glucosamine sulfate is a chemically well-characterized pure
tions in study design (10) as possible explanations for the
substance in which glucosamine, sulfate, chloride, and sodium
ions are present in stoichiometric ratios of 2:1:2:2, and it is
Two recent randomized, controlled, double-blind
approved as a prescription drug in Ͼ45 countries (Dona,
trials have assessed the efficacy of different glucosamine
Viartril-S, Xicil, and other trade names of the RottapharmGroup, Monza, Italy); it is also available as a branded dietary
preparations, compared with placebo, in the manage-
supplement in the US (Dona). The product was used in its
ment of knee OA symptoms over a medium-term treat-
once-daily formulation (sachets of powder for oral solution,
ment course. Both studies used an active medication as
containing 1,500 mg of glucosamine sulfate). Acetaminophen
a side comparator. In the Glucosamine/Chondroitin
was administered in 1-gm tablets 3 times per day, for a totaldaily dosage of 3 gm (the recommended daily dosage in
Arthritis Intervention Trial (GAIT study) celecoxib was
used as the side comparator, while in the Glucosamine
Patients receiving either of the 2 active treatments also
Unum In Die (once-a-day) Efficacy (GUIDE) trial
received placebo for the other medication, while controls
acetaminophen was used, the latter being the currently
received double placebo consisting of once-daily sachets and3-times-a-day tablets. The double-dummy placebo formula-
preferred symptomatic medication in OA (2,3). The
tions were identical in appearance to the active medications,
GAIT study was sponsored by the National Institutes of
but contained only inactive excipients. Treatment compliance
Health (NIH) and conducted in the US with glu-
was checked at clinic visits by patient interview and by counting
cosamine hydrochloride at a dosage of 500 mg 3 times
the number of unused doses of the study medications.
A block randomization list was generated by computer
daily, whereas the GUIDE trial is an industry-sponsored
and was maintained by individuals who had no contact with
study conducted in Europe with the glucosamine sulfate
investigators who assigned patients to their randomized treat-
prescription formulation of 1,500 mg once daily. Prelim-
ments, performed any patient assessment, or conducted the
inary results of both studies were presented in 2005
statistical analysis. The block size was also kept secret tomaintain blinding; each block consisted of only 3 patients, to
(11,12), and the GAIT study report was recently pub-
avoid imbalances in treatment allocation at each clinical site.
lished as a full article(13). We report herein the final
Patients were sequentially assigned their randomization num-
ber at each site, and the individual code was kept in single-
sealed, opaque envelopes to be opened only in case of a
physical function subscale), and patient global assessment
medical emergency. Double-blinding conditions were success-
(35%, 15%, and 15% relative changes, with 10, 20, and 15
standardized units of absolute change, respectively).
The pure analgesic acetaminophen was the side com-
Additional efficacy outcomes included the OARSI-B
parator treatment in the GUIDE study, and therefore it could
responder criteria (high degree of improvement in pain or
not be used as a rescue medication as is the common proce-
function, or moderate improvement in 2 of the 3 domains
dure in OA clinical trials (15). Thus, the rescue medication
listed above) (19) and the proportion of patients reporting at
consisted of the conventional nonsteroidal antiinflammatory
least minimal clinically important improvement (MCII) or
drug (NSAID) ibuprofen, in 400-mg tablets. To avoid con-
reaching the patient acceptable symptom state (PASS) in pain
founding in the efficacy assessments, the use of the rescue
and function based on the WOMAC subscales, as recently
medication in case of persistent pain was carefully standard-
ized according to the following sequential instructions: 1) leave
Assessment of safety. Reporting of adverse events was
the painful joint at rest for at least 1 hour; 2) take 1 ibuprofen
elicited with a nonleading question during clinic visits. All
tablet every 8 hours; 3) limit intake to a maximum of 3 days; 4)
events were coded according to the Medical Dictionary for
if needed, resume the rescue medication intake after a washout
Regulatory Activities, as currently required by all regulatory
period of at least 7 days; and 5) in all cases, suspend any use of
authorities including the US Food and Drug Administration
the rescue medication at least 7 days before a clinic visit. The
and the European Agency for the Evaluation of Medicinal
use of rescue ibuprofen was recorded in a patient daily diary.
Products. Routine laboratory tests, including measurement of
Prior analgesic (narcotic and non-narcotic) or antiin-
serum glucose levels for estimating effects on glucose ho-
flammatory symptomatic medications, including topical
meostasis and administration of liver function tests, were
agents, were discontinued for the duration of at least 5
performed at enrollment and after 3 months and 6 months of
half-lives or 72 hours, whichever was longer, before random-
ization and were prohibited during the study. The recom-
Statistical analysis. The primary comparison in this
mended duration of washout prior to randomization was at
study was between glucosamine sulfate and placebo. The
least 3 months for corticosteroids and 6 months for glu-
sample size was calculated on the basis of the difference
cosamine or other drugs considered specific for OA. These and
between glucosamine sulfate and placebo in the change in the
any other agents for the treatment of this condition were
Lequesne index from baseline to end of treatment, which was
prohibited throughout the study. Physical and/or occupational
at least 1 point in previous trials (9,22). With such a simulated
therapy were allowed if the regimen had been stable for at least
difference, a standard deviation of the mean response of 2.25,
a Type I error of 5%, and a Type II error of 20%, a sample size
Assessment of efficacy. The Lequesne algofunctional
of 80 patients per group was calculated (23), and this was
index of severity for OA of the knee (17) was used for sample
increased to at least 100 patients per group to take into
size calculation and was designated as the primary efficacy
account an expected dropout rate of ϳ30%. The size of the
outcome in the GUIDE trial. It is a disease-specific, aggre-
group receiving acetaminophen was also set at 100 patients.
gated multidimensional index consisting of 5 questions ad-
The GUIDE is a regulatory trial agreed upon by the
dressing knee pain, 4 questions on knee function in activities of
sponsor (Rottapharm) and the relevant health authorities.
daily living, and a scale of maximum distance walked. The
Following protocol approval and implementation, the statisti-
worst possible total index score is 24, but disease is considered
cal analysis protocol was planned by the sponsor in June 2001.
extremely severe if the score is Ͼ13 (17). At randomization,
It was amended in December 2004, prior to database lock, only
after washout of previous symptomatic medications, patients
to add the MCII and PASS assessments that had become
had to have a Lequesne score that was at least as high as the
available in the summer of the same year (20,21).
score at the screening visit. For continuation in the study
The primary efficacy analysis performed was assess-
protocol, this score had to be Ն4, corresponding to at least
ment of the difference between groups in the change from
mild-to-moderate disease severity (17).
baseline in the Lequesne index after 6 months, in the intent-
The secondary efficacy end points were the Western
to-treat (ITT) population (i.e., including all randomized pa-
Ontario and McMaster Universities Osteoarthritis Index
tients with at least 1 efficacy assessment after randomization).
(WOMAC) (18) and the Osteoarthritis Research Society
The last observation carried forward (LOCF) approach was
International (OARSI) responder criteria (19). The 0–4-point
used for patients who did not complete the study according to
Likert scale (LK 3.0) WOMAC version was used, addressing
the protocol. A per-protocol completer analysis was also
severity of knee pain (5 questions), limitation of physical
performed. To assess the differences between each of the
function (17 questions), and stiffness (2 questions) in the 48
active groups (glucosamine sulfate or acetaminophen) and
hours before assessment. The worst possible scores on the
placebo, a general linear model approach was applied in
WOMAC subscales are therefore 20, 68, and 8 in the 3
one-way analysis of variance, with treatments as fixed effect
domains, respectively, and can be used to normalize the Likert
and application of Dunnett’s 2-tailed test to adjust for multiple
scores to a 0–100 scale, i.e., similar to a 100-mm visual analog
pairwise comparisons. Results were expressed as the difference
scale (VAS) (18). The OARSI-A responder criteria for oral
between final group means and 95% confidence intervals
OA-specific drugs consist of a dichotomous outcome measure
(adjusted for multiple comparisons). In addition, the magni-
that defines as responders those patients with either a high
tude of each treatment effect was described as effect size, i.e.,
degree of improvement in pain (at least 55% relative change
the difference between the mean change from baseline with
on the WOMAC pain subscale, with an absolute change of at
the active drug and with placebo, divided by the pooled
least 30 on a 0–100 standardized scale) or moderate improve-
standard deviation (24).The same analysis was performed on
ment in 2 of the 3 domains of pain, function (on the WOMAC
the secondary efficacy outcome represented by the WOMAC,
Figure 1. Study profile. ء ϭ patients who agreed to baseline evaluation but did not qualify for randomization. Pl ϭ placebo; Ac ϭ acetaminophen; GS ϭ glucosamine sulfate; ITT ϭ intent-to-treat.
while the difference between each active group and placebo in
patients considered for the study could be randomized.
the proportion of OARSI-A responders in the ITT population
Seven patients did not provide any efficacy data after
was analyzed by 2-tailed chi-square test. The chi-square testwas also used to compare each active group with placebo for
randomization and were not included in the analysis,
the proportion of ITT patients satisfying the additional efficacy
leaving a total of 318 patients in the ITT population
parameters, in the following order: OARSI-B responders, pain
(Figure 1). Twenty-six percent of the patients receiving
MCII, function MCII, pain PASS, and function PASS. To
glucosamine sulfate or acetaminophen did not complete
adjust for the multiplicity represented by the 2 active groupcomparisons with placebo for the dichotomous secondary
the 6-month treatment period according to the study
outcome (OARSI-A) and additional efficacy parameters, the
protocol, compared with 33% of the patients in the
sequentially rejective Bonferroni method was applied, setting
␣ at 0.05 divided by the number (n) of comparisons (0.05/2 ϭ
There were no significant differences in the rea-
0.025) for the lowest P value obtained in the 2 comparisons,
sons for dropout (Figure 1). The acetaminophen group
and ␣ ϭ 0.05/(n Ϫ 1) (0.05/1 ϭ 0.05) for the second compar-ison if the first yielded a significant result (25,26).
tended to have a higher number of dropouts due to
To achieve meaningful comparisons across groups over
adverse events, but there was a trend in this group
a standardized period, the use of the rescue medication was
toward fewer withdrawals due to other reasons; these
assessed in per-protocol completers over the 6-month treat-
observations are probably of minor clinical significance
ment course. The mean number of days of use was tabulatedfor descriptive purposes, with calculation of the daily average
given the low number of events. Protocol deviations
ibuprofen tablet consumption, while the proportion of patients
consisted mainly of patients not meeting some of the
with any use of the rescue medication was compared between
inclusion/exclusion criteria (mostly presence of concom-
each active treatment group and the placebo group, by chi-
itant diseases, insufficient symptom severity, or violation
of required demographic characteristics); these patientswere therefore withdrawn early from the protocol and
were then assigned a negative efficacy outcome, often
Recruiting started in May 2000, and the last
corresponding to no change from baseline. Other rea-
followup was performed in December 2002. Most of the
sons for withdrawal were evenly distributed throughout
Number of patients withdrawn from the protocol after each
the study. The number of patients, by treatment group,
Figure 2. Mean and SEM changes in the Lequesne index after 1, 3,
who were withdrawn from the protocol at each study
and 6 months of treatment, in the intent-to-treat population (n ϭ 104
in the placebo group, 108 in the acetaminophen group, and 106 in the
The demographic and clinical characteristics of
glucosamine sulfate group). ء ϭ P ϭ 0.032 versus placebo.
the randomized patients were comparable at baseline(Table 2). As expected, the majority of patients were
ϳ11, indicating disease with moderate symptom sever-
female. The mean age was between 60 and 65 years. On
ity. This was confirmed by the baseline WOMAC pain
average, patients were overweight, and 5% of them were
and function subscale scores, which averaged ϳ40 when
obese (BMI Ͼ30 kg/m2). The mean duration of knee OA
normalized to a 0–100 scale (i.e., similar to 40 mm on a
was ϳ7 years, and slightly more than half of the patients
had a Kellgren/Lawrence radiographic grade of 2, al-
Compliance with the study medication regimen
though grading of 2 or 3 was not firmly assigned to
was good in all treatment groups. In trial completers, the
ϳ10% of the patients. Inflammatory joint disease was an
exclusion criterion, but signs of modest inflammation,
The changes in the Lequesne index after 1, 3, and
i.e., mild joint effusion, were present in 12–15% of the
6 months of treatment in the ITT population are re-
patients. The mean Lequesne index score at baseline was
ported in Figure 2. The primary outcome measure was
Demographic and baseline clinical characteristics of patients in the intent-to-treat
* Except where indicated otherwise, values are the mean Ϯ SD. WOMAC ϭ Western Ontario andMcMaster Universities Osteoarthritis Index.
the 6-month change in the index. There was a change ofalmost Ϫ2 with placebo treatment, but the change was
Ϫ3.1 with glucosamine sulfate (P ϭ 0.032 versus pla-cebo) (Table 3). The 2.7-point decrease in the acetamin-ophen group was not significantly different from thedecrease observed with placebo (P ϭ 0.18). For all 3treatments, the degree of improvement in per-protocolcompleters was higher than that in the ITT population;compared with placebo, the difference in the degree ofimprovement was significant in the glucosamine sulfategroup (P ϭ 0.01), but not in the acetaminophen group(P ϭ 0.26).
Similar results were observed for the secondary
outcome measure represented by change in theWOMAC total index (Table 3), for which the differencebetween the glucosamine sulfate group and the placebogroup was statistically significant in both the ITT andper-protocol analyses (P ϭ 0.039 and P ϭ 0.018, respec-tively). Conversely, the improvement observed with acet-aminophen just failed to reach statistical significancewhen compared with placebo (P ϭ 0.08 in both the ITTand per-protocol populations), although it was onlymarginally lower than that achieved with glucosaminesulfate. Both glucosamine sulfate and acetaminophenwere significantly more effective than placebo in termsof improvement in the WOMAC function subscales, but
Figure 3. Effect size of glucosamine sulfate and acetaminophen in the
for the WOMAC pain subscale, the difference from
intent-to-treat and per-protocol completer populations. Diamonds
placebo, for both glucosamine sulfate and acetamino-
show the effect size point estimate; bars show the 95% confidence
phen, failed to reach statistical significance in the ITT
interval. WOMAC ϭ Western Ontario and McMaster Universities
analysis. However, the better trend shown with glu-
cosamine sulfate (P ϭ 0.12 versus placebo in the ITTanalysis) was statistically significant in per-protocol com-pleters (P ϭ 0.014). The small improvements in the low
knee pain as the first threshold to qualify as a responder,
scores on the WOMAC stiffness subscale (Ͻ3 points on
the proportion of responders in the glucosamine sulfate
average at baseline) did not differ significantly among
group was almost 40%, i.e., 18.4% more than with
placebo (P ϭ 0.004) (Table 4). The response rate was
As shown in Figure 3, the effect size of glu-
also higher with acetaminophen than with placebo, with
cosamine sulfate relative to placebo was 0.32, based on
a difference of 12.1% (P ϭ 0.047). When the OARSI-B
the ITT analysis of the Lequesne index results. This
responder criteria were considered, i.e., when the first
effect size was similar to that for the WOMAC total
threshold for response was a high degree of improve-
index (0.31), and only slightly lower than that for the
ment in either knee pain or function, similar results were
WOMAC function subscale (0.34). The effect sizes of
obtained for this additional efficacy outcome (Table 4).
glucosamine sulfate according to the per-protocol ana-
Almost 50% of the patients in the glucosamine
lysis were larger and exceeded 0.40 in all analyses. This
sulfate group reported a decrease in pain above the
included the WOMAC pain subscale, for which the ITT
threshold for MCII, compared with slightly more than
analysis yielded a small effect size of 0.25 with 95%
30% of the patients treated with placebo (P ϭ 0.023).
confidence limits that crossed the zero line. Effect sizes
More than 40% of the patients in the acetaminophen
in the acetaminophen group were smaller and, in most
group achieved the MCII for pain, but the difference
from placebo was not significant (P ϭ 0.11). Conversely,
As assessed using the OARSI-A responder crite-
the difference between acetaminophen and placebo was
ria, which are characterized by high improvement in
significant for the proportion of patients achieving the
Proportion of patients meeting the dichotomous secondary efficacy outcome
measure (responders according to the OARSI-A criteria), or the additional efficacyoutcome measures (OARSI-B responders, achievement of MCII in pain and function, orachievement of PASS in pain and function) at the end of treatment, in the intent-to-treatpopulation*
* P values are versus placebo; all P values less than 0.05 are significant after correction formultiple comparisons according to the sequential Bonferroni method (see Patients andMethods). OARSI ϭ Osteoarthritis Research Society International; MCII ϭ minimalclinically important improvement; PASS ϭ patient acceptable symptom state. See Patientsand Methods for explanation of OARSI-A and OARSI-B responder criteria.
MCII on the WOMAC function scale (P ϭ 0.025),
was a trend toward a lower number of days of use in the
although the proportion of patients in the glucosamine
glucosamine sulfate and acetaminophen groups (both 28
sulfate group who reached this end point was even
days, versus 35 days with placebo). Only 9% of the
higher (P ϭ 0.008 versus placebo). Indeed, PASS was
completers in the placebo group did not use rescue
achieved in well over 60% of the patients receiving
medication at all, compared with 21% in the acetamin-
glucosamine sulfate, with highly significant differences
ophen and 22% in the glucosamine sulfate group (P ϭ
from the placebo group for pain (difference of 21.7%
0.045 and P ϭ 0.027, respectively, versus placebo).
compared with placebo; P ϭ 0.001) and function (dif-
The number of adverse events reported during
ference of 19.0% compared with placebo; P ϭ 0.006).
treatment was similar in all 3 groups: 89 with placebo, 96
The differences between the acetaminophen and pla-
with acetaminophen, and 95 with glucosamine sulfate.
cebo groups in these PASS outcomes did not reach
The most frequent adverse events were of minor clinical
statistical significance (P ϭ 0.22 and P ϭ 0.10, respec-
significance and did not differ in frequency between
groups. Table 5 summarizes the adverse events reported
When a sensitivity analysis was performed on the
by at least 3 patients in any group. There were 5 serious
primary and the 2 principal secondary outcome mea-
adverse events in the placebo group (precordial chest
sures, in which the 7 patients for whom there were no
pain, apnea, pneumonia, elective surgery, and lumbar
efficacy data after randomization were included (assign-
pain), 5 in the acetaminophen group (atrial flutter,
ing to them no changes on all outcomes, according to the
carpal tunnel syndrome, vertebral fracture, meniscus
LOCF approach), the results were virtually identical and
rupture, and crush injury), and 2 in the glucosamine
the differences between glucosamine sulfate and pla-
sulfate group (meniscus rupture and elective surgery).
cebo were significant for all parameters (Lequesne index
Routine laboratory examinations indicated that
P ϭ 0.034, WOMAC total index P ϭ 0.041, and
more patients in the acetaminophen group developed
OARSI-A responder criteria P ϭ 0.004). A significant
abnormalities in liver function (as reflected by levels of
difference between the acetaminophen group and the
transaminases and gamma glutamyl transferase [GGT]);
placebo group was again found only for the OARSI-A
abnormalities were detected in 21 patients in the acet-
aminophen group versus 2 and 6 in the glucosamine
During the 6-month treatment period, the need
sulfate and placebo groups, respectively. These abnor-
for recourse to the rescue medication was low, occurring
malities were the cause of study withdrawal after the
an average of 1 in every 5–6 days, with a mean consump-
3-month assessment in only 2 patients, whose baseline
tion of 0.20–0.26 tablets of 400 mg ibuprofen per day
values were found to be increased almost 2-fold above
across groups. Compared with the placebo group, there
the normal range (alanine aminotransferase in 1 patient
Summary of adverse events occurring in at least 3 patients
any individual patient, either among those who com-
pleted the protocol or among those in whom treatment
was withdrawn. One patient taking placebo had anabnormal serum glucose level (132 mg/dl) at the time of
screening and was withdrawn after 3 months because the
level was still 139 mg/dl. There were no significantchanges in other routine laboratory parameters. DISCUSSION
The results of the GUIDE trial show that crys-
talline glucosamine sulfate, administered once daily at a
dose equivalent to 1,500 mg glucosamine sulfate, is more
effective than placebo in relieving knee OA symptoms.
These data confirm the results obtained in previous
long-term (3-year) clinical studies (4,5) and the general
clinical trial experience with this particular glucosamine
formulation (9). However, compared with these previous
trials, the GUIDE is the first trial with this glucosamine
preparation to be conducted over a 6-month treatment
period, which is currently regarded to be the minimumtrial duration for study of a symptomatic medication in
* Adverse events are grouped by system organ class and reported asMedical Dictionary for Regulatory Activities (MedDRA) lower-level
OA (27). In addition, the study explored a complete
term except for respiratory tract infections and respiratory disorders,
panel of symptom outcomes and included an active
for which similar events were grouped under MedDRA high-level
medication, acetaminophen, as a side comparator.
According to current OA practice guidelines
(2,3), acetaminophen is the oral analgesic that should be
receiving placebo) and almost 3-fold above the normal
tried first and, if successful, the preferred long-term
range (GGT in 1 patient receiving acetaminophen),
symptomatic medication, due to its safety profile and
respectively. Clinically significant abnormalities in GGT,
common use. For this reason, and not for its efficacy,
i.e., levels 2–3 times above the upper reference limit,
acetaminophen was chosen as a side comparator in the
were found in an additional 2 patients receiving acet-
present study. In fact, acetaminophen failed to show a
aminophen and 1 patient in the glucosamine sulfate
statistically significant difference from placebo in the
group, but did not necessitate treatment withdrawal. The
primary efficacy outcome (Lequesne algofunctional in-
remaining abnormalities were mostly transient and mild
dex of severity) and in some of the secondary end points,
(i.e., from slightly above the normal range to less than
including pain outcomes. A marginally significant differ-
twice the maximum normal values) and were recorded as
ence between acetaminophen and placebo was seen in
adverse events in only 2 patients taking acetaminophen.
function outcomes, and the response rate was higher in
In no cases were these alterations judged to necessitate
the acetaminophen group than in the placebo group.
any particular followup that might have interfered with
Conversely, glucosamine sulfate was significantly more
effective than placebo in the primary and virtually all
Serum glucose levels were virtually unaltered in
secondary efficacy outcomes, with a trend toward supe-
acetaminophen- and glucosamine sulfate–treated pa-
riority compared with acetaminophen, although directly
tients who completed the protocol and had both baseline
comparing these 2 active treatments was not an aim of
and 6-month assessments (mean Ϯ SD 99 Ϯ 14 mg/dl at
baseline and 99 Ϯ 13 mg/dl at 6 months in the acetamin-
In most but not all previous trials, acetaminophen
ophen group, and 98 Ϯ 15 mg/dl at both time points in
was globally more effective than placebo but less effec-
the glucosamine sulfate group). A minimal increase was
tive than NSAIDs in the treatment of OA pain, espe-
seen in patients receiving placebo (99 Ϯ 15 at baseline
cially in patients whose pain was moderate to severe;
and 102 Ϯ 16 mg/dl at 6 months). Similarly, there was no
acetaminophen and NSAIDs showed similar efficacy in
clinically significant change in the serum glucose level in
patients with mild OA pain (28). In contrast, acetamin-
ophen exerted no significant effects on the Lequesne or
reach statistical significance in comparison with placebo
WOMAC score (28), consistent with the present find-
in the ITT population, the change was significant in
ings in the GUIDE study. It should be noted that the
per-protocol completers. Furthermore, the threshold for
dosage of acetaminophen used in this study was 3
minimally clinically important improvement in pain (20)
gm/day as is most commonly used in Europe, whereas up
was reached by significantly more ITT patients in the
to 4 gm/day is usually advised in the US (15). The 4 gm
glucosamine sulfate group, and almost 70% of them
daily dosage was used in the majority of previous clinical
reported an acceptable pain state (21) at the end of the
trials, and there are insufficient data to determine
trial, with a significant difference from placebo (Ͼ20%).
whether daily dosages of 3 gm and 4 gm have compara-
A nearly 20% difference from placebo was also found
ble effects; use of this lower dosage might have further
for the proportion of patients who were classified as
compromised the efficacy of acetaminophen in the
treatment responders based on the OARSI composite
present study. On the other hand, safety considerations
with regard to acetaminophen dosage selection also had
The results of GUIDE study are at variance with
to be taken into account, since there were no previous
those of the recently reported GAIT study (13), in which
OA clinical trials in which acetaminophen at 4 gm/day
glucosamine failed to show a significant difference in
had been administered for periods longer than 12 weeks
efficacy compared with placebo over a similar 6-month
(28) at the time the present trial was designed and
treatment period. However, the editorial accompanying
conducted; in addition, the gastrointestinal safety of
the report of the GAIT study (32) states that this finding
acetaminophen at Ͼ2 gm/day has been questioned (29).
was not surprising given the nonconventional glu-
The efficacy results observed with glucosamine
cosamine preparation used in the NIH-sponsored study,
sulfate in the present study were clinically relevant. The
which differed from the glucosamine sulfate formulation
effect size on the primary outcome measure, repre-
used in previous successful trials of glucosamine treat-
sented by the Lequesne index, was 0.32 compared with
ment and in the present study. Indeed, the regimen of
placebo, while the minimal difference that is considered
glucosamine hydrochloride at a dosage of 500 mg 3 times
clinically relevant is achieved with an effect size of 0.20
per day used in the GAIT study (13) is not approved as
(30). Effect sizes between 0.20 and 0.50 are considered
a prescription formulation and was previously used in
“small” (30), but this is a common finding for interven-
only 1 randomized controlled trial, which yielded mostly
tions in OA. An effect size of 0.32 or lower was even
described for NSAIDs for their principal use in knee
The glucosamine sulfate prescription formulation
OA, i.e., short-term pain relief, while the effect size was
used in the GUIDE trial and in most previous glu-
0.29 for the reduction in functional disability (31).
cosamine trials, i.e., once-daily administration of 1,500
Unlike NSAIDs, glucosamine sulfate is not a drug for
mg (4,5), yielded steady-state plasma and synovial fluid
short-term analgesia, but is intended for medium- to
glucosamine concentrations in the 10 M range (34,35).
long-term management of the disease. In this respect,
While these levels may be insufficient to directly stimu-
the small but clinically relevant effect size on symptoms
late the synthesis of cartilage glycosaminoglycans (36),
found in the GUIDE study, being of the magnitude
they have been found to be effective in inhibiting
observed with purely symptomatic medications adminis-
interleukin-1–induced gene expression (37), which has
tered on a short-term basis, further supports the long-
been proposed as the most probable, although hypothet-
ical, mechanism of action of glucosamine sulfate in OA
The Lequesne index is a combined measure of
(38). Conversely, the glucosamine hydrochloride prepa-
pain and functional disability, in which pain parameters
ration used in the GAIT study resulted in plasma
account for one-third of the total score and functional
glucosamine levels that were at least 3-fold lower (39)
parameters for the rest (17). Glucosamine sulfate exhib-
and therefore might have fewer pharmacologic effects.
ited efficacy in all physical function outcome measures in
In addition, while no relationship was found
the GUIDE study, with an effect size of 0.34 on the
between OA development and fasting serum sulfate
relevant WOMAC subscale. Therefore, functional im-
levels (40), sulfates have been suggested to be an
provement might be the main determinant of glu-
important component of glucosamine’s mechanism of
cosamine sulfate’s effectiveness in knee OA. However,
action (41,42). Interestingly, the most significant results
efficacy of glucosamine sulfate was also demonstrated
in the GAIT study were achieved in a subgroup analysis
for several of the pain outcomes. In fact, although the
of patients with more severe symptoms when glu-
improvement on the WOMAC pain subscale failed to
cosamine hydrochloride was combined with chondroitin
sulfate (13), presumably increasing sulfate plasma levels
backgrounds, reflecting differences between the Euro-
(42), and possibly even levels of glucosamine metabo-
pean and North American continents. Finally, the level
lites, to concentrations closer to those achieved with the
of pain at the time of enrollment was apparently lower in
prescription glucosamine sulfate formulation used in the
the GUIDE trial than in the GAIT study (ϳ40 versus
ϳ47, on a 0–100 normalized scale). However, the base-
The response to placebo in the GUIDE study
line Lequesne index scores indicated at least moderate
ranged from 20–25% (for the primary end point and the
symptomatic disease severity in the GUIDE study (17),
responder rate) to 40–45% (for the additional efficacy
and the present results are therefore applicable to this
outcomes). This placebo response rate was therefore in
subset of patients with knee OA. Conversely, previous
the expected range for OA trials and much lower than
long-term trials have focused on the effects of glu-
the rate of Ͼ60% observed in the GAIT trial (13). Such
cosamine sulfate in patients with milder disease (4,5,44).
a high rate of response to placebo is difficult to interpret
Early withdrawal from the study occurred in
and might have partly clouded the results concerning
26–33% of patients. Protocol violations were among the
efficacy of the experimental treatments in the GAIT
most frequent reasons for this, and they were mainly
study. OA trials are often add-on studies of test treat-
represented by patients not meeting the inclusion/
ments with a rescue analgesic medication, whose indis-
exclusion criteria suggested by current guidelines
criminate use might increase the placebo response. The
(14,15), who were thus misrandomized. The proportion
use of the rescue medication was strictly regulated in the
of such patients was comparable in all 3 treatment
present study, and this might account for its low con-
groups, and they were conservatively and appropriately
sumption and the observed low rate of response to
accounted for in the statistical analysis. Their early
withdrawal immediately after randomization necessi-
A possible limitation of the present study may be
tated assigning them a negative efficacy outcome for all
the requirement of a 6-month washout from prior glu-
assessments, according to the LOCF approach.
cosamine sulfate use, since patients who had potentially
Adverse events were the other main reason for
had a poor response to previous glucosamine treatment
dropout, although treatment safety was good throughout
would not be as willing to participate as those who had
the study. Glucosamine sulfate was well tolerated, and
not previously been treated with this agent. However,
did not differ from placebo in terms of frequency of
appropriate washout from previous treatment is manda-
adverse events or abnormal findings of laboratory eval-
tory in clinical trials of compounds such as glucosamine
uations, including glucose serum levels. These observa-
sulfate, which are thought to have a persistent effect
tions confirm the good safety profile of this agent, as
observed in all previous meta-analyses (3,9,45,46) and
Among other possible limitations of the present
study, it should be noted that although Ͼ90% of the
To our knowledge, the GUIDE is the first OA
patients were overweight (BMI 25–30 kg/m2), only 5%
trial to assess the safety of acetaminophen in compari-
were actually obese (BMI Ͼ30 kg/m2), due to the
son with placebo over a treatment period of 6 months.
protocol restrictions, and the average BMI was slightly
Previous trials using naproxen as a comparator docu-
lower than 28 kg/m2. In most knee OA trials the average
mented the good safety profile of acetaminophen at
BMI is higher than this, and it was even Ͼ30 kg/m2 in
doses of 2,600 mg/day for 2 years (47) and 4 gm/day for
some North American trials, including, e.g., the GAIT
6–12 months (48); acetaminophen was also well toler-
study (13). This is due to the high prevalence of obesity
ated in the present study, with no findings that would
among patients with symptomatic knee OA in the US.
cause concern with regard to gastrointestinal safety (29).
The results of the GUIDE trial therefore might not be
However, abnormalities in liver function were found in
generalizable to obese patients, and the effectiveness of
ϳ20% of the acetaminophen-treated patients, even
glucosamine sulfate in such patients would require fur-
though the drug was used at a relatively low dosage of 3
ther assessment. We also enrolled a slightly higher
gm/day, further supporting this dosage selection. The
proportion of female patients, i.e., almost 90% com-
alterations in liver function were mostly mild and tran-
pared with almost 80% in previous glucosamine sulfate
sient, and in only 5 patients were they either deemed
trials (4,5), but the results seem to have been in the same
clinically significant, reported as adverse events, or the
reason for treatment withdrawal (compared with 1 each
Additional differences in the study populations of
in the placebo and glucosamine sulfate groups).
the GUIDE and GAIT trials include genetic and ethnic
In conclusion, the results of the GUIDE trial
demonstrate that glucosamine sulfate at the once-daily
2. American College of Rheumatology Subcommittee on Osteoar-
dosage of 1,500 mg is an effective medication for knee
thritis Guidelines. Recommendations for the medical managementof osteoarthritis of the hip and knee: 2000 update. Arthritis
OA symptoms, compared with placebo. These data were
obtained during a 6-month period, which is the currently
3. Jordan KM, Arden NK, Doherty M, Bannwarth B, Bijlsma JW,
recommended minimum treatment duration for the
Dieppe P, et al. EULAR recommendations 2003: an evidencebased approach to the management of knee osteoarthritis: report
management of OA, and they complement those ob-
of a task force of the Standing Committee for International
tained over long-term treatment periods of 3 years (4,5).
Clinical Studies Including Therapeutic Trials (ESCISIT). Ann
To date, no studies have demonstrated any other phar-
4. Reginster JY, Deroisy R, Rovati LC, Lee RL, Lejeune E, Bruyere
macologic treatment to have the same efficacy as glu-
O, et al. Long-term effects of glucosamine sulfate on osteoarthritis
cosamine sulfate for the long-term treatment of OA
progression: a randomised, placebo-controlled clinical trial. Lan-
symptoms (49). The efficacy results obtained with glu-
5. Pavelka K, Gatterova J, Olejarova M, Machacek S, Giacovelli G,
cosamine sulfate were significant and clinically relevant
Rovati LC. Glucosamine sulfate use and delay of progression of
in the present study in which acetaminophen, the cur-
knee osteoarthritis: a 3-year, randomized, placebo-controlled,
rently recommended preferred medication (2,3), was
double-blind study. Arch Intern Med 2002;162:2113–23.
6. Russell AS, Aghazadeh-Habashi A, Jamali F. Active ingredient
used as a side comparator. A trial specifically designed
consistency of commercially available glucosamine sulfate prod-
to directly compare it with acetaminophen and possibly
an NSAID would be needed in order to assess whether
7. McAlindon T, Formica M, LaValley M, Lehmer M, Kabbara K.
Effectiveness of glucosamine for symptoms of knee osteoarthritis:
glucosamine sulfate could be regarded as the preferred
results from an internet-based randomized double-blind con-
trolled trial. Am J Med 2004;117:643–9.
8. Cibere J, Kopec JA, Thorne A, Singer J, Canvin J, Robinson DB,
et al. Randomized, double-blind, placebo-controlled glucosamine
AUTHOR CONTRIBUTIONS
discontinuation trial in knee osteoarthritis. Arthritis Care Res2004;51:738–45.
Dr. Herrero-Beaumont had full access to all of the data in the
9. Towheed TE, Maxwell L, Anastassiades TP, Shea B, Houpt J,
study and takes responsibility for the integrity of the data and the
Robinson V, et al. Glucosamine therapy for treating osteoarthritis.
Cochrane Database Syst Rev [serial online]. 2005;(2):CD002946. Study design. Dr. Herrero-Beaumont.
URL: http://www.thecochranelibrary.com. Acquisition of data. Drs. Herrero-Beaumont, Ivorra, Trabado, Blanco,
10. McAlindon T. Why are clinical trials of glucosamine no longer
Benito, Martı´n-Mola, Paulino, Marenco, Porto, Laffon, Arau
uniformly positive? Rheum Dis Clin N Am 2003;29:789–801.
11. Clegg DO, Reda DJ, Harris CL, Klein MA, for the GAIT
Analysis and interpretation of data. Drs. Herrero-Beaumont, Ivorra,
Investigators. The efficacy of glucosamine and chondroitin sulfate
Trabado, Blanco, Benito, Martı´n-Mola, Paulino, Marenco, Porto,
in patients with painful knee osteoarthritis (OA): the Glu-
cosamine/chondroitin Arthritis Intervention Trial [abstract]. Ar-
Manuscript preparation. Drs. Herrero-Beaumont, Ivorra, Trabado,
Blanco, Benito, Martı´n-Mola, Paulino, Marenco, Porto, Laffon,
12. Herrero-Beaumont G, Roman JA, Trabado MC, Blanco FJ,
Benito P, Martin-Mola E, et al. Effects of glucosamine sulfate on
Statistical analysis. Dr. Giampaolo Giacovelli (nonauthor; Rotta-
6-month control of knee osteoarthritis symptoms versus placebo
and acetaminophen: results from the Glucosamine Unum In DieEfficacy (GUIDE) trial [abstract]. Arthritis Rheum 2005;52 Suppl9:S460. ROLE OF THE STUDY SPONSOR
13. Clegg DO, Reda DJ, Harris CL, Klein MA, O’Dell JR, Hooper
GUIDE is a regulatory trial agreed upon by the sponsor
MM, et al. Glucosamine, chondroitin sulfate and the two in
(Rottapharm) and the relevant health authorities and designed with
combination for painful knee osteoarthritis. N Engl J Med 2006;
the principal investigator (Dr. Herrero-Beaumont). Following proto-
col approval and implementation, the statistical analysis plan was
14. Altman R, Asch E, Bloch D, Bole G, Borenstein D, Brandt K, et
prepared and executed by the sponsor. The statistical analysis was
al. Development of criteria for the classification and reporting of
supervised by the principal investigator, and each author had the
osteoarthritis: classification of osteoarthritis of the knee. Arthritis
opportunity to review the data and the analysis. The sponsor provided
the study medication and funding for the trial. In addition, it moni-
15. Altman R, Brandt K, Hochberg M, Moskowitz R. Design and
tored the study according to Good Clinical Practice standards and
conduct of clinical trials of patients with osteoarthritis: recommen-
according to all applicable laws and guidelines, to preserve the
dations from a task force of the Osteoarthritis Research Society.
integrity of the data and their collection. However, Rottapharm as a
Osteoarthritis Cartilage 1996;4:217–43.
corporate entity had no control over the writing, contents, or decision
16. Kellgren JH, Lawrence JS. Radiological assessment of osteoar-
to submit the present manuscript for publication.
throsis. Ann Rheum Dis 1957;16:494–501.
17. Lequesne MG, Mery C, Samson M, Gerard P. Indexes of severity
for osteoarthritis of the hip and knee: validation-value in compar-
REFERENCES
ison with other assessment tests. Scand J Rheumatol Suppl1987;65:85–9.
1. Felson DT, Lawrence RC, Hochberg MC, McAlindon T, Dieppe
18. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW.
PA, Minor MA, et al. Osteoarthritis: new insights. Part 2. Treat-
Validation of WOMAC: a health status instrument for measuring
ment approaches. Ann Intern Med 2000;133:726–37.
clinically important patient relevant outcomes to antirheumatic
drug therapy in patients with osteoarthritis of the hip or knee.
cosamine sulfate in knee osteoarthritis patients [abstract]. Arthri-
19. Dougados M, LeClaire P, van der Heijde D, Bloch DA, Bellamy
36. Biggee BA, Blinn CM, McAlindon TE, Nuite M, Silbert JE. Low
N, Altman RD. A report of the Osteoarthritis Research Society
levels of human serum glucosamine after ingestion of glucosamine
International standing committee for clinical trials response crite-
sulfate relative to capability for peripheral effectiveness. Ann
ria initiative. Osteoarthritis Cartilage 2000;8:395–403.
20. Tubach F, Ravaud P, Baron G, Falissard B, Logeart I, Bellamy N,
37. Piepoli T, Zanelli T, Letari O, Persiani S, Rovati LC, Caselli G.
et al. Evaluation of clinically relevant changes in patient reported
Glucosamine sulfate inhibits IL-1-stimulated gene expression at
outcomes in knee and hip osteoarthritis: the minimal clinically
concentrations found in humans after oral intake [abstract]. Ar-
important improvement. Ann Rheum Dis 2005;64:29–33 [origi-
nally published online 18 June 2004].
38. Largo R, Alvarez-Soria MA, Diez-Ortego I, Calvo E, Sanchez-
21. Tubach F, Ravaud P, Baron G, Falissard B, Logeart I, Bellamy N,
Pernaute O, Egido J, et al. Glucosamine inhibits IL-1-induced
et al. Evaluation of clinically relevant states in patient reported
NFB activation in human osteoarthritic chondrocytes. Osteoar-
outcomes in knee and hip osteoarthritis: the patient acceptable
symptom state. Ann Rheum Dis 2005;64:34–7 [originally pub-
39. Jackson CG, Plaas AH, Barnhill JG, Harris CL, Clegg DO. The
pharmacokinetics of oral glucosamine and chondroitin sulfate in
22. Noack W, Fischer M, Forster KK, Rovati LC, Setnikar I. Glu-
humans [abstract]. Arthritis Rheum 2005;52:4062–3.
cosamine sulfate in osteoarthritis of the knee. Osteoarthritis
40. Blinn CM, Dibbs ER, Hronowski LJ, Vokonas PS, Silbert JE.
Fasting serum sulfate levels before and after development of
23. Pocock SJ. Clinical trials: a practical approach. Chichester (UK):
osteoarthritis in participants of the Veterans Administration Nor-
John Wiley & Sons; 1983. p. 123–41.
mative Aging Longitudinal Study do not differ from levels in
24. Hedges LV, Olkin I. Statistical methods for meta-analysis. Or-
participants in whom osteoarthritis did not develop. Arthritis
25. Proschan MA, Waclawiw MA. Practical guidelines for multiplicity
41. Hoffer LJ, Kaplan LN, Hamadeh MJ, Grigoriu AC, Baron M.
adjustment in clinical trials. Control Clin Trials 2000;21:527–39.
Sulfate could mediate the therapeutic effect of glucosamine sul-
26. Hochberg Y, Benjamini Y. More powerful procedures for multiple
significance testing. Stat Med 1990;9:811–8.
42. Cordoba F, Nimni ME. Chondroitin sulfate and other sulfate
27. Committee for Proprietary Medicinal Products. Points to consider
containing chondroprotective agents may exhibit their effects by
on clinical investigation of medicinal products used in the treat-
overcoming a deficiency of sulfur amino acids. Osteoarthritis
ment of osteoarthritis (CPMP/EWP/784/97). London: European
Agency for the Evaluation of Medicinal Products; 1998.
43. Lequesne M, Brandt K, Bellamy N, Moskowitz R, Menkes CJ,
28. Towheed TE, Maxwell L, Judd MG, Catton M, Hochberg MC,
Pelletier JP, et al. Guidelines for testing slow acting drugs in
Wells G. Acetaminophen for osteoarthritis. Cochrane Database
osteoarthritis. J Rheumatol Suppl 1994;41:65–71.
Syst Rev 2006;(1):CD004257. URL: http://www.thecochranelibrary.
44. Bruyere O, Reginster JY, Giacovelli G, Barbetta B, Rovati LC,
Pavelka K. Clinical significance of the long-term symptom-
29. Garcia Rodriguez LA, Hernandez-Diaz S. The risk of upper
modifying effects of glucosamine sulfate: comment on the
gastrointestinal complications associated with nonsteroidal anti-
article by Brandt and Mazzuca [letter]. Arthritis Rheum 2006;
inflammatory drugs, glucocorticoids, acetaminophen and combi-
nation of these agents. Arthritis Res 2001;3:98–101.
45. McAlindon TE, LaValley MP, Gulin JP, Felson DT. Glu-
30. Kazis LE, Anderson JJ, Meenan RF. Effect sizes for interpreting
cosamine and chondroitin for treatment of osteoarthritis: a
changes in health status. Med Care 1989;27 Suppl 3:S178–89.
systematic quality assessment and meta-analysis. JAMA 2000;
31. Bjordal JM, Ljunggren AE, Klovning A, Slordal L. Non-steroidal
anti-inflammatory drugs, including cyclo-oxygenase-2 inhibitors, in
46. Richy F, Bruyere O, Ethgen O, Cucherat M, Henrotin Y, Regin-
osteoarthritis knee pain: meta-analysis of randomised placebo
ster JY. Structural and symptomatic efficacy of glucosamine and
controlled trials. BMJ 2004;329:1317–22.
chondroitin in knee osteoarthritis: a comprehensive meta-analysis.
32. Hochberg MC. Nutritional supplements for knee osteoarthritis—
still no resolution [editorial]. N Engl J Med 2006;354:858–60.
47. Williams HJ, Ward JR, Egger MJ, Neuner R, Brooks RH, Clegg
33. Houpt JB, McMillan R, Wein C, Paget-Dellio SD. Effect of
DO, et al. Comparison of naproxen and acetaminophen in a
glucosamine hydrochloride in the treatment of pain of osteoarthri-
two-year study of treatment of osteoarthritis of the knee. Arthritis
tis of the knee. J Rheumatol 1999;26:2423–30.
34. Persiani S, Roda E, Rovati LC, Locatelli M, Giacovelli G, Roda A.
48. Temple RA, Benson GD, Zinsenheim JR, Schweinle JE. Multi-
Glucosamine oral bioavailability and plasma pharmacokinetics
center, randomized, double-blind, active-controlled, parallel-
after increasing doses of crystalline glucosamine sulfate in man.
group trial of the long-term (6-12 months) safety of acetamino-
Ostoeoarthritis Cartilage 2005;13:1041–9.
phen in adult patients with osteoarthritis. Clin Ther 2006;28:
35. Persiani S, Rotini R, Trisolino G, Delliponti L, Rovati LC,
Locatelli M, et al. Glucosamine plasma and synovial fluid concen-
49. McAlindon T. Glucosamine for osteoarthritis: dawn of a new era?
trations before and after oral administration of crystalline glu-
Internet Journal of e-Language Learning & Teaching, 4(1), January 2007, pp. 15-31 The Use of ICT in the Implementation of Student- Centered Learning (SCL) HAFIZOAH KASSIM & ZURAINA ALI Universiti Malaysia Pahang Abstract As one of the new teaching approaches, Student-Centered Learning (SCL) has been proven to be effective in its ability to teach students. At
Development of Ultrasonic Assisted Extraction Method of Emerging Contaminants in Freshwater Sediments Diana Nara Ribeiro de Sousa1, Guilherme Martins Grosseli1, Mariele Barboni Campanha1, Renato Lajarim Carneiro1, Antonio Aparecido Mozeto1, Pedro Sérgio Fadini1 1Universidade Federal de São Carlos – UFSCar, Rod. Washington Luís km 235, São Introduction: The determination
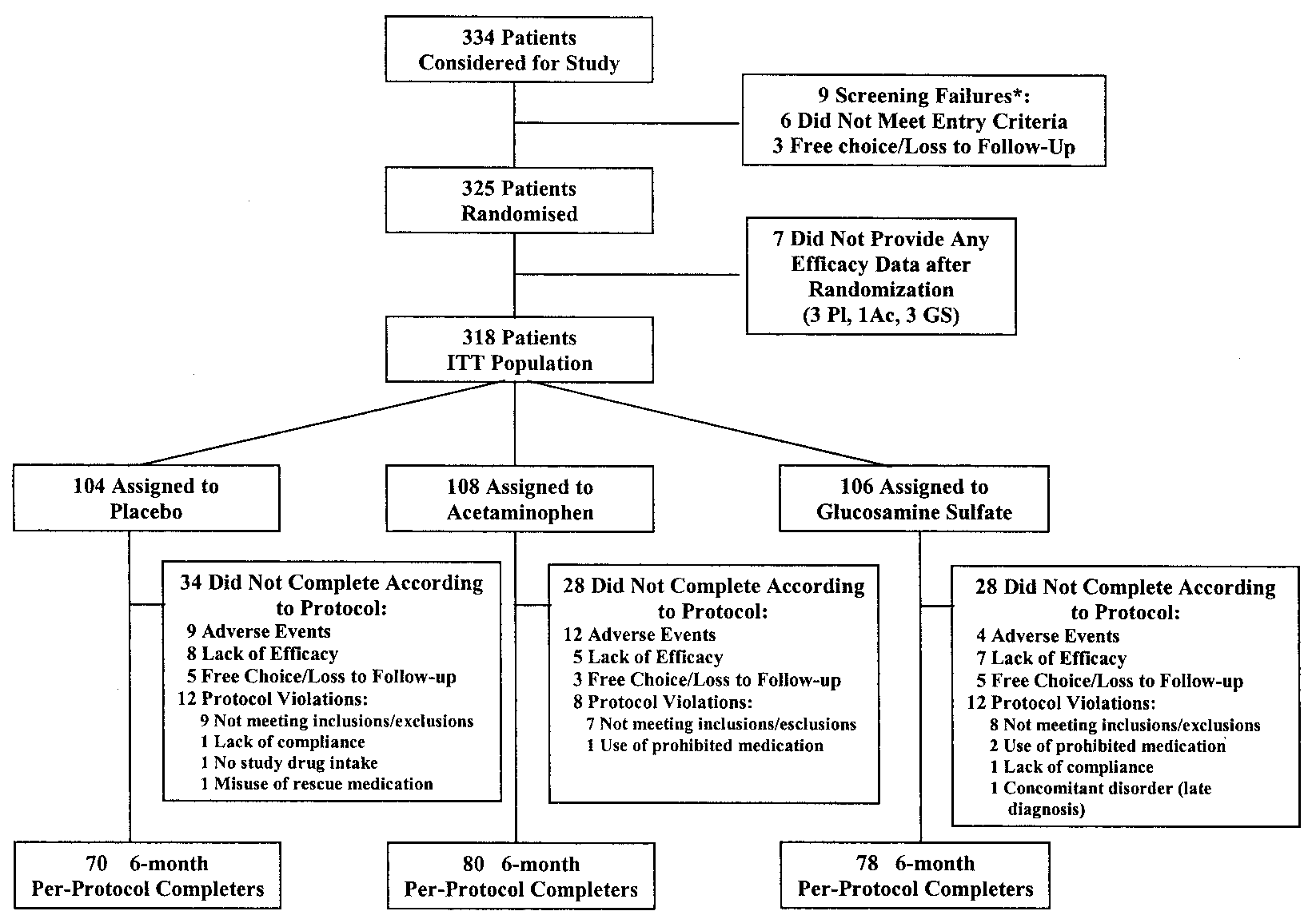 Figure 1. Study profile. ء ϭ patients who agreed to baseline evaluation but did not qualify for randomization. Pl ϭ
Figure 1. Study profile. ء ϭ patients who agreed to baseline evaluation but did not qualify for randomization. Pl ϭ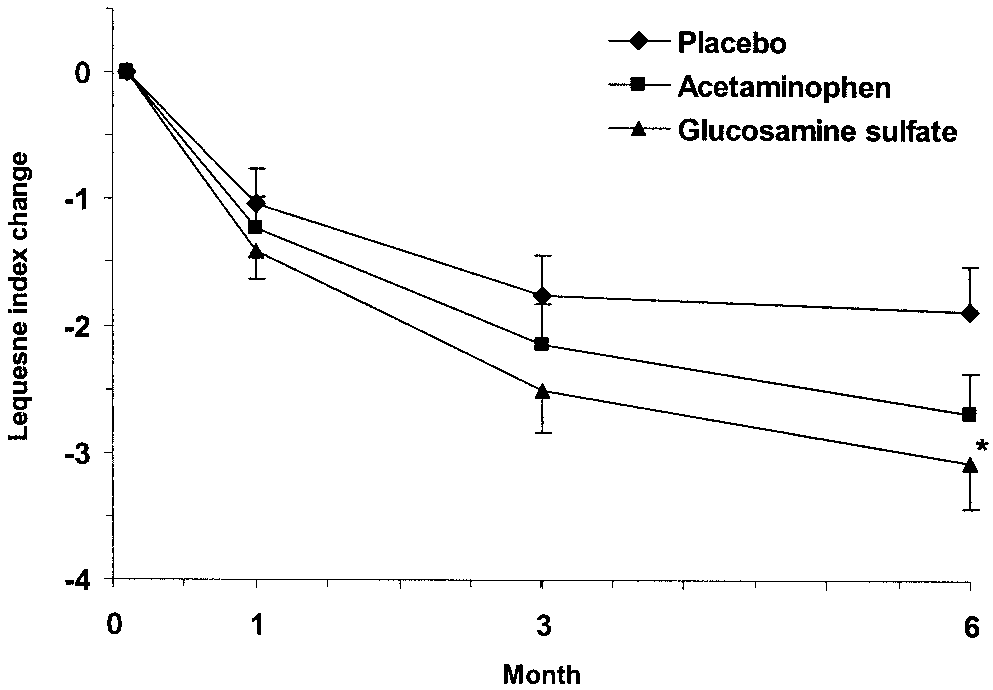 Number of patients withdrawn from the protocol after each
the study. The number of patients, by treatment group,
Figure 2. Mean and SEM changes in the Lequesne index after 1, 3,
Number of patients withdrawn from the protocol after each
the study. The number of patients, by treatment group,
Figure 2. Mean and SEM changes in the Lequesne index after 1, 3,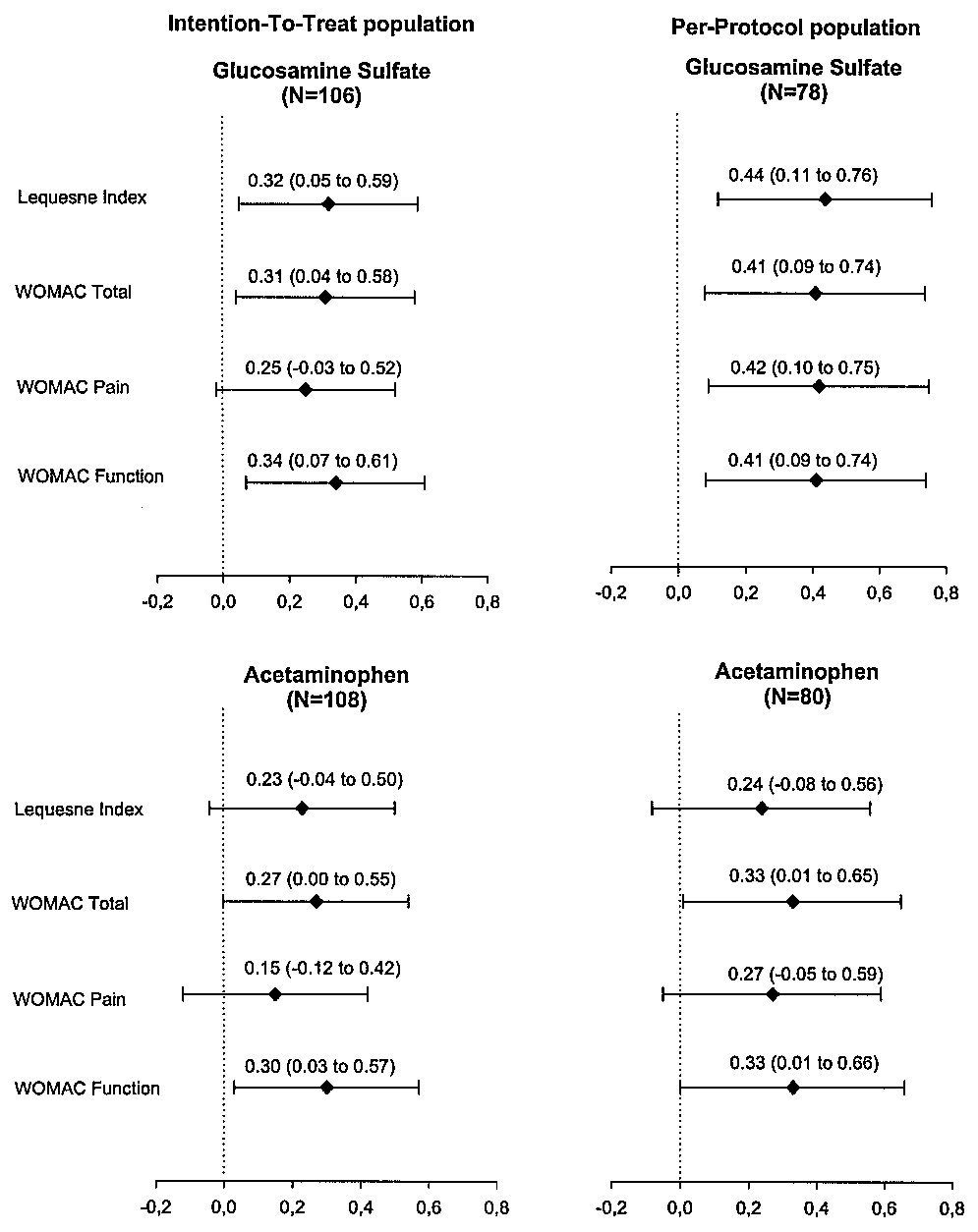 the 6-month change in the index. There was a change ofalmost Ϫ2 with placebo treatment, but the change was
Ϫ3.1 with glucosamine sulfate (P ϭ 0.032 versus pla-cebo) (Table 3). The 2.7-point decrease in the acetamin-ophen group was not significantly different from thedecrease observed with placebo (P ϭ 0.18). For all 3treatments, the degree of improvement in per-protocolcompleters was higher than that in the ITT population;compared with placebo, the difference in the degree ofimprovement was significant in the glucosamine sulfategroup (P ϭ 0.01), but not in the acetaminophen group(P ϭ 0.26).
the 6-month change in the index. There was a change ofalmost Ϫ2 with placebo treatment, but the change was
Ϫ3.1 with glucosamine sulfate (P ϭ 0.032 versus pla-cebo) (Table 3). The 2.7-point decrease in the acetamin-ophen group was not significantly different from thedecrease observed with placebo (P ϭ 0.18). For all 3treatments, the degree of improvement in per-protocolcompleters was higher than that in the ITT population;compared with placebo, the difference in the degree ofimprovement was significant in the glucosamine sulfategroup (P ϭ 0.01), but not in the acetaminophen group(P ϭ 0.26).