Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Microsoft word - 25f ijab-09-333, 133-136
INTERNATIONAL JOURNAL OF AGRICULTURE & BIOLOGY ISSN Print: 1560–8530; ISSN Online: 1814–9596 09–333/ZIP/2010/12–1–133–136 http://www.fspublishers.org
Full Length Article Effect of Pioglitazone on Glucose and Glycation Level in Type 2 Diabetic Patients MUHAMMAD ALIM1, RAKHSHANDA NAWAZ, MUHAMMAD RAFIQUE ASI†, FAROOQ ANWAR AND TAHIRA IQBAL Department of Chemistry and Biochemistry, University of Agriculture, Faisalabad-38040, Pakistan †Nuclear Institute for Agriculture and Biology (NIAB), Faisalabad, Pakistan Corresponding author’s e-mail: prof_alim68@yahoo.com ABSTRACT To elucidate the effects of pioglitazone treatment on glucose and glycation level in patients with type 2 diabetes, a total of 8 patients were treated with pioglitazone (30 mg day-1) for 12 weeks. After this period, there was a significant decrease in fasting plasma glucose and glycation level. The fasting plasma glucose was decreased from 195 to 159 mg per dL and glycation level decreased from 0.140 to 0.113 moles of glucose per moles of protein. These results suggest that pioglitazone decreases fasting plasma glucose in type 2 diabetic patients and acts as an inhibitor of glycation in-vivo. 2010 Friends Science Publishers Key Words: Pioglitazone; Glycation; Diabetic; Inhibitor INTRODUCTION
increases transcription of insulin responsive genes and thus
increases insulin sensitivity (Scholz et al., 2001).
Diabetes mellitus commonly referred to as “diabetes”
Most of the drugs metabolizing genes show different
is a group of metabolic diseases characterized by
activities in different populations, which are often major
abnormalities at multiple organ sites. These defects include
determinants of variable drug exposure and response
insulin secretion, insulin action or both (Barnett, 2007).
(Flockhart & Desta, 2009). Moreover individuals can differ
There are different forms of diabetes mellitus but type 2
greatly in their inherent capacity to absorb, distribute,
diabetes is the most common. It is also known as the non-
excrete and metabolize drugs (Vesell, 1974). To accomplish
insulin dependent diabetes mellitus (NIDDM) and occurs as
the clinical benefits, safe and effective drug therapy is
a result of progressive insulin secretory defect on the
difficult due to large inter-patient variability in response to
background of insulin resistance (American Diabetes
many drugs (Flockhart & Desta, 2009). The values of
Association, 2009). About 90 to 95% of people suffering
biochemical and physiological parameters present in the
from this disease have type 2 diabetes (DeFronzo, 1997).
literature are not inline with the values calculated under our
Without proper management many complications arise
own environmental conditions. Therefore for the welfare of
under hyperglycemic conditions. A high glucose humanity it is very necessary to generate information in our concentration increases protein glycation, also known as
population to develop our own therapeutic standards under
non-enzymatic glycosylation in blood and various organs
(Krishmanurti & Steffes, 2001). These non-enzymatic
Pioglitazone has been studied rarely and its effect on
reactions between reducing sugars and free amino groups of
glycation level has been reported only from few countries.
proteins can alter the structure and function of proteins
Moreover glycation research remains an area of outstanding
(Hartog et al., 2007) and result in the formation of advanced
interest, fascination and innovation in chemistry, biology,
glycation end products (Ulrich & Cerami, 2001).
medicine, food, nutrition and applied sciences. Therefore
Pioglitazone (±) 5-{[4-[2-(5-ethyl-2-pyridinyl) ethoxy]
the present project was designed to widen our knowledge
phenyl] methyl}-2, 4-thiazolidinedione is an oral anti-
about pioglitazone (an anti-diabetic) in Pakistani patients
hyperglycemic agent, which is used in the treatment of type
2 diabetes (Gillies & Dunn, 2000). It belongs to a class
Study Design and Methods
“thiazolidinediones", represent a potentially important group
Subjects: A total of eight type 2 diabetic patients, clinically
of drugs with a mechanism of action differing from the
diagnosed by physicians, were recruited from the outpatient
existing therapies (Yki-Jarvinen, 2004). It acts primarily by
medicine clinic of the General Hospital Faisalabad,
decreasing insulin resistance in the treatment of type 2
Pakistan. They were recommended diet and exercise at
diabetes (Radhakrishna et al., 2002). It is a peroxisome
initial stage to control the diabetes. Patients who had
proliferator activated receptor (PPARγ) agonist that
previously received insulin, metformin, thiazolidinedione or
To cite this paper: Alim, M., R. Nawaz, M.R. Asi, F. Anwar and T. Iqbal, 2010. Effect of pioglitazone on glucose and glycation level in type 2 diabetic patients. Int. J. Agric. Biol., 12: 133–136
ALIM et al. / Int. J. Agric. Biol., Vol. 12, No. 1, 2010
any other medicine related to diabetes were excluded. Entry
Table I: Demographic data of diabetic patients
criteria included age (35-55) years and weight (55-85 kg).
Patients were in good general health without cardiac,
Subject Age Weight Height Blood Pressure Body BMI*
hepatic, renal or other chronic diseases. The demographic
No. ID Years Kg Inches Systolic Diastolic °F
and clinical data of the patients is presented in Tables I and
Study design: The study was conducted for 12 weeks by
keeping in view the ethical principles laid down in the
Declaration of Helsinki (World Medical Association, 2004).
Initially subject’s education was updated and their ability to
comply with the protocol was checked. The subjects were
instructed to take balanced diet during study period. All
subjects gave signed, informed consent before participation
Subscript ‘P’ stands for patient, *BMI is Body Mass Index
Plasma collection: Blood samples from each patient after Fig. 1: Change in concentration of glucose in diabetic
every 15 days, up to 12 weeks were collected by using
patients
sterilize disposable syringes by venopuncture in pre-
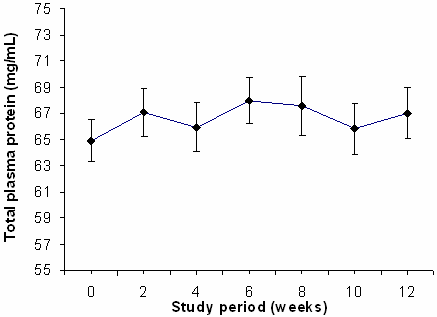
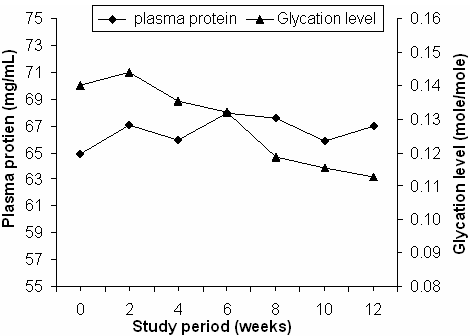
heparinised centrifuge tubes 10 mL Vacuette® Griener Bio- one, Austria. These samples were mixed gently and were then centrifuge at 4000 rpm and plasma was stored at – 20°C. Analysis techniques: In plasma samples amount of glucose was estimated by Kit method, protein concentration by Biuret method and glycation level by Thiobarbituric acid (TBA) method as described by Furth (1988), spectrophotometrically. Statistical analysis: For computation and the graphics, the Microsoft Excel 7.0 was used. All data are reported as the mean±SE (Steel et al., 1997). Fig. 2: Change in concentration of plasma proteins in diabetic patients
The results illustrating the effect of pioglitazone on
glucose concentration, proteins concentration and glycation level in diabetic patients are presented in the Figs. 1–5. In patients, there is regular decrease in the concentration of fasting plasma glucose (FPG). After 8th week, minimum concentration (159.0±3.30 mg dL-1) was obtained in comparison to 195.5±8.65 mg per dL detected at the start of the study. This level slightly increased to 163.0±4.64 mg per dL after 10th week and then declined to 159.38±4.65 mg per dL (Fig. 1). There is not gradual increase or decrease in the concentration of plasma proteins. These values changed randomly and maximum concentration 67.96±1.77 mg per
mL was achieved after 6th week and minimum value
DISCUSSION
65.83±1.93 mg per mL after 10th week (Fig. 2).
In patients, long term therapy with pioglitazone
Results indicate that long term therapy with
significantly decreased the glycation level. This level
pioglitazone have significant effect on FPG level in type 2
reduced gradually up to 12th week, but in last weeks value of
diabetic patients. This effect is more pronounced up to 8th
glycation level become consistent. Maximum glycation
week then concentration become almost constant. These
level (0.144±0.014 mole mole-1) was observed after 2nd
results are similar to the results reported in the literature.
week and minimum value 0.113±0.010 mole per mole was
Pioglitazone decrease blood glucose in diabetic animal
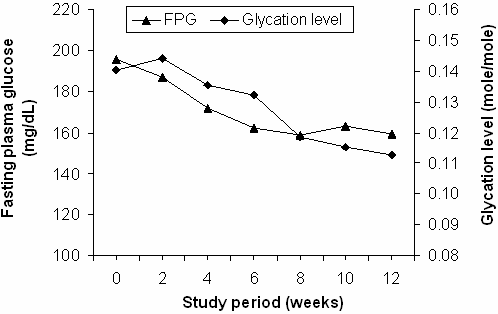
obtained after 12th week (Fig. 3). The trends between the
models (Saltiel & Olefsky, 1996) and in patients with type 2
change in fasting plasma glucose and glycation level and the
diabetes (Suter et al., 1992). In general decrease in plasma
change in concentration of proteins and glycation level are
glucose or improvement of insulin resistance by
pioglitazone requires several days in diabetic animals
EFFECT OF PIOGLITAZONE ON GLUCOSE/GLYCATION LEVEL IN DIABETIC PATIENTS / Int. J. Agric. Biol., Vol. 12, No. 1, 2010Table II: Clinical data of diabetic patients in the fasting state Subject Serum creatinine Triglycerides Hb Cholestrol SGPT Total protein TLC Neutrophils Lymphocytes dL-1 /cmm
Subscript ‘P’ stands for patient, Hb: hemoglobin, SGPT: Serum Glutamic-Pyruvic Transaminase, TLC: Total leucocyte count
(Saltiel & Olefsky, 1996) or several weeks in patients with
Fig. 3: Change in Glycation level in diabetic patients
type 2 diabetes (Iwamoto et al., 1991; Suter et al., 1992).
Aronoff et al. (2000) mentioned that the blood glucose lowering effect of pioglitazone developed gradually over weeks and maximum decrease was observed after 10-14 weeks. Pioglitazone have the ability to reduce both fasting and postprandial glucose levels (Suter et al., 1992; Ravikumar et al., 2008). After pioglitazone treatment, fasting and postprandial endogenous glucose production (EGP) decreased (16.6±1.0 vs. 12.2±0.7 µmol kg-1 min-1) and (2.58±0.25 vs. 1.26±0.30 µmol/Kg/min), respectively (Ravikumar et al., 2008). Rubin et al. (1999) also observed a decrease in FBG levels of up to 60 mg/dL in a
combination therapy. The results about the analysis of
plasma proteins illustrate that there is not regular increase or
Fig 4: Pattern between glycation level and
decrease in the concentration of proteins. These values
concentration of glucose in diabetic Patients
remain within the normal limits. This indicate that long term
treatment with pioglitazone have no effect on plasma proteins in type 2 diabetic patients.
The decrease in the glycation level after 12 weeks
treatment with pioglitazone is not surprising, because similar results are available in previous literature. As the pioglitazone significantly improves the glycemic control (Pavo et al., 2003; Umpierrez et al., 2006), therefore its inhibitory effect on glycation process can be explained in this scenario. As monotherapy, it improves the fasting blood glucose and glycosylated hemoglobin (Stratton et al., 2000; Pavo et al., 2003). On average, fasting blood glucose and
glycosylated hemoglobin can be improved by approximately
40 mg per dL and almost 1%, respectively (Stumvoll &
Fig. 5: Pattern between glycation level and
Haring, 2002). It was effective in reducing plasma glucose
concentration of proteins in diabetic patients
from the baseline levels from week 4 and this decrease
continued up to the last measurement at week 12 (Abe et al., 2007). In Wistar fatty rats, GHb levels declined gradually over 5 weeks administration of pioglitazone (Nagisa et al., 2003). It also acts as an important inhibitor of glycation and potent antioxidant (Rahbar et al., 2000; Gumieniczek, 2005). Moreover the pattern between the change in FPG and glycation level is quite similar, they show almost similar trends during the study. The pattern between change in concentration of proteins and glycation level in patients demonstrate that trend in the concentration change of plasma proteins is not similar to change in glycation level.
ALIM et al. / Int. J. Agric. Biol., Vol. 12, No. 1, 2010CONCLUSION
Pavo, I., G. Jermendy, T.T. Varkonyi, Z. Kerenyi, A. Gyimesi, S. Shoustov,
M. Shestakova, M. Herz, D. Johns, B.J. Schluchter, A. Festa and M.
Pioglitazone decreases the fasting plasma glucose
Tan, 2003. Effect of pioglitazone compared with metformin on glycemic control and indicators of insulin sensitivity in recently
level and acts as an inhibitor of glycation in type 2 diabetes
diagnosed patients with type 2 diabetes. J. Clin. Endocrinol. Metab.,
Acknowledgement: We acknowledge the support provided
Radhakrishna, T., D.R. Sreenivas and G.O. Reddy, 2002. Determination of
by the University of Agriculture, Faisalabad, Pakistan, in
pioglitazone hydrochloride in bulk and pharmaceutical formulations by HPLC and MEKC methods.
terms of equipment and laboratory facilities. Moreover we
J. Pharm. Biomed. Anal., 29: 593–
are grateful to the Higher Education Commission (HEC),
Rahbar, S., R. Natarajana, K.K. Yernenia, S. Scott, N. Gonzales and J.L.
Islamabad, Pakistan for finance of this research.
Nadler, 2000. Evidence that pioglitazone, metformin and pentoxifylline are inhibitors of glycation.
REFERENCES
Ravikumar, B., J. Gerrard, C.D. Man, M.J. Firbank, A. Lane, P.T.
English, C. Cobelli and R. Taylor, 2008. Pioglitazone decreases
Abe, M., F. Kikuchi, K. Kaizu and K. Matsumoto, 2007. Combination
fasting and postprandial endogenous glucose production in
therapy of pioglitazone with voglibose improves glycemic control
proportion to decrease in hepatic triglyceride content. Diabetes,
safely and rapidly in Japanese type 2 diabetic patients on
hemodialysis. Clin. Nephrol., 68: 287–294
Rubin, C., J. Egan and R. Schneider, 1999. Combination therapy with
American Diabetes Association, 2009. Standards of medical care in
pioglitazone and insulin in patients with type 2 diabetes. Diabetes,
diabetes. Diabetes Care, 32: S13–S61
Aronoff, S., S. Rosenblatt, S. Braithwaite, J.W. Egan, A.L. Mathisen and
Saltiel, A.R. and J.M. Olefsky, 1996. Thiazolidinediones in the treatment of
R.L. Schneider, 2000. Pioglitazone hydrochloride monotherapy
insulin resistance and type 2 diabetes. Diabetes, 45: 1661–1669
improves glycemic control in the treatment of patients with type 2
Scholz, G.H., W.A. Scherbaum and G. Lubben, 2001. Pioglitazone a review
diabetes: A 6 month randomized placebo-controlled dose-response
of preclinical data. Diabetes Stoffwechsel, 9: 23–30
study. Diabetes Care, 23: 1605–1611
Steel, R.G.D., J.H. Torrie and D.A. Dickey, 1997. Principles and
Barnett, A.H., 2007. Summarising the use of thiazolidinediones with
Procedures of Statistics: A Biomaterical Approach. Mc Graw Hill
insulin. British J. Diabetes Vasc. Dis., 7: 75–80
DeFronzo, R.A., 1997. Pathogenesis of type 2 diabetes: Metabolic and
Stratton, I.M., A.I. Adler, H.A. Neil, D.R. Matthews, S.E. Manley, C.A.
molecular implication for identifying diabetes genes. Diabetes Rev.,
Cull, D. Hadden, R.C. Turner and R.R. Holman, 2000. Association
of glycemia with macrovascular and microvascular complications of
Flockhart, D.A. and Z. Desta, 2009. Pharmacogenetics of Drug
type 2 diabetes (UKPDS 35): Prospective observational study. BMJ,
Metabolism, pp: 301–317. Clinical and Translational Science
Furth, A.J., 1988. Methods for assaying non-enzymatic glycosylation: A
Stumvoll, M. and H.U. Haring, 2002. Glitazones: Clinical effects and
review. Annal. Biochem., 175: 347–360
molecular mechanisms. Annl. Med., 34: 217–224
Gillies, P.S. and C.J. Dunn, 2000. Pioglitazone. Drugs, 60: 333–343
Suter, S.L., J.J. Nolan, P. Wallace, B. Gumbiner and J.M. Olefsky, 1992.
Gumieniczek, A., 2005. Effects of pioglitazone on hyperglycemia induced
Metabolic effects of new oral hypoglycemic agent CS-045 in
alterations in antioxidative system in tissues of alloxan-treated
NIDDM subjects. Diabetes Care, 15: 193–203
diabetic animals. Exp. Toxicol. Pathol., 56: 321–326
Ulrich, P. and A. Cerami, 2001. Protein glycation, diabetes and aging.
Hartog, J.W.L., A.A. Voors, S.J.L. Bakker, A.J. Smit and D.J. Veldhuisen,
Recent. Prog. Horm. Res., 56: 1–21
2007. Advanced glycation end products (AGEs) and heart failure:
Umpierrez, G., M. Issa and A. Vlajnic, 2006. Glimepiride versus
Pathophysiology and clinical implications. European J. Heart
pioglitazone combination therapy in subjects with type 2 diabetes
inadequately controlled on metformin monotherapy: results of a
Iwamoto, Y., T. Kuzuya, A. Matsuda, T. Awata, S. Kumakura, G. Inooka
randomized clinical trial. Curr. Med. Res. Opin., 22: 751–759
and I. Shiraishi, 1991. Effect of a new oral anti-diabetic agent CS-
Vesell, E.S., 1974. Relationship between drug distribution and therapeutic
045 on glucose tolerance and insulin secretion in patients with
effects in man. Annu. Rev. Pharmacol., 14: 249–270
NIDDM. Diabetes Care, 14: 1083–1086
World Medical Association, 2004. Declaration of Helsinki: Ethical
Krishmanurti, U. and M.W. Steffes, 2001. Glycohemoglobin: A primary
Principles for Medical Research Involving Human Subjects. 55th
predictor of the development or reversal of complications of diabetes
mellitus. Clin. Chem., 47: 1157–1165
Yki-Jarvinen, H., 2004. Thiazolidinediones. N. England J. Med., 351:
Nagisa, Y., K. Kato, K. Watanabe, H. Murakoshi, H. Odaka, K. Yoshikawa
and Y. Sugiyama, 2003. Changes in glycated hemoglobin levels in
diabetic rats measured with an automatic affinity HPLC. Clin. Exp. (Received 26 September 2009; Accepted 10 October 2009) Pharmacol. Physiol., 30: 752–758
PEDIATRIC EMERGENCY DEPARTMENT OUTCOMES COMPARING LEVALBUTEROL VS. RACEMIC ALBUTEROL Timothy R. Myers BS, RRT, Marsha Rogers CRT, John C. Carl MD, Carolyn Kercsmar MD. Rainbow Babies & Children’s Hospital. Cleveland, Ohio. Background : Pediatric asthma is a chronic condition of childhood with increasing prevalence. Emergency Department (ED) treatment of asthma constitutes a failu
LA LIBERTÉ JEUDI 28 FÉVRIER 2013 Federer domine Michael Brügger, ce héros Granollers SKI-HANDICAP • Le Singinois rentre des championnats du monde de La Molina avec Roger Federer (ATP 2) sera bien présent au trois médailles autour du cou: l’argent de la descente, le bronze du super-G et du géant. stade des quarts de finale à Dubai. Contraint dedisputer
 INTERNATIONAL JOURNAL OF AGRICULTURE & BIOLOGY ISSN Print: 1560–8530; ISSN Online: 1814–9596 09–333/ZIP/2010/12–1–133–136 http://www.fspublishers.org
Full Length Article
INTERNATIONAL JOURNAL OF AGRICULTURE & BIOLOGY ISSN Print: 1560–8530; ISSN Online: 1814–9596 09–333/ZIP/2010/12–1–133–136 http://www.fspublishers.org
Full Length Article 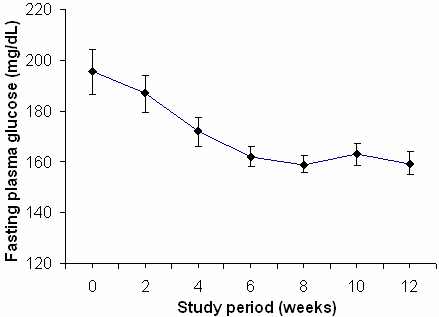
 ALIM et al. / Int. J. Agric. Biol., Vol. 12, No. 1, 2010
any other medicine related to diabetes were excluded. Entry
Table I: Demographic data of diabetic patients
ALIM et al. / Int. J. Agric. Biol., Vol. 12, No. 1, 2010
any other medicine related to diabetes were excluded. Entry
Table I: Demographic data of diabetic patients 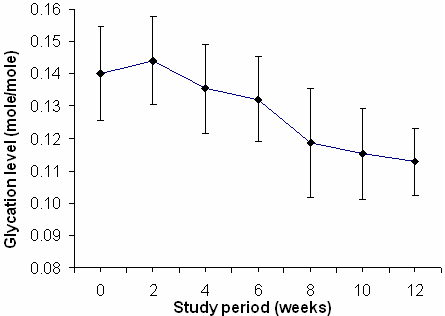
 EFFECT OF PIOGLITAZONE ON GLUCOSE/GLYCATION LEVEL IN DIABETIC PATIENTS / Int. J. Agric. Biol., Vol. 12, No. 1, 2010
Table II: Clinical data of diabetic patients in the fasting state
EFFECT OF PIOGLITAZONE ON GLUCOSE/GLYCATION LEVEL IN DIABETIC PATIENTS / Int. J. Agric. Biol., Vol. 12, No. 1, 2010
Table II: Clinical data of diabetic patients in the fasting state