Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Gdmedical.ch
Journal of Perinatology (2007) 27, 85–91
r 2007 Nature Publishing Group All rights reserved. 0743-8346/07 $30
ORIGINAL ARTICLEHigh flow nasal cannula versus nasal CPAP for neonatal
respiratory disease: a retrospective study
MT Shoemaker1, MR Pierce2, BA Yoder3 and RJ DiGeronimo11Wilford Hall USAF Medical Center, Lackland AFB, TX, USA; 2Pediatrix Medical Group, Santa Rosa Children’s Hospital, San Antonio,TX, USA and 3Primary Children’s Medical Center, University of Utah, Salt Lake City, UT, USA
cost. One report put the cost at 4.4 billion dollars per year in the
Objective: Our objective is to assess the frequency of usage, safety and
United States, and this only includes the time in the neonatal
clinical utility of humidified high flow nasal cannula (HHFNC) in two tertiary
intensive care unit.1 The current practice of most neonatologists
care hospitals and compare outcomes to a historical control group of premature
reflects the belief that limited exposure to invasive mechanical
infants who received nasal continuous positive airway pressure (NCPAP).
ventilation and careful use of oxygen support result in less lung
Study design: The first part of the study describes the increased HHFNC
injury and improved long-term pulmonary outcomes in premature
usage in two tertiary neonatal intensive care units. The second part
infants.2,3 Given this, there is now a concerted effort in many
compares outcomes of infants, born at less than 30 weeks gestation, who
practices to avoid the use of prolonged invasive ventilatory support
received either NCPAP or HHFNC as an early respiratory support mode.
when treating acute respiratory distress in premature infants withearly application of nasal continuous positive airway pressure
Results: HHFNC usage increased (64%) after its introduction in infants
(NCPAP) either immediately after birth or following a brief period
of all gestational ages whereas the usage of NCPAP decreased from 19 to
of intubation, mechanical ventilation and dosing with
4%. Ninety-five percent of infants born at less than 30 weeks gestation
received HHFNC at some point during their hospital stay whereas only
An alternative to the use of NCPAP as a non-invasive modality
12% received NCPAP. There were no differences in death or
to support respiratory distress in premature infants has been the
bronchopulmonary dysplasia (BPD), but ventilator-days per patient were
recent introduction of humidified high flow nasal cannula
decreased (19.4 to 9.9) following introduction of HHFNC. Comparing the
(HHFNC) devices in many units. Although its use has been widely
cohort of infants who received either NCPAP or HHFNC as an early mode
adopted, there have been only a few published abstracts describing
of respiratory support, there were no differences in deaths, ventilator-days,
its use in the neonatal population and no clinical trials using flows
BPD, blood infections or other outcomes. More infants were intubated for
>2 l/min.9–13 The effects of the introduction of HHFNC on
failing early NCPAP compared to early HHFNC (40 to 18%).
outcomes such as duration of supplemental oxygen, mechanical
Conclusions: HHFNC was well-tolerated by premature infants.
ventilation-days, bronchopulmonary dysplasia (BPD), hospital
Compared to infants managed with NCPAP, there were no apparent
length of stay (LOS) and mortality, among other measures, have
differences in adverse outcomes following the introduction of HHFNC.
not been formally assessed. Furthermore, in the absence of an
Additional research is needed to better define the utility and safety of
accepted way to monitor end airway pressure, it is unclear if
HHFNC is inadvertently generating high pressures and causing
Journal of Perinatology (2007) 27, 85–91. doi:10.1038/sj.jp.7211647
unrecognized lung damage, particularly in the smaller preterminfants.
Keywords: humidified high flow nasal cannula; nasal continuouspositive airway pressure; bronchopulmonary dysplasia
In this report we describe our recent experience with HHFNC
following its widespread acceptance into practice in two largereferral medical centers, to include frequency of use and efficacyand safety of HHFNC compared to previous outcomes with
non-invasive respiratory support consisting of NCPAP.
Respiratory failure in the neonatal period remains a difficultchallenge and is associated with high morbidity, mortality and
Correspondence: Dr M Shoemaker, Division of Neonatology, Wilford Hall USAF Medical
Center, 2200, Bergquest Dr, Lackland AFB, TX 78236, USA.
We performed a retrospective database review of infants admitted to
E-mail: michael.shoemaker@lackland.af.milReceived 6 June 2006; revised 18 October 2006; accepted 10 November 2006
two regional referral medical centers (Wilford Hall USAF Medical
Center, Lackland AFB, TX, USA and Christus Santa Rosa Children’s
Hospital, San Antonio, TX, USA) during two study periods. The
study periods were defined as August 2003 through June 2004
(Era 1) and August 2004 through June 2005 (Era 2). These timeperiods were based on the identification of June 2004 as a time
point in both centers when the use of HHFNC became readilyavailable as an alternative therapy to NCPAP for neonates withrespiratory distress. The study was divided into two parts: (1) The
first part describes the change in frequency of usage of HHFNC and
NCPAP and compares selected outcomes of premature infants born
during the two eras; and (2) the second part analyzes the outcomes
of a defined cohort of infants less than 30 weeks gestational age(GA) who received either NCPAP or HHFNC as an early mode of
respiratory support during the two eras (Figure 1).
Infants were included in the retrospective cohort (Part 2) if they
were less than 30 weeks GA and inborn or transferred to one of thestudy centers within the first 24 h of life. To meet study criteria,
infants had to be placed on one of the respiratory support modalitiesof interest (NCPAP or HHFNC) either initially following admission,
Part 2 : Retrospective Cohort (Tables 4-7)
as an escalation of support from oxyhood or low flow nasal cannula(p2 l/min (LPM), or immediately following extubation from
Figure 1 Design of the two parts of the study.
mechanical ventilation within 96 h of birth. Nasal CPAP supportwas provided by either the Arabella (Hamilton Medical, Inc.,
than 0.05 were considered statistically significant. Logistic regression
Bonaduz, Switzerland), InfantStar (Infrasonics, San Diego, CA,
was used to analyze potential confounding variables. This study was
USA), or Infant Flow Driver (Viasys Healthcare Inc., Warwick,
approved by the Institutional Review Boards of both institutions.
England) utilizing pressures ranging from 3 to 8 cm H2O. Astraditionally the use of standard flow nasal cannulas in most
neonatal units is limited to flow rates of 2 LPM or below, we defined
high flow for rates greater than 2 LPM (range, 2.5 to 8 LPM).
Table 1 shows the frequency of usage of HHFNC or NCPAP for all
Standard flows were delivered using the Vapotherm Neonate Nasal
infants admitted during the two study eras. Percentages shown are
Cannula (1.5 mm internal diameter), and HHFNC was generated
the percent of infants who received either NCPAP or HHFNC during
using the Vapotherm 2000i (Vapotherm Inc., Stevensville, MD,
any point during their neonatal intensive care unit (NICU) stay.
USA). Both NCPAP pressure and HHFNC flow rates were adjusted as
During Era 1, about 55% of premature infants less than 30 weeks
needed by clinicians based on clinical exam, chest radiograph
GA received NCPAP at some time during their NICU stay. This
inflation and oxygen saturation levels. The fraction of inspired
number dropped to only 12% in Era 2 whereas the use of HHFNC
oxygen (FiO2) was adjusted according to center protocol targeting
was nearly universal (95%). Similar trends were seen in those
oxygen saturations between 85 and 92% Exclusion criteria included
infants greater than 30 weeks GA, with NCPAP usage decreasing
significant congenital heart disease, chromosomal abnormalities,
from 12 to 2%, and HHFNC usage increasing from 11 to 57%
genetic syndromes or other major congenital malformations.
during Era 1 versus Era 2, respectively.
Outcomes measures of interest included death, days on
For those infants born at less than 30 weeks, regardless of
mechanical ventilation, need for reintubation, air leak, infection,
respiratory support received, there were no differences noted in
BPD (defined as an ongoing requirement for supplemental oxygen
mean gestation, birth weight, BPD and/or death between Era 1 and
at 36 weeks corrected gestational age), necrotizing enterocolitis
2 (Table 2). Additionally, the numbers of infants admitted by week
(NEC, either documented pneumatosis intestinalis or requiring
of gestation from less than 24 to 30 weeks were similar between the
surgical intervention), patent ductus arteriosus (PDA, either
two eras (Table 2). There was a significantly higher number of
receiving indomethacin or surgical ligation), severe
ventilator-days per patient, however, observed in Era 1 as compared
intraventricular hemorrhage (IVH, Papile’s grade 3 or 4),
retinopathy of prematurity (ROP), days to full feeds (120 ml/kg/day) and hospital LOS.
Statistical analyses included Student’s t-test for continuous data
We further analyzed selected outcomes for those babies placed on
and Fisher’s exact test and w2 test for categorical data. P-values less
either NCPAP or HHFNC as an early mode of respiratory support
High flow nasal cannula versus NCPAPMT Shoemaker et al
within the first 96 h of life. Thirty-six of 97 (37%) infants in Era 1
and the mean number of ventilator-days before receiving either
and 65 of 103 (63%) infants in Era 2 born at less than 30 weeks
NCPAP or HHFNC were similar (1.5 days; Table 4). There were no
EGA received either early NCPAP or HHFNC and were included in
significant differences in major clinical outcomes including death,
the retrospective cohort (Figure 1). Of note, only two of 21 (10%)
BPD, ventilator-days, NEC, PDA, severe IVH, LOS, ROP or time to
infants born between 24 and 25 6/7 weeks gestation in Era 1
full feeds (Table 5). Although each group had the same percentage
received early NCPAP compared to 11 of 25 (44%) managed with
of infants with positive blood cultures, there were more cases of
early HHFNC in Era 2. Reasons that infants did not receive the
Gram-negative blood cultures documented in the HHFNC group
respiratory mode of interest vary and are shown in Table 3. Over
(not statistically significant). The Gram-negative organisms
half of the infants excluded in each era resulted from either
isolated in Era 1 were Escherichia coli (1) and Klebsiella
prolonged intubation (>96 h) or death before extubation.
pneumonia (1) and in Era 2, K. pneumonia (2), E. coli (2),
Characteristics of each group were similar as shown in Table 4.
E. cloaclae (3), Pseudomonas aeruginosa(1) and Ralstonia
The majority of infants in both eras were initially supported by
pickettii (1) No deaths occurred in either group of infants with
mechanical ventilation for 1 to 2 days (61 and 66% respectively),
documented Gram-negative bacteremia. Although there were nodifferences in outcomes between the two groups, more infants inthe NCPAP group were either intubated after initially receiving
Table 1 Increase in usage of HHFNC after its introduction
NCPAP or reintubated from NCPAP after an extubation attemptcompared to infants initially managed with or extubated to HHFNC
Because there was a discrepancy in the two groups in patient
numbers for the smallest babies (<26 weeks) included in the study
(2 versus 11), additional analyses were performed comparinginfants 26 to 29 6/7 weeks EGA (Table 6). Although there was a
trend toward less ventilator-days per patient (2.9 versus 4.5,
P ¼ 0.25) and less BPD (20 versus 31%, P ¼ 0.23) in the HHFNC
compared to the NCPAP group, these findings were not statisticallydifferent. However, there was a significantly lower intubation/
reintubation rate in Era 2 versus Era 1 (6 versus 35%, respectively,
P<0.001), similar to that found for the less than 30 week gestation
cohort as a whole. Outcomes are available for the groups stratified
Abbreviations: GA, gestational age; HHFNC, humidified high flow nasal cannula; NCPAP,
into 24 to 25 6/7, 26 to 27 6/7 and 28 to 29 6/7 weeks GA as well
nasal continuous positive airway pressure.
As more infants in the HHFNC group had antenatal steroids
Table 2 Characteristics and outcomes of infants <30 weeks GA before
administered as well as delivered via cesarean section, we
Table 3 Reasons for exclusion of <30 weeks GA infants from analysis
Abbreviations: BPD, bronchopulmonary dysplasia; GA, gestational age; HHFNC,
Abbreviations: GA, gestational age; HHFNC, humidified high flow nasal cannula; NCPAP,
humidified high flow nasal cannula; s.d., standard deviation.
nasal continuous positive airway pressure.
Table 4 Characteristics of infants included in the analysis
Table 5 Outcomes of infants in the analysis
Total ventilator-days per patient (mean±s.d)
Ventilator-days post NCPAP/HHFNCa (mean±s.d)
Abbreviations: BPD, bronchopulmonary dysplasia; GA, gestational age; HHFNC,
humidified high flow nasal cannula; IVH, intraventricular hemorrhage; NCPAP, nasal
continuous positive airway pressure; NEC, necrotizing enterocolitis; PDA, patent ductus
arteriosus; ROP, retinopathy of prematurity. a
Number of ventilator-days per patient after receiving the early respiratory mode of
interest (NCPAP in Era 1 or HHFNC in Era 2).
bOne infant died in Era 1 and two were transferred before 36 weeks corrected GA while
still receiving supplemental oxygen. In Era 2, 2 infants died and two were transferred. cNumber of infants intubated after a trial on the respiratory mode of interest or
reintubated after being extubated to the respiratory mode of interest.
dOnly ROP documented within the hospitalization. Information was not available for allinfants.
eDefined as stage 3 or greater in any zone or stage 2 in zone 1.
multivariate logistic regression was performed controlling for GA
<26 weeks, male sex, outborn status, cesarean section and no
antenatal steroid administration, there were more (re)intubations
in the NCPAP compared to the HHFNC group (O.R. 10.7, 95% CI2.6 to 44, P ¼ 0.02). No statistical difference was seen for BPD (OR
Abbreviations: HHFNC, humidified high flow nasal cannula; NCPAP, nasal continuous
2.43, 95% CI 0.81 to 7.2, P ¼ 0.23) or gram negative bacteremia
positive airway pressure. aInitial support when placed on the respiratory mode of interest (NCPAP or HHFNC).
(OR 0.52, 95% CI 0.09 to 2.79, P ¼ 0.5) between the two groups.
bNumber of ventilator-days per patient before receiving the early respiratory mode ofinterest (NCPAP in Era 1 or HHFNC in Era 2).
performed logistic regression analyses, which did not show an
The use of HHFNC has increased in many NICUs over the past
association between antenatal steroids or mode of delivery and BPD
several years. Potential reasons for this increase include its ease of
or (re)intubation. Only low birth weight, low GA and male sex were
use and perceived improved tolerance with minimal nasal trauma
positive predictors of BPD (Table 7), consistent with earlier
compared to NCPAP. Clinical outcomes associated with the use of
observations.4 Furthermore, infants who received antenatal steroids
HHFNC are anecdotally perceived by some neonatologists to be at
had a higher BPD rate compared to those who did not (32 versus
least similar to those of NCPAP usage. Although HHFNC has been
19%, P ¼ 0.8) despite similar (re)intubation rates (19%). When
widely accepted clinically, there is scant data regarding its efficacy
High flow nasal cannula versus NCPAPMT Shoemaker et al
Table 6 Outcomes of infants 26–29 6/7 weeks GA included in the
0.05 0.73 0.54–1.00 0.0001 0.53 0.37–0.74
Ventilator-days post NCPAP/HHFNCa (mean±s.d)
Abbreviations: BPD, bronchopulmonary dysplasia; BW, birth weight; CI, confidence
interval; GA, gestational age; NCPAP, nasal continuous positive airway pressure; OR, oddsratio.
aBirth weight in increments of 100 g; GA in increments of 1 week.
bOR+95% CI of infants in Era 1 compared to those in Era 2 for selected outcomes
correcting for GA<26 weeks, male sex, outborn status, no antenatal steroids and cesarean
Abbreviations: BPD, bronchopulmonary dysplasia; EGA, estimated gestational age; GA,gestational age; HHFNC, humidified high flow nasal cannula; IVH, intraventricularhemorrhage; NCPAP, nasal continuous positive airway pressure; NEC, necrotizingenterocolitis; PDA, patent ductus arteriosus.
mode during the study period. Specifically, there were no obvious
aNumber of ventilator-days per patient after receiving the early respiratory mode of
changes identified in ventilator management, intubation or
interest (NCPAP in Era 1 or HHFNC in Era 2). b
extubation criteria, or antenatal steroid usage. Patient
Number of infants intubated after a trial on the respiratory mode of interest or
reintubated after being extubated to the respiratory mode of interest.
demographics and GA distribution were very similar between thetwo eras. In general, the majority of extremely low birth weight(ELBW) infants (<28 weeks GA) in our practice are
and safety. One published trial exists comparing standard
prophylactically intubated and administered exogenous surfactant
high-flow nasal cannula (SHFNC) with NCPAP in which SHFNC
with the goal of either immediate extubation to NCPAP or HHFNC,
was shown to be as efficacious as NCPAP in preventing apnea of
or early extubation following limited mechanical ventilation.
prematurity.14 Otherwise there have been only a few abstracts9–13
Although on a respiratory support modality, permissive hypercapnia
with small patient numbers reported to date describing the safety of
is usually tolerated with the goal of maintaining arterial pH>7.25
this modality compared to NCPAP in premature infants, and no
coupled with a concerted effort to limit excessive oxygen exposure.
controlled clinical trials evaluating its utility in this population.
The above practice guidelines have been in place at both of our
In this report we describe our experience in two large regional
study centers for a number of years preceding the defined study
medical centers where HHFNC has largely replaced NCPAP as the
period; this is consistent with the approach adopted by many
preferred mode of noninvasive respiratory support, particularly in
institutions over the past decade in an effort to avoid or limit the
those infants born at less than 30 weeks GA (Part 1). By comparison
duration of mechanical ventilation in preterm infants with
to historical data before its widespread introduction, we have shown
that HHFNC appears to be well tolerated and to provide similar
Historical problems associated with using an early NCPAP
outcomes when compared to NCPAP. Death and BPD rates were
strategy in ELBW infants include difficulty with comfortably
similar for premature infants before and following the introduction
maintaining a functional patient–device interface and the
of HHFNC, and there was a decrease in ventilator-days.
associated nasal trauma that can occur with using this modality.
We are not aware of any significant shift in clinical practice
The application of HHFNC in these small babies, however, is much
other than the introduction of HHFNC as a respiratory support
simpler, which is likely one of the main reasons for its widespread
acceptance into a number of neonatal units. Additionally, the ease
flow.21 In our study, no infant supported with HHFNC during their
of use of HHFNC as compared to NCPAP (at least as perceived by
hospitalization in either Era 1 or Era 2 (whether they were
medical, nursing and respiratory care providers) may have
included in the analysis or not) had a pneumothorax while on this
contributed to a greater willingness to use HHFNC and bias toward
respiratory mode. Further studies measuring airway pressure
its more successful utility as a mode of respiratory support.
generated with HHFNC devices in premature neonates, to include
When infants less than 30 weeks GA were compared by early
how pressures vary with weight and at different flow rates, need to
mode of respiratory support (NCPAP or HHFNC), outcomes were
similar (Part 2). There were no statistically significant differences
Recently the device we used to deliver high flow, the Vapotherm
in ventilator-days, deaths, infections, IVH or LOS. There is debate
2000i, was recalled owing to concerns of increased Gram-negative
whether early NCPAP decreases the risk of BPD in infants <30
bacteremia, specifically R. pickettii.22 In our study, although we
weeks GA.4–8 Our data did not show a difference in BPD rates
found the overall rate of bacteremia to be similar between the two
between the NCPAP and HHFNC groups. Although there was a
Eras, we did find a higher incidence of Gram-negative bacteremia
lower rate of BPD in infants who received HHFNC as first intention
in the infants who received HHFNC as an early mode of respiratory
versus NCPAP, especially in the 26 to 29 6/7 week GA group, the
support versus NCPAP. Only one infant grew R. pickettii. Although
numbers were small and the power inadequate. The majority of
we cannot directly attribute the increased Gram-negative
infants in both eras included in the analysis were intubated for 1 to
bacteremia to use of HHFNC, the relationship warrants further
2 days before receiving either NCPAP or HHFNC (Table 4) and
investigation. Based on our data, approximately 250 infants would
outcomes in these infants were not different. Six of the nine infants
need to be enrolled in a prospective study to detect a significant
who received NCPAP first (GA 28.8±1.1 weeks, birth weight (BW)
difference in Gram-negative bacteremia (80% power). A recent
1205±197 g) versus only three of the 17 infants who received
report described a positive association between nasal cannula
HHFNC first (GA 28.8±0.7 weeks, BW 1094±202 g) were later
continuous positive airway pressure (but not mechanical
intubated for respiratory reasons, spending an average of 5.1±5.7
ventilation) and late onset Gram-negative blood infections in low
and 1.6±2.9 days, respectively, mechanically ventilated. Although
birth weight infants, which the authors attributed to increasing
this finding is of interest, it is possible that some babies may have
nasal mucosa damage from the cannulas.23 As HHFNC maintains a
been placed on HHFNC in Era 2 who otherwise would have done
normal mucosa better than standard high flow nasal cannula,24
just as well on less respiratory support (i.e., <2 LPM nasal cannula
it remains to be seen if infection rates will be altered.
or room air), which would have contributed to relatively more
Although this study is limited by its relatively small size and
infants being intubated in the NCPAP cohort as well as to a
inclusion of only those infants less than 30 weeks GA, the data
reduction in the BPD rates reported for HHFNC babies in Era 2.
presented here indicate that HHFNC may represent a well-tolerated
There are existing concerns among neonatologists regarding the
and effective alternative respiratory support mode to NCPAP in the
widespread application and usage of HHFNC in premature infants
preterm infant population. Its potential advantages include its
in the absence of sufficient published literature supporting its
simplicity, improved tolerability with less injury to the nasal
utility and safety. Particular concern has focused on the imprecise
architecture and mucosa, and perhaps greater clinical utility in
regulation and generation of pressure that may occur at higher
managing respiratory distress in premature infants. However, owing
flows, especially in the smallest of infants, as well as the potential
to unresolved infection concerns and the paucity of published
for a significant increased work of breathing with HHFNC devices
outcomes to date, the safety and utility of HHFNC as compared to
as compared to NCPAP.15–18 Of interest, a recently published small
more traditional respiratory support modes remains unproven and
randomized trial did not show increased work of breathing or
needs to be further investigated. We believe our experience warrants
respiratory rates of preterm infants <2 kg on HHFNC (3 to 5 LPM)
a large, randomized controlled trial comparing the efficacy, safety
compared to preterm infants receiving NCPAP set at 6 cm H2O.19
Additionally, recorded esophageal pressures were consistently
<4 cm H2O at flow rates of 3 to 5 LPM, similar to delivered NCPAP
pressures. Previously, Locke et al.20 reported that as much as 9 cm
H2O pressure measured by esophageal balloon manometry can be
The opinions expressed are of the authors only and do not necessarily represent
generated with as little as 2 LPM SHFNC in 3 mm cannulas but not
those of the Department of the Air Force or the Department of Defense.
in 2 mm cannulas. The cannulas used in our infants were 1.5 mm,and although we did not quantify pressure, pressures generated didnot appear to be excessive based on clinical evaluations including
serial chest radiographs. One recent report looking at airway
Angus DC, Linde-Zwirble WT, Clermont G, Griffen MF, Clark RH.
pressure generated in preterm infants with the Vapotherm device
Epidemiology of neonatal respiratory failure in the United States. Am J Resp
found a high pressure of only 4.5 cm H2O with up to 8 LPM of
Crit Care Med 2001; 164: 1154–1161.
High flow nasal cannula versus NCPAPMT Shoemaker et al
Hudson LD. Progress in understanding ventilator-induced lung injury. JAMA
conventional nasal continuous positive airway pressure. Pediatrics 2001;
Jobe AH, Ikegami M. Mechanisms initiating lung injury in the preterm
Chang GC, Cox CC, Shaffer TH. Nasal cannula, CPAP, and Vapotherm: effect
infant. Early Hum Dev 1998; 53: 81–94.
of flow on temperature, humidity, pressure and resistance. Pediatr Acad Soc
Rich W, Finer NN, Vaucher YE. Ten-year trends in neonatal assisted
ventilation of very low- birthweight infants. J Perinatol 2003; 28: 660–663.
Courtney SE, Pyon KH, Saslow JG, Arnold GK, Pandit PB, Habib RH. Lung
Jegatheesan P, Keller RL, Hawgood S. Early variable-flow nasal continuous
recruitment and breathing pattern during variable versus continuous flow
positive pressure in infants < or ¼ 1000 grams at birth. J Perinatol 2006;
nasal continuous positive airway pressure in premature infants: an
evaluation of three devices. Pediatrics 2001; 107: 304–308.
Aly H, Milner JD, Patel K, El-Mohandes AA. Does the experience with the use
Finer NN. Nasal cannula use in the preterm infant: oxygen or pressure?
of nasal continuous positive airway pressure improve over time in extremely
low birth weight infants? Pediatrics 2004; 114: 697–702.
Walsh M, Engle W, Laptook A, Kazzi SNJ, Buchter S, Rasmussen M et al.
Narendran V, Donovan EF, Hoath SB, Akinbi HT, Steichen JJ, Jobe AH. Early
Oxygen delivery through nasal cannulae to preterm infants: can practice be
bubble CPAP and outcomes in ELBW preterm infants. J Perinatol 2003; 23:
improved? Pediatrics 2005; 116: 857–861.
Saslow JG, Aghai ZH, Nakhla TA, Hart JJ, Lawrysh R, Stahl GE et al. Work of
Davis PG, Henderson-Smart DJ. Post-extubation prophylactic nasal
breathing using high-flow nasal cannula in preterm infants. J Perinatol
continuous positive airway pressure in preterm infants: systematic review
and meta-analysis. J Paediatr Child Health 1999; 35: 367–371.
Locke RG, Wolfson MR, Shaffer TH, Rubenstein SD, Greenspan JS.
Nair G, Karna P. Comparison of the effects of Vapotherm and nasal CPAP in
Inadvertent administration of positive end-distending pressure during nasal
respiratory distress in preterm infants. Pediatr Acad Soc 2005; 57: 2054.
cannula flow. Pediatrics 1993; 91: 135–138.
Ovalle OO, Gomez T, Troncoso G, Palacios J, Ortiz E. High flow nasal
Kubicka Z, Limauro J, Darnall R. High flow nasal cannula therapy with
cannula after surfactant treatment for infant respiratory distress syndrome in
Vapothem: yet another way to deliver CPAP? Pediatr Acad Soc 2006; 59:
preterm infants <30 weeks. Pediatr Acad Soc 2005; 57: 3417.
Ramanathan A, Cayabyab R, Sardesai S, Siassi B, Seri I, Ramanathan R.
Center for Disease Control Convention. Ralstonia associated with Vapotherm
High flow nasal cannula use in preterm and term newborns admitted to
oxygen delivery device – United States, 2005. Morb Mortal Wkly Rep 2005;
neonatal intensive care unit: A prospective, observational study. Pediatr Acad
Graham III PL, Begg MD, Larson E, Della-Latta P, Allen A, Saiman L. Risk
Sanchez F, Sabato K. Very high nasal cannula-alternative to NCPAP in select
Factors for late onset Gram-negative sepsis in low birth weight infants
ICN patients? Respir Care 2004; 49: 1373.
hospitalized in the neonatal intensive care unit. Pediatr Infect Dis J 2006;
Holleman-Duray DL, Kaupie DL, Weiss MG. Safety and efficacy of the
Vapotherms high flow humidification system and an early extubation
Woodhead DD, Lambert DK, Clark JM, Christensen RD. Comparing two
protocol. Pediatr Acad Soc 2006; 59: 517.
methods of delivering high-flow gas therapy by nasal cannula following
Sreenan C, Lemke RP, Hudson-Mason A, Osiovich H. High-flow nasal
endotracheal extubation: a prospective, randomized, masked, crossover trial.
cannulae in management of apnea of prematurity: a comparison with
Supplementary Information accompanies the paper on the Journal of Perinatology website (http://www.nature.com/jp)
5-HTP - 5-Hydroxytryptophan aus Griffonia Simplicifolia Hilft beim natürlichen Einschlafen. Verringert die Schmerzempfindlichkeit. Wirkt als natürliches Mittel gegen Depressionen. Lindert Migränekopfschmerzen. Hilft bei der Verminderung von Angst und Stress. Hilft bei der Linderung einiger Symptome von biologischen Störungen im Körper, die durch Alkohol ausgelöst werden, und ist e
 Journal of Perinatology (2007) 27, 85–91
r 2007 Nature Publishing Group All rights reserved. 0743-8346/07 $30
ORIGINAL ARTICLEHigh flow nasal cannula versus nasal CPAP for neonatal
respiratory disease: a retrospective study
MT Shoemaker1, MR Pierce2, BA Yoder3 and RJ DiGeronimo11Wilford Hall USAF Medical Center, Lackland AFB, TX, USA; 2Pediatrix Medical Group, Santa Rosa Children’s Hospital, San Antonio,TX, USA and 3Primary Children’s Medical Center, University of Utah, Salt Lake City, UT, USA
cost. One report put the cost at 4.4 billion dollars per year in the
Objective: Our objective is to assess the frequency of usage, safety and
United States, and this only includes the time in the neonatal
clinical utility of humidified high flow nasal cannula (HHFNC) in two tertiary
intensive care unit.1 The current practice of most neonatologists
care hospitals and compare outcomes to a historical control group of premature
reflects the belief that limited exposure to invasive mechanical
infants who received nasal continuous positive airway pressure (NCPAP).
Journal of Perinatology (2007) 27, 85–91
r 2007 Nature Publishing Group All rights reserved. 0743-8346/07 $30
ORIGINAL ARTICLEHigh flow nasal cannula versus nasal CPAP for neonatal
respiratory disease: a retrospective study
MT Shoemaker1, MR Pierce2, BA Yoder3 and RJ DiGeronimo11Wilford Hall USAF Medical Center, Lackland AFB, TX, USA; 2Pediatrix Medical Group, Santa Rosa Children’s Hospital, San Antonio,TX, USA and 3Primary Children’s Medical Center, University of Utah, Salt Lake City, UT, USA
cost. One report put the cost at 4.4 billion dollars per year in the
Objective: Our objective is to assess the frequency of usage, safety and
United States, and this only includes the time in the neonatal
clinical utility of humidified high flow nasal cannula (HHFNC) in two tertiary
intensive care unit.1 The current practice of most neonatologists
care hospitals and compare outcomes to a historical control group of premature
reflects the belief that limited exposure to invasive mechanical
infants who received nasal continuous positive airway pressure (NCPAP).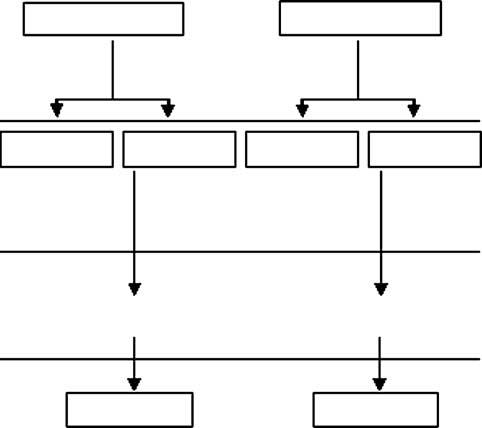

 Center, Lackland AFB, TX, USA and Christus Santa Rosa Children’s
Hospital, San Antonio, TX, USA) during two study periods. The
study periods were defined as August 2003 through June 2004
(Era 1) and August 2004 through June 2005 (Era 2). These timeperiods were based on the identification of June 2004 as a time
point in both centers when the use of HHFNC became readilyavailable as an alternative therapy to NCPAP for neonates withrespiratory distress. The study was divided into two parts: (1) The
first part describes the change in frequency of usage of HHFNC and
NCPAP and compares selected outcomes of premature infants born
during the two eras; and (2) the second part analyzes the outcomes
of a defined cohort of infants less than 30 weeks gestational age(GA) who received either NCPAP or HHFNC as an early mode of
respiratory support during the two eras (Figure 1).
Center, Lackland AFB, TX, USA and Christus Santa Rosa Children’s
Hospital, San Antonio, TX, USA) during two study periods. The
study periods were defined as August 2003 through June 2004
(Era 1) and August 2004 through June 2005 (Era 2). These timeperiods were based on the identification of June 2004 as a time
point in both centers when the use of HHFNC became readilyavailable as an alternative therapy to NCPAP for neonates withrespiratory distress. The study was divided into two parts: (1) The
first part describes the change in frequency of usage of HHFNC and
NCPAP and compares selected outcomes of premature infants born
during the two eras; and (2) the second part analyzes the outcomes
of a defined cohort of infants less than 30 weeks gestational age(GA) who received either NCPAP or HHFNC as an early mode of
respiratory support during the two eras (Figure 1). High flow nasal cannula versus NCPAPMT Shoemaker et al
within the first 96 h of life. Thirty-six of 97 (37%) infants in Era 1
and the mean number of ventilator-days before receiving either
and 65 of 103 (63%) infants in Era 2 born at less than 30 weeks
NCPAP or HHFNC were similar (1.5 days; Table 4). There were no
EGA received either early NCPAP or HHFNC and were included in
significant differences in major clinical outcomes including death,
the retrospective cohort (Figure 1). Of note, only two of 21 (10%)
BPD, ventilator-days, NEC, PDA, severe IVH, LOS, ROP or time to
infants born between 24 and 25 6/7 weeks gestation in Era 1
full feeds (Table 5). Although each group had the same percentage
received early NCPAP compared to 11 of 25 (44%) managed with
of infants with positive blood cultures, there were more cases of
early HHFNC in Era 2. Reasons that infants did not receive the
Gram-negative blood cultures documented in the HHFNC group
respiratory mode of interest vary and are shown in Table 3. Over
(not statistically significant). The Gram-negative organisms
half of the infants excluded in each era resulted from either
isolated in Era 1 were Escherichia coli (1) and Klebsiella
prolonged intubation (>96 h) or death before extubation.
High flow nasal cannula versus NCPAPMT Shoemaker et al
within the first 96 h of life. Thirty-six of 97 (37%) infants in Era 1
and the mean number of ventilator-days before receiving either
and 65 of 103 (63%) infants in Era 2 born at less than 30 weeks
NCPAP or HHFNC were similar (1.5 days; Table 4). There were no
EGA received either early NCPAP or HHFNC and were included in
significant differences in major clinical outcomes including death,
the retrospective cohort (Figure 1). Of note, only two of 21 (10%)
BPD, ventilator-days, NEC, PDA, severe IVH, LOS, ROP or time to
infants born between 24 and 25 6/7 weeks gestation in Era 1
full feeds (Table 5). Although each group had the same percentage
received early NCPAP compared to 11 of 25 (44%) managed with
of infants with positive blood cultures, there were more cases of
early HHFNC in Era 2. Reasons that infants did not receive the
Gram-negative blood cultures documented in the HHFNC group
respiratory mode of interest vary and are shown in Table 3. Over
(not statistically significant). The Gram-negative organisms
half of the infants excluded in each era resulted from either
isolated in Era 1 were Escherichia coli (1) and Klebsiella
prolonged intubation (>96 h) or death before extubation. Table 4 Characteristics of infants included in the analysis
Table 5 Outcomes of infants in the analysis
Total ventilator-days per patient (mean±s.d)
Ventilator-days post NCPAP/HHFNCa (mean±s.d)
Abbreviations: BPD, bronchopulmonary dysplasia; GA, gestational age; HHFNC,
humidified high flow nasal cannula; IVH, intraventricular hemorrhage; NCPAP, nasal
continuous positive airway pressure; NEC, necrotizing enterocolitis; PDA, patent ductus
arteriosus; ROP, retinopathy of prematurity.
Table 4 Characteristics of infants included in the analysis
Table 5 Outcomes of infants in the analysis
Total ventilator-days per patient (mean±s.d)
Ventilator-days post NCPAP/HHFNCa (mean±s.d)
Abbreviations: BPD, bronchopulmonary dysplasia; GA, gestational age; HHFNC,
humidified high flow nasal cannula; IVH, intraventricular hemorrhage; NCPAP, nasal
continuous positive airway pressure; NEC, necrotizing enterocolitis; PDA, patent ductus
arteriosus; ROP, retinopathy of prematurity. High flow nasal cannula versus NCPAPMT Shoemaker et al
Table 6 Outcomes of infants 26–29 6/7 weeks GA included in the
0.05 0.73 0.54–1.00 0.0001 0.53 0.37–0.74
Ventilator-days post NCPAP/HHFNCa (mean±s.d)
Abbreviations: BPD, bronchopulmonary dysplasia; BW, birth weight; CI, confidence
interval; GA, gestational age; NCPAP, nasal continuous positive airway pressure; OR, oddsratio.
High flow nasal cannula versus NCPAPMT Shoemaker et al
Table 6 Outcomes of infants 26–29 6/7 weeks GA included in the
0.05 0.73 0.54–1.00 0.0001 0.53 0.37–0.74
Ventilator-days post NCPAP/HHFNCa (mean±s.d)
Abbreviations: BPD, bronchopulmonary dysplasia; BW, birth weight; CI, confidence
interval; GA, gestational age; NCPAP, nasal continuous positive airway pressure; OR, oddsratio. acceptance into a number of neonatal units. Additionally, the ease
flow.21 In our study, no infant supported with HHFNC during their
of use of HHFNC as compared to NCPAP (at least as perceived by
hospitalization in either Era 1 or Era 2 (whether they were
medical, nursing and respiratory care providers) may have
included in the analysis or not) had a pneumothorax while on this
contributed to a greater willingness to use HHFNC and bias toward
respiratory mode. Further studies measuring airway pressure
its more successful utility as a mode of respiratory support.
acceptance into a number of neonatal units. Additionally, the ease
flow.21 In our study, no infant supported with HHFNC during their
of use of HHFNC as compared to NCPAP (at least as perceived by
hospitalization in either Era 1 or Era 2 (whether they were
medical, nursing and respiratory care providers) may have
included in the analysis or not) had a pneumothorax while on this
contributed to a greater willingness to use HHFNC and bias toward
respiratory mode. Further studies measuring airway pressure
its more successful utility as a mode of respiratory support. High flow nasal cannula versus NCPAPMT Shoemaker et al
Hudson LD. Progress in understanding ventilator-induced lung injury. JAMA
conventional nasal continuous positive airway pressure. Pediatrics 2001;
Jobe AH, Ikegami M. Mechanisms initiating lung injury in the preterm
Chang GC, Cox CC, Shaffer TH. Nasal cannula, CPAP, and Vapotherm: effect
infant. Early Hum Dev 1998; 53: 81–94.
High flow nasal cannula versus NCPAPMT Shoemaker et al
Hudson LD. Progress in understanding ventilator-induced lung injury. JAMA
conventional nasal continuous positive airway pressure. Pediatrics 2001;
Jobe AH, Ikegami M. Mechanisms initiating lung injury in the preterm
Chang GC, Cox CC, Shaffer TH. Nasal cannula, CPAP, and Vapotherm: effect
infant. Early Hum Dev 1998; 53: 81–94.