Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Doi:10.1016/j.jpeds.2007.04.010
Nebulized Hypertonic Saline in the Treatment of Viral Bronchiolitis in Infants
BRIAN A. KUZIK, MD, MSC, FRCP(C), SAMIM A. AL QADHI, MD, MBCHB, STEVEN KENT, BSC(MED), MD, FRCP(C),
MICHAEL P. FLAVIN, MB, MRCP(UK), FRCP(C), WILMA HOPMAN, MA, SIMON HOTTE, MD, AND SARAH GANDER, MD
Objective To investigate the use of nebulized 3% hypertonic saline (HS) for treating viral bronchiolitis in moderately ill hospitalized infants by a prospective, randomized, double-blinded, controlled, multicenter trial. Study design A total of 96 infants (mean age, 4.7 months; range, 0.3 to 18 months) admitted to the hospital for treatment of viral bronchiolitis were recruited from 3 regional pediatric centers over 3 bronchiolitis seasons (December 2003 to May 2006). Patients were randomized to receive, in a double-blind fashion, repeated doses of nebulized 3% HS (treatment group) or 0.9% normal saline (NS; control group), in addition to routine therapy ordered by the attending physician. The principal outcome measure was hospital length of stay (LOS). On an intention-to-treat basis, the infants in the HS group had a clinically relevant 26% reduction in LOS to 2.6 ؎ 1.9 days, compared with 3.5 ؎ 2.9 days in the NS group (P ؍ .05). The treatment was well tolerated, with no adverse effects attributable to the use of HS. Conclusions The use of nebulized 3% HS is a safe, inexpensive, and effective treatment for infants hospitalized with moderately severe viral bronchiolitis. (J Pediatr 2007;151:266-70) Respiratorysyncytialvirus(RSV)accountsforthemajorityofviralbronchiolitiscases,althoughotherviruses,including
human metapneumovirus, adenovirus, parainfluenza, rhinovirus, and influenza,also play important Given that virtually all children become infected with
RSV by age 2 years and that at least 1% of these children will develop bronchiolitis
sufficient to require the burden of this disease is high, accounting for upto 17% of all infant at an annual cost of more than $500 million in theUnited States
From the Department of Paediatrics,Sheikh Khalifa Medical City, Abu Dhabi,
Despite the high prevalence and morbidity of bronchiolitis, therapy remains con-
United Arab Emirates (B.K., S.Q.); Depart-
troversial and without widely accepted therapeutic guidelines other than supportive
ment of Paediatrics, University of BritishColumbia, Victoria General Hospital, Victo-
Bronchiolitis is characterized by airway plugging with sloughed epithelium,
ria, British Columbia, Canada (S.K.); Depart-
mucus, and edema rather than Nevertheless, the use of nebulized
ment of Paediatrics, Queen’s University,
bronchodilators continues to be despite extensive evidence supported by 3
Kingston General Hospital, Kingston, On-tario, Canada (M.F., S.H., S.G.); Clinical Re-
meta-analyses that the benefits are limited, short term, and do not justify routine
Similarly, although steroids might reasonably be expected to decrease the inflammatory
response in bronchiolitis, published data are conflicting, with equally well-designed
Supported by the Queen Alexandra Foun-dation for Children, British Columbia, Can-
studies concluding that steroids may be either or The
primary treatment, therefore, remains largely supportive, with administration of fluids and
Youth and Maternal Programme, BritishColumbia, Canada; and an Ontario Tho-
supplemental oxygen, observation, and mechanical ventilatory support as
Several reports over the last decade have demonstrated that inhalation of nebulized
No reprint requests are available from the
6% to 10% hypertonic saline (HS) improves both immediate and long-term clearance of
small airways in patients with cystic The exact mechanism is unknown but
Submitted for publication Aug 17, 2006;last revision received Mar 7, 2007; accepted
is thought to facilitate removal of inspissated mucus through osmotic hydration, disrup-
tion of mucus strand cross-linking, and reduction of mucosal In otherwise
Reprint requests: Brian A. Kuzik, MD, MSc,FRCP(C), Department of Paediatrics, RoyalVictoria Hospital of Barrie, 208-1 QuarryRidge Road, Barrie, Ontario, Canada L4M
Respiratory Distress Assessment Instrument
6M2. E-mail: briankuzik@hotmail.com.
healthy infants hospitalized with viral bronchiolitis, the reg-
Study Design
ular administration of nebulized 3% HS combined with epi-
Patients admitted to hospital with bronchiolitis were
nephrine decreased length of stay (LOS) by approximately
assessed within 12 hours for entry into the study. If inclusion/
22% compared with infants receiving the same dose of epi-
exclusion criteria were satisfied, then informed consent was
nephrine mixed in 0.9% normal saline Similarly, in
obtained, and the patient was randomized to receive treat-
ambulatory infants with mild bronchiolitis, inhalation of neb-
ment with 4 mL of nebulized study solution containing either
ulized 3% HS (with terbutaline) improved clinical scores but
3% HS (study group) or NS (control group). The study
did not produce a decrease in hospital admission rate.Both
solution was administered in a double-blind fashion every 2
of the aforementioned studies used 3 times per day dosing,
hours for 3 doses, followed by every 4 hours for 5 doses,
which is significantly less than the 3 to 6 times per hour
followed by every 6 hours until discharge. After study enroll-
regimens often used to deliver nebulized medication to chil-
ment, any additional (nonprotocol) treatments were at the
sole discretion of the attending physician, who was blinded to
The purpose of the present study was to investigate the
the study treatment. If additional treatments included nebu-
addition of frequently nebulized 3% HS to standard therapy
lized medication, the medication was nebulized in 4 mL of
of moderately ill infants hospitalized with typical viral bron-
the assigned study solution (ie, HS or NS). All inhaled
chiolitis in a prospective, randomized, double-blind, con-
therapies were delivered to a settled infant from a standard
trolled fashion. The primary objective was to compare the
oxygen-driven hospital nebulizer through a tight-fitting face-mask, or head box, whichever was better tolerated by the
LOS of these infants with that of a control group of infants
receiving standard therapy plus frequently nebulized NS.
Patients were randomized independently at each study
site to receive either HS or NS using a computer-based
randomization program. Study solutions were prepared by aresearch pharmacist and were identical in appearance and
Patients
odor. The identity of the study solutions was blinded to all
Infants up to age 18 months who were admitted to the
participants, care providers, and investigators. Clinical re-
hospital for the treatment of moderately severe viral bronchi-
sponse was determined by the designated study physicianusing RDAI scores and SaO
olitis were eligible for study. The diagnosis of moderately
severe bronchiolitis required a history of a preceding viralupper respiratory infection, the presence of wheezing orcrackles on chest auscultation, plus either an oxygen satura-
Determination of LOS
LOS was defined as the time between study entry
2) of Ͻ94% in room air or significant respiratory
distress as measured by a Respiratory Distress Assessment
(within 12 hours of admission to the hospital) and the time at
Instrument score of Ն4. In brief, 6 separate assess-
which the infant either reached protocol-defined discharge
ments of retractions and auscultatory findings are made and
criteria as measured by the study physician or was discharged
assigned a numerical score; the sum of these scores provides
from the hospital on independent clinical grounds by the
the RDAI score ranging from 0 to 17, with increasing scores
attending physician, whichever came first. Protocol-defined
indicating increasing respiratory distress.
discharge criteria required both an RDAI score Ͻ4 and an
Exclusion criteria included a history of any of the fol-
SaO2 of at least 95% in room air for 4 hours.
lowing: previous episode of wheezing, chronic cardiopulmo-nary disease or immunodeficiency; critical illness at presenta-
tion requiring admission to intensive care; the use of
The study was approved by the ethics and human
nebulized HS within the previous 12 hours; or premature
research committees of the 3 participating hospitals. In-
birth (gestational age Յ 34 weeks).
formed written consent was obtained from at least 1 parent ofeach infant before enrollment. Statistical Strategy
The study was conducted at 3 regional tertiary care
A reduction in LOS of 1 day was previously proposed as
hospitals: Sheikh Khalifa Medical City (SKMC), Abu Dhabi,
being clinically and was adopted in this study. It
United Arab Emirates; Victoria General Hospital (VGH),
was anticipated that this would require a sample size of
Victoria, British Columbia, Canada, and Kingston General
approximately 46 patients per trial arm, for 80% power, to
Hospital (KGH), Kingston, Ontario, Canada. VGH and
show a P value Յ .05. This number is based on a prestudy
KGH serve multiethnic populations in the west coast and
mean LOS at the largest study hospital (SKMC) of 4.1 Ϯ 1.7
central regions of Canada, respectively. Data were collected
days (unpublished data). Data were entered into an Excel
during the winter bronchiolitis seasons between December
spreadsheet (Microsoft Corp, Redmond, WA) and imported
into SPSS version 12.0.1 software (SPSS Inc, Chicago, IL)
Nebulized Hypertonic Saline in the Treatment of Viral Bronchiolitis in Infants
Table I. Patient demographics and illness status at Table III. Treatments received during the study baseline Treatment (n ؍ 47)* (n ؍ 49)* P (n ؍ 47)* (n ؍ 49)* P
*Sample sizes vary slightly for the individual comparisons due to missing data.
tested infants were positive for RSV. Subset comparison of
the SKMC and Canadian sites revealed minimal differences
*Sample sizes vary slightly for the individual comparisons due to missing data.
the Arab infants tended to be sicker (RDAI 8.9 Ϯ 2.9 vs6.2 Ϯ 1.9; P Ͻ .001) and more likely to receive previoustreatment with a bronchodilator (98% vs 70%; P Ͻ .001), all
for analysis on an intention-to-treat basis. Descriptive analy-
ses were completed overall and also for the control and studygroups separately. The 2 test (Fisher’s exact) was used to
Treatment Received
examine the association between categorical variables and
After enrollment, all treatments (protocol and add-on)
group, and independent sample t tests and Levene’s test for
received by infants in the HS and NS groups were comparable
equality of variance were used to assess the association be-
The infants received a mean of 9 nebulizations of
tween numeric variables and group. One-way analysis of
study solution per day delivered alone (38% of treatments) or
variance (ANOVA) was used to compare data from the 3
co-administered with albuterol (salbutamol; 37%), racemic
study sites. To test for the potential effect of age on the
epinephrine (racepinephrine; 23%), or inhaled steroid (3%).
results, the patients were divided into 3 age groups (0 to 6
Subset comparison of the SKMC and Canadian sites revealed
months, 7 to 12 months, and 13 to 18 months), and the
minimal differences in the treatments received
effects of age and treatment were tested in a 2-way ANOVA.
available at Treatment at SKMC was morelikely to include antibiotics (P ϭ .002) as well as the addition
of racemic epinephrine to the inhaled study solution (P ϭ
Study Population
A total of 96 previously well infants (mean age, 4.7 Ϯ
4.2 months; range, 10 days to 18 months) with viral bron-
Adverse Effects of HS
chiolitis were enrolled from 3 centers during the bronchiolitis
All participants tolerated therapy without apparent ad-
seasons from December 2003 to May 2006. Thirty-two in-
verse effects and were eventually discharged after achieving
fants were enrolled from the 2 Canadian sites (VGH and
full recovery. No infants were withdrawn by the medical staff
KGH), and 64 infants were enrolled from SKMC. Forty-
due to clinical deterioration or the need for intensive care
seven infants were randomized to the HS treatment group,
support. Although 5 infants were withdrawn at parents’ re-
and 49 were randomized to the NS control group. Five infants
quest because of perceived adverse effects of therapy, only 2 of
(2 from the HS group and 3 from the NS group) were
these infants were receiving HS. One of these infants (a
withdrawn at parental request before study completion but
2-month-old male) cried very vigorously during his third
were included in the final intention-to-treat analysis.
inhalation (HS alone) and again with his fifth inhalation (HS
The HS and NS groups were comparable at baseline
with racemic epinephrine) and was withdrawn at that time.
and typically presented on the fifth day of illness (range, 1 to
This was not associated with any significant acute change in
14 days) with borderline hypoxia (mean SaO2, 95%; range,
his clinical condition, and he was eventually discharged on
85% to 100%) and moderate respiratory distress (mean clinical
day 6. The second infant (a 3-month-old female) was with-
score, 8 out of 17; range, 4 to 17) Some 69% of all
drawn because of agitation after her second inhalation (HS
The Journal of Pediatrics • September 2007
bronchiolitis studies, with a slight male predominance (62%),primary infection with RSV (69%), mean age of 4.7 months,and LOS in the control group of 3.5 to 4 Strictinclusion and discharge criteria were used to minimize pos-sible confounding effects of uncharacterized and evolvingwheezing phenotypes and to minimize between-site variabil-ity. The clinical scoring system chosen has been widely usedin other studies on and has been proposedto be the scoring system of choice for further studies.Therefore, our findings should be universally applicable toother previously healthy infants hospitalized with moderatelysevere viral bronchiolitis.
The majority of our patients received bronchodilators
before study entry. In addition, although our study protocoldid not require or encourage the co-administration of bron-chodilator with the study solution, blinded attending physi-cians prescribed bronchodilators approximately 5 times perday. This finding was not unexpected, because the use ofbronchodilators in bronchiolitis remains widespread, withsome reporting it in more than 80% of It is alsopossible that attending physicians prescribed bronchodilatorsto prevent possible adverse effects of HS. Although inhalationof HS may cause bronchoconstriction in and
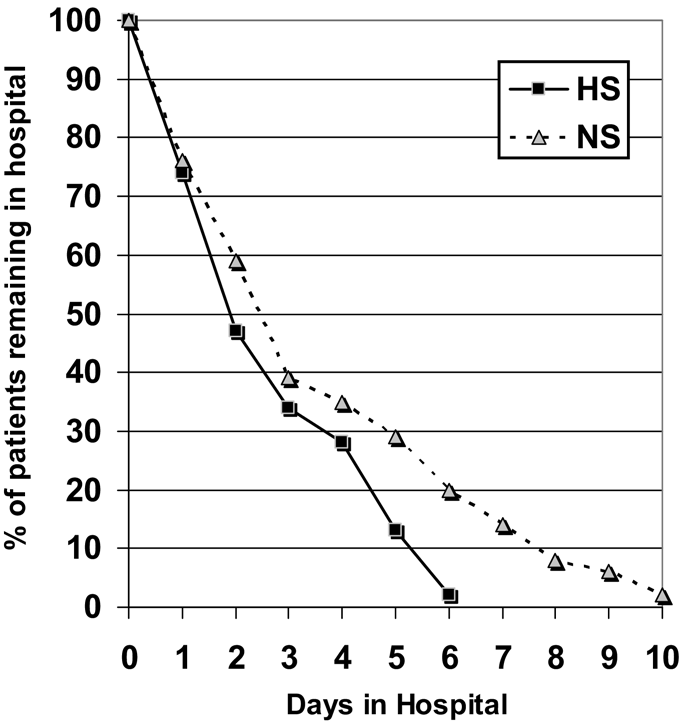
Figure. Percentage of patients in each group remaining in the hospital.
co-administration with a bronchodilator is often recom-
with albuterol), which was not associated with a significant
mended,others have reported that inhalation of 4.5% to
change in her respiratory status. She was eventually dis-
7% HS (without a bronchodilator) can be performed safely in
healthy nonasthmatic childrenor in children with mod-erately severe small airway obstruction secondary to cystic
Response to Therapy
In our study, there were no apparent adverse effects
The endpoint of LOS was identified by the attending
attributable to the use of HS without a bronchodilator, al-
physician using clinical grounds alone (45% of patients) or by
though the numbers were insufficient to allow further explo-
reaching protocol-established discharge criteria as measured
ration of this issue. However, there was no increase in add-on
by the study physician (55% of patients), whichever came first.
bronchodilator therapy in the treatment group, suggesting
One-way ANOVA confirmed that the LOS did not differ
that the use of HS in this setting was not associated with a
significantly between study sites for either the NS group (P ϭ
clinically significant increase in lower airway obstruction.
.12) or the HS group (P ϭ .44).
The use of inhaled HS in the treatment of viral bron-
Infants in the control group had a mean LOS of 3.5 Ϯ
chiolitis in hospitalized infants is a novel therapy that was first
2.9 days, whereas infants treated with nebulized 3% HS were
reported in and recently strengthened with the pub-
discharged on average 1 day sooner, with a 26% reduction in
lication of a 2-year extension of the original These
LOS to 2.6 Ϯ 1.9 days (P ϭ .05). There was a trend toward
authors demonstrated that 3 times a day dosing with 4 mL of
greater improvement in infants under age 6 months, but this
3% HS containing 1.5 mg of epinephrine compared with the
difference did not attain statistical significance (P ϭ .17). The
same dose of epinephrine in NS reduced the LOS from 3.6 Ϯ
percentage of patients from each group remaining in hospital
1.6 days to 2.8 Ϯ 1.3 days, a 22% improvement (P Ͻ .05).
They included epinephrine to prevent possible adverse effectsof HS and attributed the beneficial effects in the treatment
group to the presence of HS. Our study was very similar but
This study demonstrates that inhaled 3% HS is an
differed primarily in the inclusion of slightly older infants (up
effective treatment for infants up to age 18 months hospital-
to age 18 months), plus the much more frequent dosing of HS
ized with viral bronchiolitis. Repeated inhalations of nebu-
(9.1 Ϯ 3.0 inhalations/day). In our hands, increasing the
lized HS reduced the LOS by approximately 1 day, from
frequency of inhaled HS produced a further reduction in the
3.5 Ϯ 2.9 to 2.6 Ϯ 1.9 days. This is a clinically relevant benefit
LOS to 26%, but this reduction was not significant compared
with the potential for widespread impact on the treatment of
The routine use of 3% HS in the treatment of infants
The infants that we studied came from a population
hospitalized with bronchiolitis has the potential for enormous
that was geographically and ethnically very diverse. Neverthe-
economic benefit. A 26% reduction in LOS not only will
less, these infants were very similar to those described in other
return infants to home and their parents to work a day sooner,
Nebulized Hypertonic Saline in the Treatment of Viral Bronchiolitis in Infants
but also will also substantially reduce hospital costs. The
19. Patel H, Platt R, Lozano JM, Wang EEL. Glucocorticoids for acute viral bron-
estimated hospital costs for bronchiolitis in the US, which
chiolitis in infants and young children. Cochrane Database Syst Rev 2004:CD004878. 20. Bulow SM, Nir M, Levin E, Friis B, Thomsen LL, Nielsen JE, et al. Prednisolone
includes the widespread use of bronchodilators nebulized with
treatment of respiratory syncytial virus infection: a randomized controlled trial of 147
substitution of NS with the comparably priced 3% HS, with
21. van Woensel JB. Long-term effects of prednisolone in the acute phase of bron- chiolitis caused by respiratory syncytial virus. Pediatr Pulmonol 2000;30:92-6.
the subsequent reduction in LOS, has the potential to save
22. King VJ, Viswanathan M, Bordley C, Jackman AM, Sutton SF, Lohr KN, et al.
the US healthcare system more than $150 million annually.
Pharmacologic treatment of bronchiolitis in infants and children: a systematic review.
In summary, inhaled 3% HS is a safe, inexpensive, and
Arch Pediatr Adolesc Med 2004;158:127-37. 23. Elkins MR, Robinson M, Rose BR, Harbour C, Moriarty CP, Marks GB, et al.
effective treatment for previously well infants admitted to the
A controlled trial of long-term inhaled hypertonic saline in patients with cystic fibrosis.
hospital with moderately severe viral bronchiolitis. Further
research is needed to determine the optimum dosing and to
24. Eng PA, Morton J, Douglass JA, Riedler J, Wilson J, Robertson CF. Short-term efficacy of ultrasonically nebulized hypertonic saline in cystic fibrosis. Pediatr Pulmonol
identify whether there is any benefit from co-administered
25. Riedler J, Reade T, Button B, Robertson CF. Inhaled hypertonic saline increases sputum expectoration in cystic fibrosis. J Paediatr Child Health 1996;32:48-50. We thank Jaishen Rajah, Senior Consultant in Paediatrics,26. Suri R, Grieve R, Normand C, Metcalfe C, Thompson S, Wallis C, et al. Effects of hypertonic saline, alternate day and daily rhDNase on healthcare use, costs and SKMC, for his initial statistical guidance.
outcome in children with cystic fibrosis. Thorax 2002;57:841-6. 27. Robinson M, Hemming AL, Regnis JA, Wong AG, Bailey DL, Bautovich GJ,
et al. Effect of increasing doses of hypertonic saline on mucociliary clearance in patientswith cystic fibrosis. Thorax 1997;52:900-3.
Gleazen WP, Denny FW. Epidemiology of acute lower respiratory disease in
28. Tomooka LT, Murphy C, Davidson TM. Clinical study and literature review of
children. N Engl J Med 1973;288:498-505.
nasal irrigation. Laryngoscope 2000;110:1189-93.
Ray CG, Minnich LL, Holberg CJ, Shehad ZM, Wright AL, Barton LL, et al. 29. Tal G, Cesar K, Oron A, Houri S, Ballin A, Mandelberg A. Hypertonic saline/
Respiratory syncytial virus–associated lower respiratory illnesses: possible influence of
epinephrine treatment in hospitalized infants with viral bronchiolitis reduces hospital-
other agents. Pediatr Infect Dis 1993;12:15-9.
izations stay: 2 years experience. IMAJ 2006;8:169-73.
Smyth RL, Openshaw PJM. Bronchiolitis. Lancet 2006;368:312-22. 30. Sarrell E, Tal G, Witzling M, Someck E, Houri S, Cohen HA, et al. Nebulized
Hall CB. RSV and parainfluenza virus. N Engl J Med 2001;344:1917-28.
3% hypertonic saline solution treatment in ambulatory children with viral bronchiolitis
McConnochie KM, Roghmann KJ, Liptak GS. Hospitalization for lower respi-
decreases symptoms. Chest 2002;122:2015-20.
ratory tract illness in infants: variation in rates among counties in New York State and
31. Wainright C, Altamirano L, Cheney M, Cheney J, Barber S, Price D, et al. A
areas within Monroe Counties. J Pediatr 1995;126:220-9.
multicentre, randomized, double-blind, controlled trial of nebulized epinephrine in
Pelletier AJ, Mansbach JM, Camargo CA. Direct medical costs of bronchiolitis
infants with acute bronchiolitis. N Engl J Med 2003;349:27-35.
hospitalizations in the United States. Pediatrics 2006;118:2418-23. 32. Patel H, Platt RW, Pekeles GS, Ducharme FM. A randomized controlled trial of
Wright RB, Pomerantz WJ, Luria JW. New approaches to respiratory infections
the effectiveness of nebulized therapy with epinephrine compared with albuteral and
in children: bronchiolitis and croup. Emer Med Clin North Am 2002;20:93-114.
saline in infants hospitalized for acute viral bronchiolitis. J Pediatr 2002;141:818-24.
Subcommittee on Diagnosis and Management of Bronchiolitis, American Acad-
33. Ray MS. Comparison of nebulized adrenaline versus salbutamol in wheeze asso-
emy of Pediatrics. Diagnosis and management of bronchiolitis. Pediatrics 2006;
ciated with respiratory tract infection in infants. Indian Pediatr 2002;39:12-22. 34. Lowell DI, Lister G, Von Koss H, McCarthy P. Wheezing in infants: the
Welliver JR, Welliver RC. Bronchiolitis. Pediatr Rev 1993;14:134-9.
response to epinephrine. Pediatrics 1987;79:939-45. 10. Aherne W, Bird T, Court SDM, Gardner PS, McQuillin J. Pathological changes 35. Cheney J, Barber S, Altamirano L, Cheney M, Williams C, Jackson M, et al. A
in viral infections of the lower respiratory tract in children. J Clin Pathol 1970;23:7-18.
clinical pathway for bronchiolitis is effective in reducing readmission rates. J Pediatr
11. Kostagal UR, Robbins JM, Kini NM, Schoettker PJ, Atherton HD, Kirschbaum
MS. Impact of a bronchiolitis guideline: a multi-site demonstration project. Chest
36. Todd J, Bertock D, Dolan S. Use of a large national database for comparative
evaluation of the effect of a bronchiolitis/viral pneumonia clinical care guidelines on
12. Christakis DA, Cowan CA, Garrison MM, Molteni R, Marcuse E, Zerr DM.
patient outcome and resource utilization. Arch Pediatr Adolesc Med 2002;156:1086-90.
Variation in inpatient diagnostic testing and management of bronchiolitis. Pediatrics
37. Menon K, Sutcliffe T, Klassen TP. A randomized trial comparing the efficacy of
epinephrine with salbutamol in the treatment of acute bronchiolitis. J Pediatr
13. Kellner JD, Ohlsson A, Gadomski AM, Wang EEL. Efficacy of bronchodilator
therapy in bronchiolitis: a meta-analysis. Arch Pediatr Adolesc Med 1996;150:1166-72. 38. Cataldo D, Foidant JM, Lau L, Bartsch P, Djukanovic R, Louis R. Induced 14. Kellner JD, Ohlsson A, Gadomski AM, Wang EEL. Bronchodilators for bron-
sputum: comparison between isotonic and hypertonic saline solution in patients with
chiolitis. Cochrane Database Syst Rev 2000;CD001266. 15. Flores G, Horwitz RI. Efficacy of beta-2 agonists in bronchiolitis: a reappraisal 39. Mandelberg A, Tal G, Witzling M, Someck E, Houri S, Balin A, et al. Nebulized
and meta-analysis. Pediatrics 1997;100:233-9.
3% hypertonic saline solution treatment in hospitalized infants with bronchiolitis. Chest
16. Schuh S, Coates AL, Binnie R, Allin T, Goia C, Corey M, et al. Efficacy of oral
dexamethasone in outpatients with acute bronchiolitis. J Pediatr 2002;140:27-32. 40. Araki H. Inhalation of hypertonic saline as a bronchial challenge in children with 17. Csonka P, Kaila M, Laippala P, Iso-Mustajarvi M, Vesikari T, Ashorn P. Oral
mild asthma and normal children. J Allergy Clin Immunol 1989;84:99-107.
prednisolone in the acute management of children age 6 to 35 months with viral
41. Williams PV. Inhalation bronchoprovocation in children. Immunol Clin North
respiratory infection-induced lower airway disease: a randomized, placebo-controlled
42. Suri R, Marchall LJ, Wallis C, Mecalfe C, Shute JK, Bush A. Safety and use of 18. Weinberger M. Oral prednisolone in the acute management of children age 6 to
sputum induction in children with cystic fibrosis. Pediatr Pulmonol 2003;35:309-13.
35 months with viral respiratory infection–induced lower airway disease: a randomized,
43. Friedman SM. The inflation calculator. Available at
placebo-controlled trial. J Pediatr 2004;145:137-8.
The Journal of Pediatrics • September 2007
Table II. Site-specific patient demographics and Table IV. Site-specific treatments received illness status at baseline KGH ؉ VGH VGH ؉ KGH Treatment (n ؍ 64)* (n ؍ 32)* P (n ؍ 64)* (n ؍ 32)* P
*Sample sizes vary slightly for the individual comparisons due to missing data.
*Sample sizes vary slightly for the individual comparisons due to missing data.
Nebulized Hypertonic Saline in the Treatment of Viral Bronchiolitis in Infants
No. 29 (2/00) PSYCHIATRIC MEDICATION FOR CHILDREN AND ADOLESCENTS PART II: TYPES OF MEDICATIONS Psychiatric medications can be an effective part of the treatment for psychiatric disorders of childhood and adolescence. In recent years there have been an increasing number of new and different psychiatric medications used with children and adolescents. Research studies are underway
SPECIAL ONE TIME SETTLEMENT SCHEME (OTS) FOR NPA ACCOUNTS IN MSME SECTOR Coverage of the Scheme • The approved policy will also cover eligible cases in which the Bank has initiated actions under SARFAESI Act, cases pending before Courts/ DRTs /Lok Adalat and decreed accounts subject to obtaining consent decree from the Court/ DRT/ Lok Adalat. • The approved OTS scheme will cover
 bronchiolitis studies, with a slight male predominance (62%),primary infection with RSV (69%), mean age of 4.7 months,and LOS in the control group of 3.5 to 4 Strictinclusion and discharge criteria were used to minimize pos-sible confounding effects of uncharacterized and evolvingwheezing phenotypes and to minimize between-site variabil-ity. The clinical scoring system chosen has been widely usedin other studies on and has been proposedto be the scoring system of choice for further studies.Therefore, our findings should be universally applicable toother previously healthy infants hospitalized with moderatelysevere viral bronchiolitis.
bronchiolitis studies, with a slight male predominance (62%),primary infection with RSV (69%), mean age of 4.7 months,and LOS in the control group of 3.5 to 4 Strictinclusion and discharge criteria were used to minimize pos-sible confounding effects of uncharacterized and evolvingwheezing phenotypes and to minimize between-site variabil-ity. The clinical scoring system chosen has been widely usedin other studies on and has been proposedto be the scoring system of choice for further studies.Therefore, our findings should be universally applicable toother previously healthy infants hospitalized with moderatelysevere viral bronchiolitis.