Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
102527 341.348
Human Reproduction Update, Vol.10, No.4 pp. 341–348, 2004Advance Access publication June 10, 2004.
Mechanisms of action of mifepristone and levonorgestrelwhen used for emergency contraception
Department of Woman and Child Health, Division of Obstetrics and Gynecology, Karolinska Hospital/Institute,S-171 76 Stockholm, Sweden
1To whom correspondence should be addressed. E-mail: kristina.gemzell@kbh.ki.se
An emergency contraceptive method is used after coitus but before pregnancy occurs. The use of emergency con-traception is largely under-utilized worldwide. One of the main barriers to widespread use is concern about themechanism of action. Recently, treatment with either 10 mg mifepristone or 1.5 mg of levonorgestrel has emergedas the most effective hormonal method for emergency contraception with very low side-effects. However, theknowledge of the mechanism of action of mifepristone and levonorgestrel in humans, when used for contraceptivepurposes and especially for emergency contraception, remains incomplete. The objective of this review is to sum-marize available data on the effects of mifepristone and levonorgestrel on female reproductive functions relevantto the emergency use of the compounds. When summarized, available data from studies in humans indicate thatthe contraceptive effects of both levonorgestrel and mifepristone, when used in single low doses for emergency con-traception, involve either blockade or delay of ovulation, due to either prevention or delay of the LH surge, ratherthan to inhibition of implantation.
Key words: emergency contraception/endometrium/levonorgestrel/mifepristone/ovulation
given within 72 h of the intercourse and repeated after 12 h(Yuzpe and Lance, 1977). The Yuzpe regimen has since been the
Emergency contraception (EC) is defined as the use of any drug
most commonly used method. Other available methods today are
or device used after an unprotected intercourse to prevent an
the administration of levonorgestrel 0.75 mg, repeated after 12 h
unwanted pregnancy. The use of emergency contraception is
or in a single dose of 1.5 mg, as a single dose of 10 mg mifepris-
largely under-utilized worldwide. Emergency contraception has
tone (only available in China), or insertion of a copper intrauter-
been called ‘one of the best kept secrets in family planning’.
ine device (IUD) (Lippes et al., 1979).
One of the main barriers to widespread use is the concern about
Recently, treatment with levonorgestrel only and mifepristone
the mechanisms of action, such as impairment of implantation,
has emerged as the most effective hormonal method with very
or dislodgement of an implanted fetus. Emergency contraception
low side-effects and higher efficacy than the standard Yuzpe
is frequently confused with induced abortion. In many develop-
regimen [World Health Organization (WHO), 1998, 1999].
ing countries, the lack of knowledge about and access to emer-
Following these studies, levonorgestrel 1.5 mg has become the
gency contraception may result in women resorting to unsafe
recommended regimen. The hormonal methods are usually also
abortions, which contribute significantly to maternal mortality
considered as more convenient than the insertion of a copper
and morbidity. It has been estimated that millions of unwanted
IUD which is otherwise the most effective method. When
pregnancies could be avoided if emergency contraception were
600 mg of mifepristone was administered within 72 h of an
widely accessible (Consensus statement of emergency contracep-
unprotected intercourse, no pregnancy occurred among 597
tion, 1995). An understanding of the mechanism of action
women treated (Glasier et al., 1992; Webb et al., 1992). The
of contraceptive methods is essential for the development of
efficacy was shown to be higher than with the Yuzpe regimen
new methods as well as for optimizing the use of those already
and the incidence of side-effects such as nausea and vomiting
available. This knowledge may also influence religious, cultural
was significantly decreased. However, a delay in the return of
and individual acceptability of contraceptive methods.
the menstrual bleeding was more commonly observed after mife-
Trials on emergency contraception were first described in
pristone. In the study by Webb et al. (1992), three women who
the 1930s using high doses of stilbestrol (Morris and van
conceived after treatment but before follow-up were excluded.
Wagenen, 1966). In the late 1970s Yuzpe introduced a regimen
When the dose of mifepristone was reduced to 50 or 10 mg,
consisting of 0.1 mg ethinylestradiol and 0.5 mg levonorgestrel,
Human Reproduction Update Vol. 10 No. 4 q European Society of Human Reproduction and Embryology 2004; all rights reserved
K.Gemzell-Danielsson and L.Marions et al.
the efficacy was shown to be the same as with the higher dose,
the first events observed following the binding of progesterone
but the delay of the next menses was clearly shortened in a
to the sperm cell. There are conflicting results on the effect of
dose-dependent manner. Also, the interval from coitus to treat-
mifepristone on sperm functions in vitro. Some authors report
ment could be extended to 120 h and, in contrast to the Yuzpe
that the influx of calcium and the acrosome reaction can be
regimen and levonorgestrel, there seemed to be no decrease in
inhibited by mifepristone (Serres et al., 1994; Yang et al., 1994).
efficacy with time (WHO, 1999). However, in a more recent
However, it has also been reported that mifepristone is ineffec-
study comparing 25 and 10 mg of mifepristone given within
tive in inhibiting the progesterone-mediated calcium increase in
120 h of an unprotected intercourse, both doses were equally
sperm (Blackmore et al., 1991). A single dose of 200 mg mife-
effective in preventing pregnancy but efficacy decreased with
pristone when given to 12 healthy, male volunteers did not
treatment delay (Xiao et al., 2002). The efficacy of 10 mg of
seem to affect baseline levels of sperm intracellular calcium or
mifepristone was tested further and compared to levonorgestrel,
the capacity of sperm to increase intracellular calcium following
0.75 mg twice with a 12 h interval or in a single dose of 1.5 mg
exposure to progesterone (our unpublished data). Incubation of
(von Hertzen et al., 2002). Pregnancy rates did not differ
sperm samples with 100 mmol/l mifepristone during capacitation
between mifepristone and levonorgestrel treatment in divided or
led to a decrease in basal intracellular calcium levels but the
single doses when taken within 5 days of unprotected intercourse
response to progesterone was unaffected. Results from our
(1.5%). Side-effects were mild and similar between treatment
studies indicate that mifepristone may decrease basal intracellu-
groups. Women who took levonorgestrel had earlier menses than
lar calcium levels of capacitated sperm. The concentration of
those who took mifepristone. An advance in the next menses of
mifepristone required to cause such an effect is, however, several
. 7 days occurred in 15% of women following levonorgestrel
times higher than the drug level reached in seminal plasma after
and 9.4% following mifepristone while a delay in the next
treatment of male volunteers in vivo (our unpublished data).
menses of . 7 days occurred in 5 and 9% for levonorgestrel andmifepristone respectively.
In all WHO studies, efficacy was calculated as ‘intention-to-
Kesseru¨ et al. (1974) showed that treatment with 0.4 mg of
treat’ which means that all pregnancies were included, even
levonorgestrel within 3 – 10 h of an unprotected intercourse had a
those resulting from intercourse after treatment but before
number of effects. It decreased the number of sperm recovered
from the uterine cavity beginning 3 h after treatment, caused
Although both mifepristone and levonorgestrel are highly
pronounced alkalization of the intrauterine fluid beginning at 5 h,
effective when used for emergency contraception, the knowledge
which immobilized the sperm, and increased the viscosity of
of the mechanism underlying these effects remains incomplete.
the cervical mucus, beginning at 9 h after treatment. Effects
The objective of this review is to summarize available data on
described on sperm function in vitro seem to be dose dependent
the effect of mifepristone and levonorgestrel on female repro-
and results are slightly divergent. Yeung et al. (2002) reported a
ductive functions relevant to emergency use of the compound.
dose-dependent effect on zona-binding capacity and sperm
Unprotected intercourse may occur, and emergency contracep-
velocity but no effect on acrosome reaction after exposure of
tion may be used, at any time during the menstrual cycle but it
human sperm to levonorgestrel whereas a dose-dependent
is only during a limited period, from , 5 days before to 1 day
increase in the rate of acrosome reaction was noted in another
after ovulation that unprotected intercourse may result in a preg-
nancy (Wilcox et al., 1995). To be effective, postcoital treatment
Taken together, these data indicate that levonorgestrel or
could theoretically target one or several of the following events:
mifepristone in doses relevant for emergency contraception have
sperm transport and function, follicular development, ovulation,
no direct effect on sperm function. The observations described
fertilization, embryo development and transport, endometrial
by Kesseru¨ et al. are probably of importance when levonorges-
trel is used as a regular contraceptive but unlikely to be the main
(Table I). In the following we address the effects of mifepristone
mechanism of action of levonorgetrel used for EC since sperm
and levonorgestrel on each of these reproductive processes
can be retrieved from the Fallopian tube within min after insemi-nation (Kunz et al., 1996).
Effects on human sperm transport and function
Progesterone triggers the acrosome reaction of capacitated
human sperm in vitro. A rise in intracellular calcium is one of
The effect of mifepristone during the menstrual cycle is well
Table I. Possible targets for emergency contraception
known to be dependent on the dose given and the time of treat-ment. Administration of mifepristone during the pre-ovulatory
phase of the menstrual cycle either disrupts follicular develop-
ment or inhibits ovulation. A low dose (, 50 mg) of mifepristone
may lead to a delay in follicular maturation, which, as soon as
the influence of mifepristone is over, continues to an ovulation
that will be delayed. Alternatively, ovulation returns when a new
Endometrial receptivity and implantationCorpus luteum
leading follicle has been recruited. The follicle may also remainunruptured until the end of the cycle. When ovulation occurs,
Emergency contraception: mechanisms of action
the following luteal phase seems to be normal with normal endo-
continued to grow, exceeding the size seen in the control cycle,
metrial development and function, as judged by implantation
and the LH surge was delayed. Follicular rupture occurred at
rates (Swahn et al., 1988; Ghosh et al., 1997). Thus, mifepris-
a diameter of 25 mm in one woman but remained unruptured
tone blocks or delays ovulation in a dose-dependent fashion. At
in the other woman. When follicular growth and the luteal phase
doses of 1 – 10 mg, ovulation is delayed but not necessarily abol-
hormonal levels were further assessed, ultrasound showed
ished (Spitz et al., 1993; Marions et al., 2002). At higher doses,
various effects on follicular development (Marions et al., 2004).
200 – 600 mg, a new follicle is often recruited (Liu et al., 1987;
The mean diameter of the leading follicle at treatment on day
Shoupe et al., 1987), so that a single 600 mg dose is more likely
LH-2 was 18.1 mm. Among seven women, follicular develop-
to cause a 1 week delay in menses (36%) than 10 mg (18%)
ment was arrested in three of them. In three women follicular
development was delayed for 2 – 3 days and in one woman the
Administration of 5 mg mifepristone when follicular diameter
growing follicle remained unruptured until the end of the cycle.
is 6 – 11 mm, i.e. before selection of the dominant follicle, has no
No signs of follicle rupture were observed by ultrasound. Luteal
effect on follicular development (Croxatto et al., 1995). A single
phase urinary pregnanediol levels increased following treatment,
dose of 5 mg administered when the leading follicle had reached
but the increase was delayed and reduced compared to the con-
a diameter of 12 – 14 mm retarded its growth for 12 – 48 h after
trol cycle. Cycle length was slightly prolonged. There was a
treatment (Croxatto et al., 1995). Similar results were seen after
difference between the effect of treatment on estradiol- and preg-
daily treatment with 5 mg for 3 days at the same follicular stage.
anediol-glucuronide levels in these two studies (Marions et al.,
These observations indicate that mifepristone interrupts follicular
2002 and 2004). However, the reason for the difference is prob-
growth after selection of the dominant follicle. This effect
may be related to an increase in progesterone receptors (PR)in the theca and granulosa cells of the dominant follicle as it
approaches maturation (. 12 mm) (Iwai et al., 1990). Higher
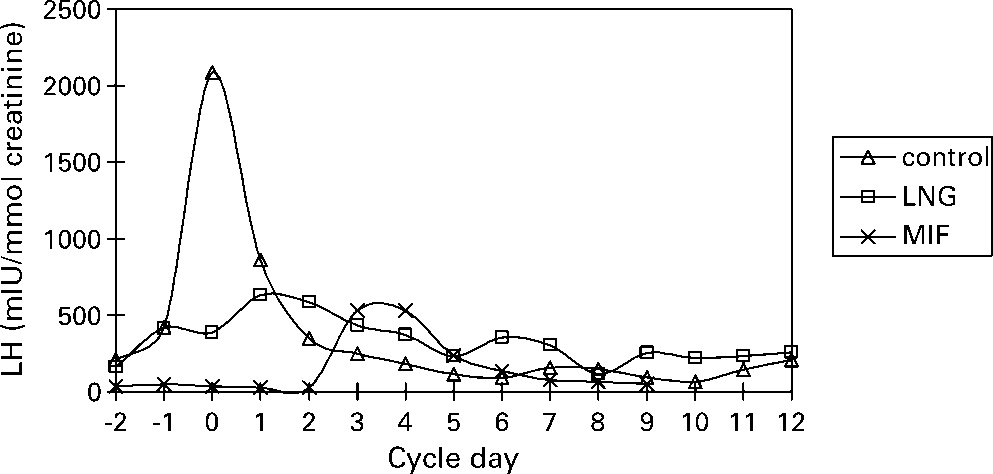
Treatment with 0.75 mg levonorgestrel twice, 12 h apart, on
doses (3 mg/kg) resulted in collapse of the dominant follicle and
approximately day LH-2 inhibited the LH peak in all women
delayed ovulation until a new follicle had been recruited
studied (Figure 1) (Marions et al., 2002, 2004). Further assess-
(Liu et al., 1987). This effect may be related to the decrease in
ment revealed that luteal phase pregnanediol- and estrone-
FSH and LH, which is induced by higher doses of mifepristone
glucuronide levels slightly but significantly differed from
(Liu et al., 1987; Permezel et al., 1989). At the pituitary level,
controls (Marions et al., 2004). Urinary glucuronide levels
mifepristone does not block the ‘rise’ in progesterone, it
were decreased compared to controls but similar to the levels
blocks the ability of progesterone to act on PR in the pituitary to
observed following mifepristone. Cycle length was slightly
facilitate the LH surge (Batista et al., 1992, 1994). In women
shorter compared to control cycles. Ultrasound revealed that
with hypothalamic amenorrhoea, mifepristone delays the mid-
follicular development was either arrested (n ¼ 3) or that the
cycle gonadotrophin surge and ovulation, despite the exogenous
treatment had resulted in a persistent unruptured follicle (n ¼ 4).
administration of GnRH (Batista et al., 1994).
In a similar study, 12 women received 0.75 mg twice with
When a single dose of 10 mg mifepristone was given to six
12 h interval pre-ovulatory (Hapangama et al., 2001b). When the
women at a follicular diameter of . 15 mm, or , 2 days prior to
treatment was given on day LH-2 or-3, the LH peak was inhib-
the LH surge, the LH surge was delayed or inhibited in all sub-
ited. In contrast, the treatment given on day LH-1 or on the day
jects (Figure 1) (Marions et al., 2002). However, no changes in
of the LH peak did not inhibit ovulation. Luteal phase LH levels
pregnanediol- or estrone-glucuronide levels in the luteal phase
were decreased, as well as the cycle length. The cycle was moni-
could be seen compared to controls. Unfortunately, repeated
tored by daily urinary samples used for the determination of LH.
ultrasound examinations during the whole cycle were only per-
No ultrasound measurements were performed. Similar results
formed in two of the six subjects. In both subjects follicles
were obtained in the rat where treatment with levonorgestrelduring the luteal phase was shown to block ovulation, totally orpartially (Mu¨ller et al., 2003). The closer to ovulation the treat-ment was given the less was the effect. Furthermore, treatmentwith levonorgestrel in the rat and monkey does not affect fertili-zation or implantation (Mu¨ller et al., 2003).
Mifepristone and levonorgestrel thus seem to affect follicular
development after selection of the dominant follicle but beforethe rise in LH has begun. The effect on follicular developmentand ovulation varies between the delayed follicular development,and arrested or persistent unruptured follicles. The LH peak iseither blocked or delayed and blunted.
Figure 1. Effect of levonorgestrel (LNG) (0.75 mg twice) or mifepristone
(MIF) (10 mg single dose) on urinary LH. The concentrations are expressedas ratios to creatinine. LNG or MIF were administered in different cycles to
There are no data on the direct exposure of human embryos
seven women on day 2 2, which was defined as the day on which the follicle
to mifepristone or levonorgestrel. Exposure of mifepristone to
size corresponded to that seen 2 days before the LH peak in the controlcycle.
monkey embryos did not affect embryo development or their
K.Gemzell-Danielsson and L.Marions et al.
ability to implant (Wolf et al., 1989). An adverse effect of levo-norgestrel seems unlikely since gestagens are commonly admi-nistered to facilitate implantation following assisted reproductionsuch as IVF.
To investigate if mifepristone interferes with gonadotrophin-
induced oocyte maturation and fertilization, clomiphene wasgiven for 5 days for stimulation of follicular growth to 40 volun-teers (Messinis and Templeton, 1988). On day 16,20 womenreceived 100 mg mifepristone 1 h before induction of ovulationwith injection of 5000 IU of hCG. Laparoscopy (for tubal sterili-zation) was performed 34 h after hCG and all follicles with adiameter of . 15 mm were aspirated, and collected oocytes sub-mitted to IVF. The 20 women not receiving mifepristone servedas a control group. The number of retrieved oocytes, the rate offertilization, and the cleavage rate did not differ between themifepristone group and the controls.
When treatment with mifepristone takes place just prior toovulation, follicular rupture may occur. Mifepristone in highdoses, due to its long half-life, may also affect tubal and uter-ine functions. The tubal microenvironment is probably of greatimportance to ensure normal embryo development, and stage-specific expression of receptors for various growth factorshas been found on human embryos (Smotrich et al., 1996). Too rapid or too slow tubal transport could also be expectedto cause desynchronization between the embryo and the tube,and/or the blastocyst and the endometrium. Progesteroneregulates tubal transport in vitro, as confirmed in a study by
Figure 2. Immunostaining of (a) progesterone receptors (PR) and (b) estro-
Mahmood et al. (1998). Cilia from the human Fallopian tube
gen receptors (ER) in the human Fallopian tube on day LH þ 4 to þ 6 in
beat significantly slower after treatment with high doses of
controls and following treatment on day LH þ 2. Treatment with 200 mg
progesterone, an effect that could be reversed by mifepristone.
of mifepristone significantly increased expression of PR and ER. Treatment
Furthermore, animal studies have previously shown accelerated
with levonorgestrel (0.75 mg twice) had no effect. Mean and SD of
tubal egg transport after mifepristone treatment (Psychoyos and
A spatially dependent expression of progesterone receptors
has been shown in the human Fallopian tube (Christow et al.,
a slight inhibition of endometrial development on cycle days
2002). Higher levels of receptors are being expressed in the
LH þ 6 to þ 8. The expression of the b3 integrin subunit in
isthmic region than the ampullar region of the tube on days
the glandular epithelial cells was decreased in two subjects. The
LH þ 4 to þ 6. Following the administration of 200 mg of mife-
expression of COX-1 and -2, integrin a4, progesterone receptors
pristone on day LH þ 2, progesterone receptor concentration
and DBA-lectin binding as well as pinopode development was
increased in epithelial and stromal cells. There was also an effect
the same as observed in control cycles (Figure 3).
on estrogen receptor levels, although less pronounced and
In contrast, a higher dose of mifepristone given in the peri-
restricted to the epithelial cells (Figure 2).
ovulatory phase, even when too late to inhibit ovulation, affected
The treatment with 0.75 mg of levonorgestrel twice with a
endometrial development during the luteal phase. When a single
12 h interval did not affect the distribution of progesterone or
dose of 200 mg of mifepristone was given at the time when LH
just started to increase, ovulation occurred in five women andwas delayed in two women. Endometrial development duringthe mid-luteal phase was assessed in six women (Brown et al.,
2003). Asynchrony between the endocrine patterns, and betweenthe endometrial appearances, was described. There was a failure
of normal secretory change, with absent or minimal vacuolation
A single dose of 10 mg of mifepristone administered , 2 days
prior to ovulation inhibited or delayed the LH surge in all sub-
Treatment with levonorgestrel 0.75 mg twice, 12 h apart, on
jects (Marions et al., 2002). The luteal phase levels of estrone-
day LH-2 had no effect on the endometrial development
and pregnanediol-glucuronide were slightly decreased compared
during the mid-luteal phase at the expected time of endometrial
to control levels (Marions et al., 2004). Two subjects showed
receptivity and implantation (Marions et al., 2002).
Emergency contraception: mechanisms of action
dose of 0.5 mg was administered daily for three cycles, all sub-jects ovulated and similar changes were observed in the endome-trium although to a lesser degree than with the once-weeklyregimen (Gemzell Danielsson et al., 1997b). Both regimenshave been shown to significantly impair fertility although notsufficient for contraceptive use (Marions et al., 1998a, 1999).
When a single dose of 10 mg mifepristone was administered
on day LH þ 2, the observed effect on the endometrium wasless pronounced than after treatment with 200 mg or repeatedlow doses (Marions et al., 2002). Following 10 mg, the endome-trium was slightly out of phase, while no obvious effect wasseen on LIF and integrin expression or pinopod development. DBA lectin binding, reflecting endometrial secretory activity,was reduced in four of six subjects and down-regulation ofprogesterone receptors was inhibited in five of six subjects. A large number of factors have been suggested as markers ofendometrial receptivity, but progesterone receptor concentrationcould be expected to be highly associated with successfulimplantation since many of the relevant local factors such ascytokines are progesterone-regulated. However, different regulat-ory mechanisms or pathways may be involved. In Bonnet mon-
Figure 3. Pinopod formation in varying developing stages. Endometrial
keys treatment with onapristone in doses ranging from 2.5 to
sample obtained on LH þ 6 following mifepristone 10 mg on LH-2. Electron
10 mg every third day did not inhibit ovulation and had only a
microscopy. Original magnification £ 200.
minor effect on endometrial morphology, but it was shown to behighly effective in inhibiting endometrial receptivity and implan-
tation (Puri et al., 2000). The lowest dose, 2.5 mg every third
Treatment with a single dose of 200 mg mifepristone on day
day, did not affect progesterone receptor expression, but reduced
LH þ 2 has been shown to be an effective contraceptive
LIF and integrins. However, higher doses affected all markers
method (Gemzell Danielsson et al., 1994; Hapangama et al.,
2001a) (Table II). Early luteal phase treatment causes changes in
Levonorgestrel (0.75 mg £ 2) administered on day LH þ 2
endometrial glandular apoptosis, secretory activity, expression of
did not affect endometrial morphology or any studied markers of
steroid receptors, especially progesterone receptors but also
receptivity (Durand et al., 2001; Marions et al., 2002).
androgen and estrogen receptors, integrins and leukaemia inhibi-tory factor (LIF) at the expected time of implantation (GemzellDanielsson et al., 1997a, 1998; Marions et al., 1998a; Critchleyet al., 1999; Slayden et al., 2001). Mifepristone also affects
calcitonin expression (Kumar et al., 1998) as well as prostaglan-
Down-regulation of progesterone receptor B (PRB) mRNA
din dehydrogenase (Cameron et al., 1997). Furthermore, changes
occurs in the mid-luteal phase corpus luteum (Ottander et al.,
occur in the composition and amount of uterine fluid (Gemzell
2000). PRB mRNA levels were found to be 100–1000-fold
lower than progesterone receptor A plus B (PRA/B) mRNA levels
rhythm remains undisturbed and serum levels of estradiol and
and were 46% lower in mid-luteal phase, compared to early and
progesterone remain essentially unchanged (Swahn et al., 1990).
late luteal phase. Freshly obtained mid-luteal corpus luteum cells
Treatment with 5 mg mifepristone once a week with start on
were cultured in vitro and media analysed for progesterone con-
cycle day 2 did not inhibit ovulation but retarded or desynchro-
centrations after treatment with hCG and mifepristone. Mifepris-
nized endometrial development (Gemzell Danielsson et al.,
tone did not alter progesterone synthesis per se, but when
1996). An increase in progesterone receptor levels was observed
it was added in conjunction with hCG, a dose-dependent
as well as an impaired secretory activity. When an even lower
inhibitory response was seen, with a maximal 47% reduction in
Table II. Effects of antigestagens in various doses on potential markers of endometrial receptivity and contraceptive efficacy
K.Gemzell-Danielsson and L.Marions et al.
progesterone output at a 10 mmol/l mifepristone addition. The
advantage with the lower dose is that the effect on the menstrual
effect of mifepristone on early corpus luteum was not studied.
cycle (WHO, 1999) and delay of the next menstruation is dose-
Administration of $ 25 mg of mifepristone during the mid- to
dependent and less pronounced with this dose. A delay in the
late luteal phase results in shedding of the endometrium and
next menses may add to the worry about an unintended preg-
vaginal bleeding within a few days of the treatment. The bleed-
nancy. Furthermore, with the higher doses there is an increased
ing is probably induced by an effect of mifepristone on endo-
risk of delayed ovulation which exposes the women to the risk
metrial prostaglandin metabolism (Hapangama et al., 2003). If
of pregnancy should she have further acts of unprotected
premature menstruation is not accompanied by luteolysis in the
mid-luteal phase (, 50% of cases), the endometrial and ovarian
Treatment with 200 mg mifepristone on day LH þ 2 changes
cycles are desynchronized and a second bleeding episode occurs
the steroid receptor expression in the Fallopian tube, inhibits
at the time of the expected menstruation (Schaison et al., 1985;
endometrial development, and effectively prevents implantation
Garzo et al., 1988; Swahn et al., 1988). The manner in which
(Gemzell Danielsson et al., 1993; Hapangama et al., 2001). Low
antiprogestin induces luteolysis in certain situations is not pre-
dose mifepristone (10 mg) administered after ovulation seems to
cisely known, but could be indirect via withdrawal of LH sup-
have some effect on endometrial development and progesterone
port (Mais et al., 1986) as shown by a reduction in amplitude
receptor expression although not as pronounced as the effect of
and frequency of LH pulses and blunting of the pituitary LH
the higher dose (i.e. 200 mg). The effect seems to be variable
response to GnRH (Schaison et al., 1985; Garzo et al., 1988). It
possibly reflecting individual sensitivity, or the 10 mg dose
may also depend on the age of the corpus luteum (Swahn et al.,
might be at the threshold of affecting the endometrium. Further-
1988). Once-a-week treatment with 5 mg mifepristone did not
more, treatment prior to ovulation did not significantly affect
inhibit ovulation and did not influence the length of the luteal
endometrial development in contrast to a single dose of 200 mg
phase (Gemzell Danielsson et al., 1996).
(Marions et al., 2002; Brown et al., 2003).
The possibility of using the antiprogestin mifepristone for late
Daily low dose treatment with 0.5 mg mifepristone, had an
luteal phase treatment or menstrual regulation has been evalu-
effect on endometrial morphology similar to that of a 10 mg
ated in a number of studies (Ulmann, 1987; van Santen and
single dose, without influencing ovulation, and significantly
Haspels, 1987; Dubois et al., 1988; La¨hteenma¨ki et al., 1988).
reduced fertility (Marions et al., 1999). However, 0.5 mg per day
The overall failure rate per treatment cycle is , 5% and per
had a different effect on some proposed markers of endometrial
pregnant cycle 17% (for review, see Swahn et al, 1996; Crox-
receptivity. Low daily doses did not affect progesterone
atto, 2003). Late luteal phase treatment with 200 mg mifepris-
receptor expression, but significantly reduced LIF and integrin
tone on the day prior to the expected menstruation, followed
by a prostaglandin analogue 48 h later, was also shown to be
progesterone receptor expression but had no effect on LIF
ineffective as a contraceptive method (Swahn et al., 1999).
In summary, available data from the studies in humans indi-
cate that the contraceptive effect of 10 mg mifepristone used as
a single dose for emergency contraception is mainly due to
Treatments with low dose mifepristone or levonorgestrel have
impaired ovarian function, either by blocking the LH surge or
emerged as effective, convenient and safe methods for emer-
by postponing the surge rather than inhibiting the implantation.
gency contraception. The contraceptive effect of 1.5 mg levonor-
In contrast, higher doses affect both ovulation and implantation.
gestrel or 10 mg of mifepristone involves blockade or delay of
It may seem surprising that doses ranging from 10 mg to 600 mg
ovulation. The ‘window of effect’ for levonorgestrel seems to be
were reported to be equally effective. However, when the effi-
rather narrow. It begins after selection of the dominant follicle,
cacy of 600 mg of mifepristone is further analysed and women
but before LH begins to rise. Levonorgestrel does not affect
who conceived after treatment are excluded, the data actually
endometrial development or steroid receptor expression in the
show that 600 mg is more effective than the lower doses (WHO,
Fallopian tube. Animal studies confirm that levonorgestrel acts
1999). Thus, the mode of action of mifepristone, as well as effi-
to block or delay ovulation but does not affect fertilization or
cacy, seems to be both dose and time dependent.
implantation (Mu¨ller et al., 2003). If the effect of EC is mainly
In conclusion, emergency contraception with 10 mg of mif-
to block the LH surge or to interfere with other processes
pristone as a single dose or 1.5 mg of levonorgestrel acts mainly
involved in ovulation, is not clear and needs to be further
to inhibit or delay ovulation but does not prevent fertilization
or implantation. Increased knowledge of the mechanism of
The efficacy of levonorgestrel, 0.75 mg twice 12 h apart or a
action could hopefully increase the acceptability and thus avail-
single dose of 1.5 mg, was shown to be equal to that of a single
ability of these methods, to offer women a chance to prevent an
dose of 10 mg of mifepristone (von Hertzen et al., 2002). Further
unwanted pregnancy and thus reduce the numbers of induced
analysis of the data shows that mifepristone seems to be slightly
more effective in preventing pregnancy after one act of unpro-tected intercourse, while it is also more likely to postpone ovu-lation. Thus women with further acts of unprotected intercourse
are put at higher risk of pregnancy.
We are grateful to Associate Professor Sten Cekan for help in the
A single dose of 10 mg mifepristone within 120 h of an unpro-
editing and preparation of this article. The studies from the
tected intercourse has been shown to be as effective as doses of
Karolinska Hospital referred to in the article were supported by
50 or 600 mg but with significantly less side-effects. A great
UNDP/UNFPA/WHO/World Bank Special Programme of Research
Emergency contraception: mechanisms of action
Development and Research Training in Human Reproduction,
on ovarian function and endometrial development. Hum Reprod
World Health Organization, Geneva, Switzerland, and the Swedish
Medical Research Council (nos. 05696, 05170 and 0855), The Knut
Glasier A, Thong KJ, Dewar M, Mackie M and Baird D (1992) Mifepristone
and Alice Wallenberg Foundation, the Karolinska Institute Research
(RU 486) compared with high-dose estrogen and progesterone for emer-
Funds and Professor Sune Bergstro¨m, Karolinska Institute.
gency postcoital contraception. New Eng J Med 327,1041 – 1044.
Ghosh D, Kumar PG and Sengupta J (1997) Early luteal phase administration
of mifepristone inhibits preimplantation embryo development and viabi-lity in the rhesus monkey. Hum Reprod 12,575– 582.
Hapangama DK, Brown A, Glasier AF and Baird DT (2001a) Feasibility of
Bahamondes L, Nascimento JAA, Munuce MJ, Fazano F and Faundes
administering mifepristone as a once a month contraceptive pill. Hum
A (2003) The in vitro effect of levonorgestrel on the acrosome reaction
of human spermatozoa from fertile men. Contraception 68,55 – 59.
Hapangama DK, Glasier AF and Baird DT (2001b) The effects of peri-ovula-
Batista MC, Cartledge TP, Zellmer AW, Nieman LK, Merriam GR and
tory administration of levonorgestrel on the menstrual cycle. Contracep-
Loriaux DL (1992) Evidence for a critical role of progesterone in the
regulation of the midcycle gonadotropin surge and ovulation. J Clin
Hapangama DK, Critchley HOD, Henderson TA and Baird DT (2003)
Mifepristone-induced vaginal bleeding is associated with increased
Batista MC, Cartledge TP, Zellmer AW, Nieman LK, Loriaux DL and
immunostaining for cyclooxygenase-2 and decrease in prostaglandin
Merriam GR (1994) The antiprogestin RU 486 delays the midcycle
dehydrogenase in luteal phase endometrium. J Clin Endocrinol Metab
gonadotropin surge and ovulation in gonadotropin-releasing hormone-
induced cycles. Fertil Steril 62,28 – 34.
Iwai T, Nanbu Y, Iwai M, Taii S, Fujii S and Mori T (1990) Immunohisto-
Blackmore PF, Neulen J, Lattanzio F and Beebe SJ (1991) Cell surface bind-
chemical localisation of oestrogen receptors and progesterone receptors
ing sites for progesterone mediate calcium uptake in human sperm.
in the human ovary throughout the menstrual cycle. Virchows Arch A
Pathol Anat Histopathol 417,369– 375.
Brown A, Williams A, Cameron S, Morrow S and Baird DT (2003) A single
Kesseru¨ E, Garmendia F, Westphal N and Parada J (1974) The hormonal
dose of mifepristone (200 mg) in the immediate preovulatory phase
and peripheral effects of dl-norgestrel in postcoital contraception.
offers a contraceptive potential without cycle disruption. Contraception
Kumar S, Zhu LJ, Polihronis M, Cameron ST, Baird DT, Schatz F, Dua A,
Cameron ST, Critchley HO, Buckley CH, Kelly RW and Baird DT (1997)
Ying YK, Bagchi MK and Bagchi IC (1998) Progesterone induces
Effect of two antiprogestins (mifepristone and onapristone) on endo-
calcitonin gene expression in human endometrium within the putative
metrial factors of potential importance for implantation. Fertil Steril
window of implantation. J Clin Endocrinol Metab 83,4443– 4450.
Kunz G, Beil D, Deininger H, Wildt L and Leyendecker G (1996) The
Christow A, Sun X and Gemzell-Danielsson K (2002) Effect of mifepristone
dynamics of rapid sperm transport through the female genital tract: evi-
and levonorgestrel on expression of steroid receptors in the human
dence from vaginal sonography of uterine peristalsis and hysterosalpin-
Fallopian tube. Mol Hum Reprod 8,333 – 340.
goscintigraphy. Hum Reprod 11,627– 632.
Consensus statement of emergency contraception (1995) Consortium for
Lippes J, Tatum HJ, Maulik D and Sielezny M (1979) Postcoital copper
Emergency Contraception. Contraception 52,211– 213.
Critchley HO, Tong S, Cameron ST, Drudy TA, Kelly RW and Baird DT
Liu JH, Garzo G, Morris S, Stuenkel C, Ulmann A and Yen SS (1987) Dis-
(1999) Regulation of bcl-2 gene family members in human endometrium
ruption of follicular maturation and delay of ovulation after adminis-
by antiprogestin administration in vivo. J Reprod Fertil 115,389– 395.
tration of the antiprogesterone RU486. J Clin Endocrinol Metab 65,
Croxatto HB (2003) Mifepristone for luteal phase contraception. Contracep-
La¨hteenma¨ki P, Rapeli T, Kaariainen Alfthan H and Ylikorkala O (1988)
Croxatto HB, Salvatierra AM, Fuentealba B and Leiva L (1995) Follicle
Late postcoital treatment against pregnancy with antiprogesterone RU
stimulating hormone-granulosa cell axis involvement in the antifolliculo-
trophic effect of low dose mifepristone (RU486). Hum Reprod 10,
Mais V, Kazer RR, Cetel NS, Rivier J, Vale W and Yen SSC (1986) The
dependency of folliculogenesis and corpus luteum function on pulsatile
Dubois C, Ulmann A and Baulieu EE (1988) Contragestion with late luteal
gonadotropin secretion in cycling women using a gonadotropin-releasing
administration of RU 486 (Mifepristone). Fertil Steril 50,593 – 596.
hormone antagonist as a probe. J Clin Endocrinol Metab 62,1250– 1255.
Durand M, del Carmen Cravioto M, Raymond EG, Duran-Sanchez O, De la
Mahmood T, Saridogan E, Smutna S, Habib AM and Djahanbakhch O
Luz Cruz-Hinojosa M, Castell-Rodriguez A, Schiavon R and Larrea F
(1998) The effect of ovarian steroids on epithelial ciliary beat frequency
(2001) The mechanism of action of short term levonorgestrel adminis-
in the human Fallopian tube. Hum Reprod 13,2991 – 2994.
tration in emergency contraception. Contraception 64,227– 234.
Marions L, Gemzell Danielsson K, Swahn ML and Bygdeman M (1998a)
Garzo VG, Liu J, Ulmann A, Baulieu E and Yen SSC (1988) Effects of an
The effect of antiprogestin on integrin expression in human endome-
antiprogesterone (RU 486) on the hypothalamic-hypophyseal-ovarian-
trium: an immunohistochemical study. Hum Reprod 4,491 – 495.
endometrial axis during the luteal phase of the menstrual cycle. J Clin
Marions L, Gemzell Danielsson K, Swahn ML and Bygdeman M (1998b)
Contraceptive efficacy of low doses of mifepristone. Fertil Steril 70,
Gemzell Danielsson K, Swahn ML, Svalander P and Bygdeman M (1993)
Early luteal phase treatment with RU486 for fertility regulation. Hum
Marions L, Viski S, Danielsson KG, Resch BA, Swahn ML, Bygdeman M
and Kovacs L (1999) Contraceptive efficacy of daily administration of
Gemzell Danielsson K and Hamberg M (1994) The effect of antiprogestin
0.5 mg mifepristone. Hum Reprod 14,2788 – 2790.
(RU 486) and prostaglandin biosynthesis inhibitor (naproxen) on uterine
Marions L, Hultenby K, Lindell I, Sun X, Stabi B and Gemzell Danielsson K
fluid prostaglandin F2a concentration. Hum Reprod 9,1626 – 1630.
(2002) Emergency contraception with mifepristone and levonorgestrel:
Gemzell Danielsson K, Svalander P, Swahn ML, Johannisson E and
mechanism of action. Obstet Gynecol 100,65 – 71.
Bygdeman M (1994) Effects of a single-postovulatory dose of RU486
Marions L, Cekan C, Bygdeman M and Gemzell Danielsson K (2004) Pre-
on endometrial maturation in the implantation phase. Hum Reprod
ovulatory treatment with mifepristone and levonorgestrel impairs luteal
function. Contraception 69,373– 377.
Gemzell Danielsson K, Westlund P, Swahn ML, Bygdeman M and Seppala
Messinis IE and Templeton A (1988) The effect of the antiprogestin mife-
M (1996) Effect of low weekly doses of mifepristone on ovarian func-
pristone (RU486) on maturation and in-vitro fertilization of human
tion and endometrial development. Hum Reprod 11,256– 264.
oocytes. Br J Obstet Gynaecol 95,592 – 595.
Gemzell Danielsson K, Swahn ML and Bygdeman M (1997a) The effect of
Morris JMcL and van Wagenen G (1966) Compounds interfering with ovum
various doses of mifepristone on endometrial leukaemia inhibitory factor
implantation and development. III. The role of estrogens. Am J Obstet
expression in the midluteal phase—an immunohistochemical study.
Mu¨ller AL, Llados CM and Croxatto HB (2003) Postcoital treatment with
Gemzell Danielsson K, Swahn ML, Westlund P, Johannisson E, Seppa¨la¨ M
levonorgestrel does not disrupt postfertilization events in the rat. Contra-
and Bygdeman M (1997b) Effect of low daily doses of mifepristone
K.Gemzell-Danielsson and L.Marions et al.
Ottander U, Hosokawa K, Liu K, Bergh A, Ny T and Olofsson J (2000) A
Swahn ML, Bygdeman M, Chen J-K, Gemzell Danielsson K, Song S, Yang
putative stimulatory role for progesterone acting via progesterone recep-
Q-Y, Yang P-J, Chen J-K, Qian M-L and Chang W-F (1999) Once-a-
tors in the steroidogenic cells of the human corpus luteum. Biol Reprod
month treatment with a combination of mifepristone and the prostaglan-
din analogue misoprostol. Hum Reprod 14,485 – 488.
Permezel JM, Lenton EA, Roberts I and Cooke ID (1989) Acute effects of
Ulmann A (1987) Uses of RU 486 for contragestion: an update. Contracep-
progesterone and the antiprogestin RU 486 on gonadotropin secretion in
the follicular phase of the menstrual cycle. J Clin Endocrinol Metab
van Santen MR and Haspels AA (1987) Interception III: postcoital luteal
contragestion by an antiprogestin (mifepristone RU 486) in 62 women.
Psychoyos A and Prapas I (1987) Inhibition of egg development and implan-
tation in rats after post-coital administration of the progesterone antag-
von Hertzen H, Piaggio G, Ding J, Chen J, Song S, Bartfai G, Ng E, Gem-
onist RU 486. J Reprod Fertil 80,487 – 491.
zell-Danielsson K, Oyunbileg A, Wu S, Cheng W et al. (2002) Low
Puri CP, Katkam RR, Sachdeva G, Patil V, Manjramkar DD and Kholkute
dose mifepristone and two regimens of levonorgestrel for emergency
SD (2000) Endometrial contraception: modulation of molecular determi-
contraception: a WHO multicentre randomised trial. Lancet 360,
nants of uterine receptivity. Steroids 65,783– 794.
Schaison G, George M, Lestrat N, Reinberg A and Baulieu EE (1985)
Webb AM, Russell J and Elstein M (1992) Comparison of Yuzpe regimen,
Effects of the antiprogesterone steroid RU 486 during midluteal phase in
danazol and mifepristone (RU486) in oral postcoital contraception. Br
normal women. J Clin Endocrinol Metab 61,484– 489.
Shoupe D, Mishell DR, Jr, Page MA, Madkour H, Spitz IM and Lobo RA
Wilcox AJ, Weinberg CR and Baird DD (1995) Timing of sexual intercourse
(1987) Effects of the antiprogesterone RU 486 in normal women. II.
in relation to ovulation. N Engl J Med 133,1517 – 1521.
Administration in the late follicular phase. Am J Obstet Gynecol
Wolf JP, Danforth DR, Ulmann A, Baulieu EE and Hodgen GD (1989) Con-
traceptive potential of RU486 by ovulation inhibition II. Supression of
Serres C, Yang J and Jouannet P (1994) RU486 and calcium fluxes in human
pituitary gonadotropin secretion in vitro. Contraception 40,185 – 193.
spermatozoa. Biochem Biophys Res Commun 15,1009– 1015.
World Health Organization Task Force on Post-ovulatory Methods for Ferti-
Slayden OD, Nayak NR, Burton KA, Chwalisz K, Cameron ST, Critchley
lity Regulation (1998) Randomized controlled trial of levonorgestrel ver-
HO, Baird DT and Brenner RM (2001) Progesterone antagonists
sus the Yuzpe regimen of combined oral contraceptives for emergency
increase androgen receptor expression in the rhesus macaque and human
contraception. Lancet 352,428 – 433.
endometrium. J Clin Endocrinol Metab 86,2668 – 2679.
World Health Organization Task Force on Post-ovulatory Methods for Ferti-
Smotrich DB, Stillman RJ, Widra EA, Gindoff PR, Kaplan P, Graubert M
lity Regulation (1999) Comparison of three single doses of mifepristone
and Johnson KE (1996) Immunocytochemical localization of growth
as emergency contraception: a randomised trial. Lancet 353,697 – 702.
factors and their receptors in the human pre-embryos and Fallopian
Xiao BL, Von Hertzen H, Zhao H and Piaggio G (2002) A randomized
double-blind comparison of two single doses of mifepristone for emer-
Spitz IM, Croxatto HB, Salvatierra AM and Heikinheimo O (1993) Response
gency contraception. Hum Reprod 17,3084– 3089.
to intermittent RU486 in women. Fertil Steril 59,971 – 975.
Yang J, Serres C, Philibert D, Robel P, Baulieu EE and Jouannet P (1994)
Swahn ML, Johannisson E, Daniore V, de la Torre B and Bygdeman M
Progesterone and RU486: opposing effects on human sperm. Proc Natl
(1988) The effect of RU 486 administered during the proliferative and
secretory phase of the cycle on the bleeding pattern, hormonal par-
Yeung WSB, Chiu PCN, Wang CHYQ, Yao YQ and Ho PC (2002) The
ameters and the endometrium. Hum Reprod 3,915 – 921.
effects of levonorgestrel on various sperm functions. Contraception
Swahn ML, Bygdeman M, Xing S, Cekan S, Masironi B and Johannisson E
(1990) The effect of RU 486 administered during the early luteal phase
Yuzpe AA and Lance WJ (1977) Ethinylestradiol and dl-norgestrel as a
on bleeding pattern, hormonal parameters and endometrium. Hum
potential contraceptive. Fertile Steril 28,932– 936.
Swahn ML, Gemzell Danielsson K and Bygdeman M (1996) Contraception
with antiprogesterone. In Glasier A (ed) Ballie`re’s Clinical Obstetrics
Submitted on December 12, 2003; resubmitted on February 20, 2004;
and Gynecology: Contraception. Ballie`re Tindall, Oxford, pp 43 – 53.
Gaucher Disease Newsletter Summer, 2000 A Publication of the National Gaucher Foundation Founded by Rubin Bakin Dear Doctor Q: I am a 35 year old woman who was diagnosed 10 years ago with Gaucher Disease. I have received ERT for 5 years and I feel great. I am going to Israel for 3 months. Can I stop my infusions while I am in Israel? A: There are various theories abou
YOUR REQUEST UNDER FREEDOM OF INFORMATION Q. I would like to request a copy of the latest medicines formularies for Cornwall and the Isles of Scilly, as well as any prescribing guidelines for asthma, COPD or diabetes. Answer: Follow the link to the PCT website for the joint formulary: Attached are the following: Respiratory resource pack Formulary factsheet, Insulin for Type 2 Diabetes
 Emergency contraception: mechanisms of action
the following luteal phase seems to be normal with normal endo-
continued to grow, exceeding the size seen in the control cycle,
metrial development and function, as judged by implantation
and the LH surge was delayed. Follicular rupture occurred at
rates (Swahn et al., 1988; Ghosh et al., 1997). Thus, mifepris-
a diameter of 25 mm in one woman but remained unruptured
tone blocks or delays ovulation in a dose-dependent fashion. At
in the other woman. When follicular growth and the luteal phase
doses of 1 – 10 mg, ovulation is delayed but not necessarily abol-
hormonal levels were further assessed, ultrasound showed
ished (Spitz et al., 1993; Marions et al., 2002). At higher doses,
various effects on follicular development (Marions et al., 2004).
Emergency contraception: mechanisms of action
the following luteal phase seems to be normal with normal endo-
continued to grow, exceeding the size seen in the control cycle,
metrial development and function, as judged by implantation
and the LH surge was delayed. Follicular rupture occurred at
rates (Swahn et al., 1988; Ghosh et al., 1997). Thus, mifepris-
a diameter of 25 mm in one woman but remained unruptured
tone blocks or delays ovulation in a dose-dependent fashion. At
in the other woman. When follicular growth and the luteal phase
doses of 1 – 10 mg, ovulation is delayed but not necessarily abol-
hormonal levels were further assessed, ultrasound showed
ished (Spitz et al., 1993; Marions et al., 2002). At higher doses,
various effects on follicular development (Marions et al., 2004).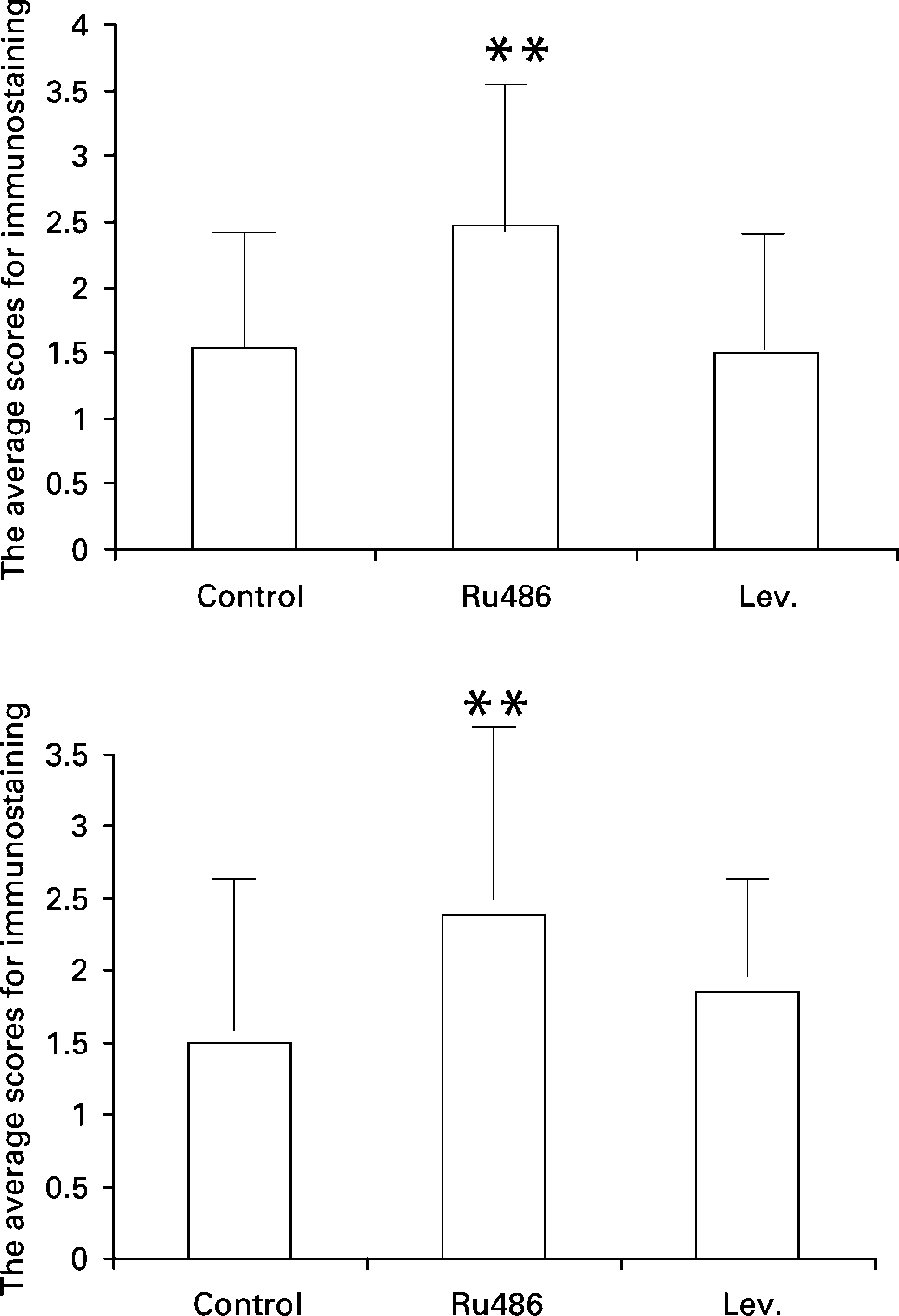 K.Gemzell-Danielsson and L.Marions et al.
K.Gemzell-Danielsson and L.Marions et al.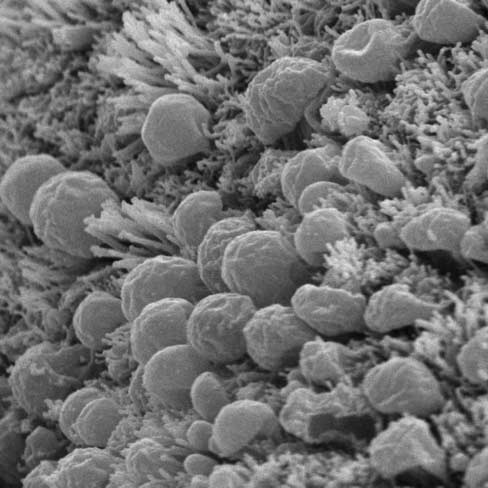 Emergency contraception: mechanisms of action
dose of 0.5 mg was administered daily for three cycles, all sub-jects ovulated and similar changes were observed in the endome-trium although to a lesser degree than with the once-weeklyregimen (Gemzell Danielsson et al., 1997b). Both regimenshave been shown to significantly impair fertility although notsufficient for contraceptive use (Marions et al., 1998a, 1999).
Emergency contraception: mechanisms of action
dose of 0.5 mg was administered daily for three cycles, all sub-jects ovulated and similar changes were observed in the endome-trium although to a lesser degree than with the once-weeklyregimen (Gemzell Danielsson et al., 1997b). Both regimenshave been shown to significantly impair fertility although notsufficient for contraceptive use (Marions et al., 1998a, 1999).