Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Cancer dacus 21 ottobre 2012 jco
The optimal duration of low molecular weight heparin for the treatment of cancer- related deep vein thrombosis: the Cancer-DACUS Study
Running Title: Residual vein thrombosis and low molecular weight heparins
1Sergio Siragusa, 1Giorgia Saccullo, 1Alessandra Malato, 2Walter Ageno, 3Davide Imberti
4Doris Mascheroni, 5Eugenio Bucherini, 6Pina Gallucci, 7Andrea D’Alessio, 8Tullia Prantera
9Pietro Spadaro, 10Stefano Rotondo, 11Pierpaolo Di Micco, 12Vincenzo Oriana, 13Oreste
Urbano, 14Francesco Recchia, 15Angelo Ghirarduzzi, 1Lucio Lo Coco, 1Salvatrice Mancuso,
1Mariasanta Napolitano, 16Antonio Russo, 17Alessandra Casuccio, 18Giovam Battista Rini
Affiliations:
1Cattedra ed Unità di Ematologia con trapianto, Dipartimento di Medicina Interna e
Specialistiche DIMIS, Università degli Studi di Palermo, Palermo
2Dipartimento di Medicina Clinica e Sperimentale, Università dell’Insubria, Varese
3Dipartimento di Medicina Interna, Ospedale di Piacenza
5Modulo Angiologia, Ospedale di Faenza, Italy
6CROB Basilicata, Rionero in Volture, Italy
8Ospedale S. Giovanni di Dio, Crotone, Italy
10Centro Studi Neurolesi, Messina, Italy
12Azienda ospedaliera di Reggio Calabria, Reggio Calabria, Italy
15Azienda Ospedaliera di Reggio Emilia Arcispedale S. Maria Nuova, Reggio Emilia
16Dipartimento di Scienze Chirurgiche ed Oncologiche, Sezione di Oncologia, Università
17Dipartimento di Biomedicina Sperimentale e Neuroscienze Cliniche (BIONEC), Università
18Cattedra di Medicina Interna, Dipartimento di Medicina Interna e Specialistiche DIMIS,
Università degli Studi di Palermo, Palermo
Cattedra ed U.O. di Ematologia con trapianto
Dipartimento di Medicina Interna e Specialistica (DIMIS)
Via del Vespro 127, 90127 Palermo, Italy
Abstract
Purpose: We evaluated the role of Residual Vein Thrombosis (RVT) to assess the optimal
duration of anticoagulants in cancer patients with Deep Vein Thrombosis (DVT) of the lower
limbs. Patients and Methods: Patients with active cancer and a first episode of DVT who
were treated with Low Molecular Weight Heparin (LMWH) for 6 months were eligible for
the study. Patients were managed according to RVT findings: those with RVT were
randomized to continue with LMWH for 6 additional months (Group A1) or to discontinue it
(Group A2), while patients without RVT stopped anticoagulant treatment (Group B). Primary
endpoint was recurrent VTE and secondary endpoint was major bleeding. The patients were
followed up for one year after LMWH discontinuation. Results: Between October 2005 and
April 2010, 409 patients were evaluated and 347 were enrolled in the study. RVT was
detected in 242 (69.7%) patients; recurrence occurred in 15.1% of patients randomized to
continue (Group A1) and in 21.9% of those who discontinued LMWH (Group A2). Only
2.8% of patients without RVT experienced a recurrent event (Group B) (p<0.0005). Three
major bleeding events occurred in Group A1 and two events each in Groups A2 and B
(p=0.880). Overall, 42 (12.1%) patients died, during 12-months follow-up, due to cancer
progression; no statistical significant difference among the groups (p=0.366) were found.
Conclusion: In cancer patients with a first episode of DVT, absence of RVT identifies a
population at a low risk for recurrent thrombotic events.
(ClinicalTrials.gov: number NCT00450645)
Introduction
Venous thromboembolism (VTE) is a frequent complication in cancer patients that
can affect overall survival and quality of life (1-3). Management of deep vein thrombosis
(DVT) and/or pulmonary embolism (PE) may be difficult in this population because of the
high risk of both recurrent events and major hemorrhages, even if adequate vitamin K
antagonist (VKA) therapy is administered (4). It has been reported that the use of low
molecular weight heparin (LMWH) is more effective than VKA without increasing the risk
for major bleeding in the first 6 months of therapy (5), and this treatment is now
recommended as the first option for all cancer patients with acute VTE (6-7). There is less
evidence regarding the duration of anticoagulant treatment; current guidelines suggest that
patients with cancer-related DVT should be treated for 6 months or even longer (6) if the
cancer is still active, but such recommendations do not rely on data from randomized trials,
hence the uncertainty. In the non-cancer patients, the risk of recurrence is usually greatest in
the first year after withdrawal from anticoagulant treatment and gradually diminishes (8),
while the increased bleeding risk may offset the benefits of prolonged VKA (9). For this
reason, new markers, such as residual vein thrombosis (RVT) and D-dimers, have been
proposed to individualize the duration of VKA treatment for the secondary prevention of
VTE (10-13). Results from prospective studies have shown that the absence of RVT or
negative D-dimers may drive safe withdrawal of VKA treatment after 3-6 months from the
index DVT (10). On the other hand, the presence of RVT has been associated with an
increased risk for recurrent venous thrombosis in idiopathic and provoked DVT (11-13). In
comparison to D-dimers, RVT has potential advantages in patients with chronic activation of
coagulation or inflammation, since it is not influenced by factors acting on blood coagulation;
this makes such parameter particularly suitable for cancer patients. However, it is still
unknown whether RVT may be used to optimize the duration of LMWH treatment in cancer
patients, a population at a high-risk for recurrent events.
We therefore performed a randomized study in patients with a first episode of cancer-
related symptomatic DVT of the lower limbs to test the hypothesis that RVT may be used to
establish the optimal duration of LMWH treatment.
Study population
Inclusion criteria were age older than 18 years; symptomatic proximal DVT detected
by compression ultrasonography (C-US), active cancer defined as metastatic or locally-
advanced lung, gastrointestinal (stomach, colon, or rectum), pancreatic, breast, ovarian, or
head and neck cancer, blood cancer and treatment with LMWH for 6 months after the index
event (5). Patients with active cancer and a DVT episode occurring after cancer surgery were
also eligible for the study. Eligible patients were enrolled after written informed consent was
Patients were excluded if they had: Eastern Cooperative Oncology Group score > 2;
previous VTE; antiphospholipid antibody syndrome, or other known thrombophilic states
(such as deficiency in antithrombin, protein C and S, homozygosity for FV Leiden or factor II
G20210A mutations or heterozygous combinations thereof); other conditions requiring
prolonged anticoagulation; active bleeding or bleeding requiring hospitalization, transfusion
or surgical intervention in the past 4 weeks; intracranial bleeding over the past 6 months; high
risk of bleeding (international normalized ratio or activated partial thromboplastin time ratio
above 1.3, or a platelet count lower than 75×109/L); known active gastric or duodenal ulcer;
known cerebral metastases; severe and uncontrolled hypertension; creatinine clearance < 30
ml/min; severe liver insufficiency; unavailability for follow-up.
The study was carried out in accordance with the provisions of the Declaration of
Helsinki and local regulations. The protocol was approved by the institutional review board at
each study center, and written informed consent was obtained from all patients before
Study design and procedures
This multicenter prospective study was carried out between October 2005 and April
2010. At the time of enrolment in the study, at 6 months from the index event, all patients
underwent C-US of the affected leg and images were obtained from the transverse section
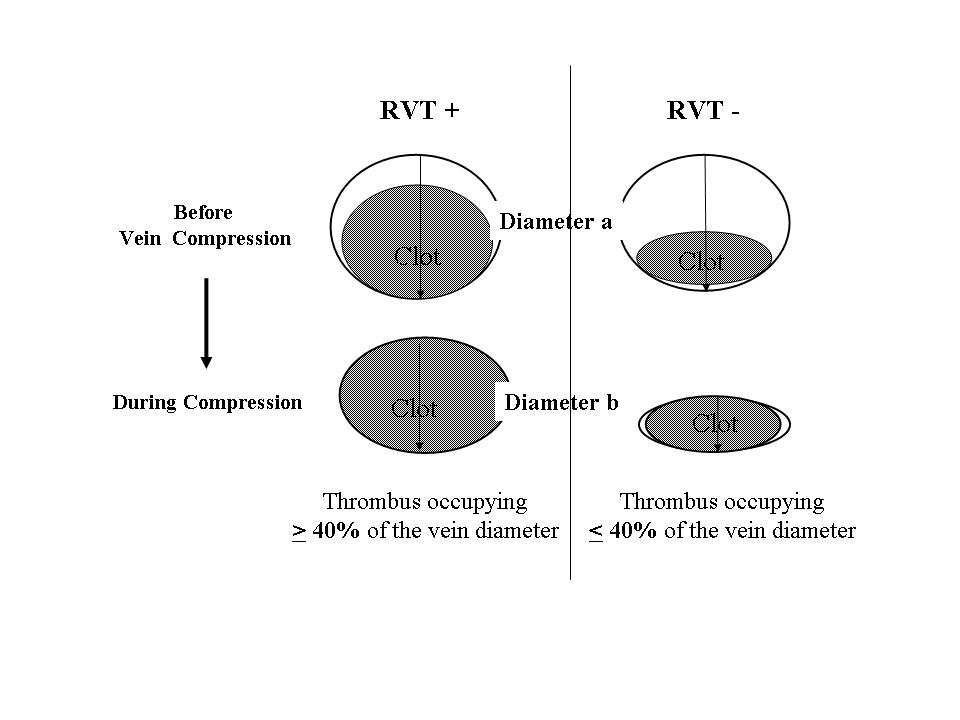
only. Lumen compressibility was then evaluated by gentle pressure of the probe; RVT
diameter was taken by measuring the distance between the anterior and posterior walls of the
vein, on freeze-frame B-mode images, during compression with the ultrasound probe (14).
The examination was performed with the patient in the supine position with the leg externally
rotated and slightly flexed at the knee. Measurements were taken at the common femoral
vein, 1 cm below the inguinal ligament, and at the popliteal vein, at the most prominent
crease in the mid-popliteal fossa. The RVT calculation was made as previously described
(12): RVT = vein diameter during compression (diameter b) x 100/vein diameter before
compression (diameter a). RVT was arbitrarily scored as “absent” when the value was < 40%
of the vein diameter. The patient was considered to have RVT when a persisting thrombus
was shown to be present in at least one of the two examined vein segments (Figure 1).
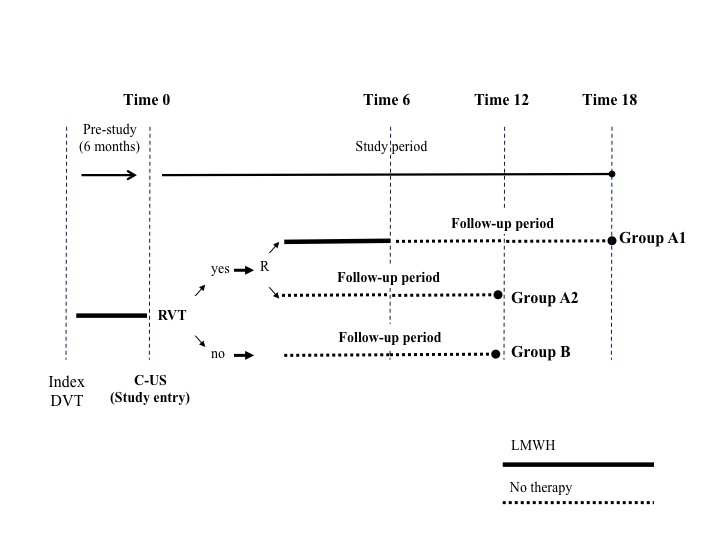
Patients with RVT were then randomized to either stop or continue LMWH
(Nadroparine), administered at 75% of full dose (97 UI antiFXa/kg/twice daily) for 6
additional months (Group A2 and A1, respectively). This dosage was chosen accordingly to
the results of randomized studies that evaluated LMWH in comparison to VKA in cancer
patients with VTE (5, 15). All patients with no evidence of RVT stopped anticoagulation
(Group B) (Figure 2). After the first C-US test performed at the time of enrolment in the
study, patients underwent additional testing only when recurrence was clinically suspected.
Randomization and masking
For each different institution, after signing the informed consent form, patients with
RVT were randomized to either stop or continue LMWH, using sequentially numbered,
sealed, opaque envelopes prepared from a list of computer-generated pseudo-random
numbers. The sequences were balanced in blocks of 10. Patients and treating physicians were
Study outcomes and follow-up
Patients were followed up for one year after LMWH discontinuation (Figure 2)
and were seen at the clinical center at intervals of 3 months. Primary endpoint was
recurrent VTE and secondary endpoint was major bleeding. Patients were instructed to
contact the clinical center if symptoms suggestive of VTE or bleeding developed. In
cases of recurrence, results of C-US were compared with those of the previous
examination. Diagnosis of recurrent DVT was made if a previously fully compressible
segment (contralateral or ipsilateral) became no longer compressible, or if an increase of
> 4 mm in the diameter of the residual thrombus during compression was detected (16);
in undetermined cases, repetition of the test (after 5-7 days) or contrast venography was
performed. In patients with suspected pulmonary embolism, the diagnosis of recurrence
was based on objective algorithms with the use of clinical probability, ventilation–
perfusion lung scanning or helical CT (17-18). Major bleeding was defined as a decrease
in hemoglobin > 2.0 g/dl, intracranial or retroperitoneal bleeding, bleeding requiring
surgical intervention or blood transfusion, or any other bleeding considered clinically
relevant by the physician in charge requiring suspension of anticoagulation and the use of
hemostatic approaches (9). Minor bleeds comprised all other bleeding events. All
suspected outcome events and deaths were evaluated by a central adjudication committee
whose members were unaware of the patient's name, the center where the patient had
been enrolled, the results of RVT assays, and the group assignment. Committee members
also reviewed the results of all clinical investigations without knowing the patient's
name, the group assignment, or the center where RVT had been performed.
Statistical analysis
The sample size was calculated taking into account an incidence of 20% for recurrent
thrombotic events and 5% of complications for the group with the best prognosis (4). An
overall sample size of 300 patients (100 for each study group) was calculated to achieve a
power of 80% to document a difference of at least 15% in at least one of the different head-
to-head comparisons, based on the Bonferroni method for distributing type I error (0.05)
among multiple comparisons. In order to monitor the safety of the trial, an interim analysis
was planned after enrolment of two-thirds of the total patient population. Prior to study onset,
we set up an internal quality control system to assess inter- and intra-examiner reproducibility
for RVT analysis among operators by the use of the unweighted Cohen’s kappa (k) test (19).
Baseline differences between groups were assessed by the chi-square test (Yates’
correction) for categorical variables, and the univariate analysis of variance (ANOVA) for
parametric analyses. Data were analyzed on an intention-to-treat basis. Kaplan-Meier curve
was plotted to estimate the cumulative probability of absence of symptomatic recurrent
thrombosis. Hazard Ratios (HRs) and their 95% confidence intervals (CIs), calculated using
the Cox proportional hazards model were adjusted for age, sex, previous surgery and
presence of metastasis. Data were analyzed using Epi Info software (version 6.0, Centers for
Disease Control and Prevention, Atlanta, GA, USA) and SPSS Software (version 14.0, SPSS
Inc., Chicago, Il, USA). All p-values were two-sided; p-values < 0.05 were considered
Patients and treatment groups
Of the 409 evaluated patients, 62 were excluded: 9 because they did not provide
informed consent, 18 because they required long-term anticoagulation, 7 because of low
platelet count, 12 for recent surgery, 3 for cerebral metastases, and the remaining 13 for organ
failure. A total of 347 patients were therefore included in the study. No patient was lost to
follow-up. RVT was detected in 242 (69.7%) patients who were then randomized to continue
(119 patients; group A1) or to discontinue (123 patients; group A2) anticoagulant treatment
with LMWH. RVT was absent in 105 (30.3%) patients (group B). Baseline patient
characteristics are reported in Table 1. Cancer characteristics, site and chemotherapy
treatments in the different groups are reported in Tables 1 and 2. There were no statistically
significant differences among groups in the prevalence of metastatic cancer, different cancer
types and ongoing chemotherapy. Twenty-three percent of patients had a hematologic cancer,
Outcomes
During the overall follow-up, recurrent events occurred in 18/119 (15.1%) of RVT
patients randomized to continue and 27/123 (21.9%) of those who discontinued LMWH. In
patients without RVT (105, 30.3%), recurrent events occurred in 3 (2.8%) cases (A1 vs A2,
p= 0.150; B vs A1, p=0.002; B vs A2, p<0.0005; Log Rank test) (Table 3 and Figure 4).
The recurrence rate x100 person-year was 11.3 in Group A1, 26.7 in Group A2 and
3.0 in Group B. Most of these events were deep venous thromboses of the lower limbs; in 12
of 48 (25%) cases, thromboses occurred in the contralateral leg. The adjusted hazard ratio
(HR) for recurrent DVT between RVT groups (Group A2 vs A1) was 1.37 (95% confidence
interval [CI], 0.7–2.5; p=0.311). The adjusted HR between group A1 versus RVT-negative
group (B) was 5.68 (CI 1.6–19.4; p=0.006). The adjusted HR between group A2 versus the
RVT-negative group (B) was 7.96 (CI 2.4–26.3; p=0.001). Among participants with RVT,
continuation of heparin therapy reduced the risk of recurrent VTE by about 30% (6.8
Bleeding events was reported in Table 3. During 12-months follow-up, 3 major
bleedings occurred in group A1, and 2 events occurred in both groups A2 and B, respectively
(p=0.880). Among patients randomized to continue LMWH for additional 6 months, patients’
compliance was high: 15 of the 119 patients interrupted LMWH for less of 5 days during
Overall, 42 (12.1%) patients died during 12-months follow-up, all because of cancer
progression: 12 patients (10.1%) died in group A1, 19 (15.4%) in group A2 and 11 (10.5%)
Discussion
Our results suggest that RVT assessment is useful for establishing the optimal
duration of cancer-related DVT, as we previously observed in the non-cancer population (12-
13). In fact, RVT assessment has identified a subset of patients at a lower risk of recurrence
(about 30%) that can safely stop anticoagulation. In high-risk patients (those with persistent
RVT), our data show that interruption of LMWH treatment is associated with a high risk of
recurrence even if anticoagulation is continued for up to 1 year.
LMWH is currently considered the standard of care for cancer-related DVT due to its
favorable safety and efficacy profile even if its optimal duration is still debated. International
guidelines recommend to continue the treatment while the neoplasm is active (6) but cancer
populations differ substantially in terms of type, stage, histology and, consequently, treatment
choice (20). On this basis, the optimal management of anticoagulant therapy should be based
on the possibility of tailoring treatment, according to the type and characteristics of
underlying cancer as well as concomitant chemotherapy.
Such individual-based approach has been experimented in non-cancer population,
where individual markers for establishing the optimal duration of anticoagulant treatment
have been proposed (10-13). Residual Vein Thrombosis and D-dimers have been extensively
evaluated and the results of clinical studies suggest that, after an initial course of treatment
with VKA, a negative D-dimer or the absence of RVT identify patients who can stop
treatment, independently from the pathogenesis of the index DVT. These data are lacking in
the cancer population; among these individual markers, RVT looks more suitable than D-
dimer since it is insensitive to factors affecting blood coagulation (such as infections or
cancer) and it can be performed without interrupting anticoagulation (11-13).
The results of our study have obvious advantages in clinical practice: in low-risk
patients, short-term anticoagulation reduces the clinical burden for both the patient and the
healthcare system, and substantially reduces the overall risk of bleeding that is inherent with
prolonged anticoagulant treatment. These advantages are supported by the fact that we used a
simple and reproducible method for tailoring LMWH duration in cancer-related DVT. This
strategy is important in practical terms as it can be easily and broadly applied. Another
consideration regards mortality among the groups; overall almost 12% of patients died during
the follow-up. This rate was similar regardless of RVT findings or LMWH duration.
However, our study design does not allow us to look at potential advantages in terms of
reducing mortality among groups, as previously reported in patients on LMWH (22-23).
As in the non-cancer population, more than 20% of the recurrent thromboses occurred
in the contralateral leg; whether this fact indicates RVT as a marker of an underlying pro-
thrombotic state, thus triggering a sustained hypercoagulability (24), need to be confirmed in
This study has limitations; first, the trial was not blinded. However, committee
members who were unaware of the results of RVT detection and treatment assignments
assessed recurrent events, thus reducing the risk for diagnostic suspicion bias. Moreover, the
rates of events in the treated and untreated patients are in the range of those reported in the
literature (4, 25). Second, some concerns may arise about the reproducibility of RVT
detection. Prior to the DACUS studies, we tested RVT assessment on a consecutive series of
64 non-compressible venous segments (in popliteal and common femoral veins). The result
of inter- and intra-observer variation assessment among operators was shown to be adequate
(κ =0.95; 95% CI, 0.88 to 1.00) (11, 26). Third, RVT assessment was performed only at the
study entry. We can not exclude that during follow-up some patients, with originally absence
of RVT, could have had abnormal results on repeated testing, providing a detectable warning
sign of recurrent hypercoagulability and an increased risk of thrombosis. Repeated RVT in
patients with an originally absence of residual thrombus may be useful in detecting a late
relapse even if asymptomatic, but this hypothesis should be assessed in future studies. Fourth,
although the study was large enough to detect significant differences between groups in the
frequency of the recurrent venous thromboembolism, it was not large enough to make a
definitive assessment of the relative risk of bleeding. Fifth, in patients without RVT, the
incidence of recurrent VTE was lower (3%) than previously reported in cancer population.
However, if we take in account all patients evaluated in the study (both with and without
RVT), the rate of recurrent VTE was high as 14% an average rate similar to that reported (4-
7). Finally, the robustness of the association between RVT and recurrent VTE has been
recently evaluated in two meta-analyses (26, 27); the results have shown a weaker association
than that previously reported in prospective trials. However, the study by Tan et al. (26)
found across-study heterogeneity (I2=74%) when the analysis was confined to patients with
unprovoked DVT, thereby limiting the study conclusions to such patients. The study by
Carrier et al. (27) was unable to adjust for potential covariates. An updated systematic review
and patient-level meta-analysis on this topic is currently ongoing.
In conclusion, our results indicate that the absence of RVT identifies cancer patients at
a low risk for recurrent thrombotic events. This ability is important in driving a management
strategy for both the prevention of recurrences and the selection of a DVT patient population
who may benefit from a short period of anticoagulation.
Authors’ contributions
Sergio Siragusa: study design, data analysis and interpretation, writing the manuscript
Giorgia Saccullo and Alessandra Malato: study design, data collection, analysis and
Walter Ageno and Davide Imberti: data collection and writing the manuscript
Alessandra Casuccio: data analysis and interpretation, writing the manuscript
References
1. Chew HK, Wun T, Harvey D, et al. Incidence of venous thromboembolism and its effect
on survival among patients with common cancers. Arch Intern Med 166;458–64, 2006
2. Sorensen HT, Mellemkjaer L, Olsen JH, Baron JA. Prognosis of cancers associated with
venous thromboembolism. N Engl J Med 343:1846–50, 2000
3. Bick RL. Cancer-associated thrombosis. N Engl J Med 349:109–111, 2003
4. Prandoni P, Lensing AW, Piccioli A, et al. Recurrent venous thromboembolism and
bleeding complications during anticoagulant treatment in patients with cancer and
venous thrombosis. Blood 100:3484–88, 2002
5. Lee AY, Levine MN, Baker RI, et al. Low-molecular weight heparin versus a coumarin
for the prevention of recurrent venous thromboembolism in patients with cancer. New
6. Kearon C, Akl EA, Comerota AJ, et al. Antithrombotic Therapy for VTE Disease:
Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of
Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 141:e419S-94S,
7. Hull RD, Pineo GF, Brant RF, et al. Long-term low-molecular-weight heparin versus
usual care in proximal-vein thrombosis patients with cancer. Am J Med 119:1062-72,
8. Agnelli G, Prandoni P, Santamaria MG, et al. Three months versus one year of oral
anticoagulant therapy for idiopathic deep venous thrombosis. Warfarin Optimal Duration
Italian Trial Investigators. N Engl J Med 345:165-9, 2001
9. Palareti G, Leali N, Coccheri S, et al. Bleeding complications of oral anticoagulant
treatment: an inception-cohort, prospective collaborative study (ISCOAT): Italian Study
on Complications of Oral Anticoagulant Therapy. Lancet 348:423-8, 2001
10. Palareti G, Cosmi B, Legnani C, et al. D-dimer testing to determine the duration of
anticoagulation therapy. N Engl J Med 355:1780-9, 2006
11. Prandoni P, Lensing AWA, Prins MH, et al. Residual venous thrombosis as a predictive
factor of recurrent venous thromboembolism. Ann Intern Med 137:955-60, 2002
12. Siragusa S, Malato A, Anastasio R, et al. Residual vein thrombosis to establish duration
of anticoagulation after a first episode of deep vein thrombosis: the Duration of
Anticoagulation based on Compression UltraSonography (DACUS) study. Blood 112:
13. Siragusa S, Malato A, Saccullo G, et al. Residual vein thrombosis for assessing duration
of anticoagulation after unprovoked deep vein thrombosis of the lower limbs: the
extended DACUS study. Am J Hematol 86:914-7, 2011
14. Bates SM, Jaeschke R, Stevens SM, et al. Antithrombotic Therapy and Prevention of
Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines. Chest 141:e351S-e418S, 2012
15. Meyer G, Marjanovic Z, Valcke J, et al. Comparison of low-molecular-weight heparin
and warfarin for the secondary prevention of venous thromboembolism in patients with
cancer: a randomized controlled study. Arch Intern Med 162:1729–1735, 2002
16. Prandoni P, Lensing AW, Bernardi E, Villalta S, Bagatella P, Girolami A. The diagnostic
value of compression ultrasonography in patients with suspected recurrent deep vein
thrombosis. Thromb Haemost 88:402-6, 2002
17. Fedullo PF, Tapson VF. The evaluation of suspected pulmonary embolism. N Engl J
18. Kearon C. Diagnosis of pulmonary embolism. Can Med Assoc J 2003;168:183-94
19. Brennan P, Silman A. Statistical methods for assessing observer variability in clinical
20. Imberti D, Agnelli G, Ageno W, et al. Clinical characteristics and management of
cancer-associated acute venous thromboembolism: findings from the MASTER Registry.
21. Di Nisio M, Sohne M, Kamphuisen PW, Büller HR. D-Dimer test in cancer patients with
suspected acute pulmonary embolism. J Thromb Haemost 3:1239-42, 2005
22. Klerk CP, Smorenburg SM, Otten HM, et al. The effect of low molecular weight heparin
on survival in patients with advanced malignancy. J Clin Oncol 23:2130–5, 2005
23. Kakkar AK, Levine MN, Kadziola Z, et al. Low molecular weight heparin, therapy with
dalteparin, and survival in advanced cancer. The Fragmin advanced malignancy outcome
study (FAMOUS). J Clin Oncol 22:1944–8, 2004
24. Spiezia L, Tormene D, Pesavento R, Salmaso L, Simioni P, Prandoni P. Thrombophilia
as a predictor of persistent residual vein thrombosis. Haematologica 93:479-80, 2008
25. Noble S, Pasi J. Epidemiology and pathophysiology of cancer-associated thrombosis. Br
26. Tan M, Bornais C, Rodger M. Interobserver reliability of compression ultrasound for
residual thrombus after first unprovoked deep vein thrombosis. J Thromb Haemost
27. Carrier M, Rodger MA, Wells PS, Righini M, LE Gal G. Residual vein obstruction to
predict the risk of recurrent venous thromboembolism in patients with deep vein
thrombosis: a systematic review and meta-analysis. J Thromb Haemost 9:1119-25, 2011
Table 1. Baseline characteristics by patient group
^P-value refers to chi-square test unless specified; § Univariate analysis of variance
(ANOVA) test; *In the past 3 months; **In the past 3 months or ongoing;
Footnote:
Group A1: patients with RVT who continued LMWH for additional 6 months
Group A2: patients with RVT randomized to stop LMWH
Group B: patients without RVT who stopped LMWH
Table 2. Cancer site and chemotherapy by treatment group
Footnote:
Group A1: patients with RVT who continued LMWH for additional 6 months
Group A2: patients with RVT randomized to stop LMWH
Group B: patients without RVT who stopped LMWH
Table 3. Recurrent thromboembolic and bleeding events by treatment group and cancer
18/119(15.1) 27/123 (21.9) 3/105 (2.8) <0.0005
DVT and PE (pulmonary embolism), N° (%)
DVT in not previous affected leg, N° (%)
* P-value refers to chi-square test unless specified.
** Chi-square test for the comparison of two proportions, expressed as percentage.
Footnote:
Group A1: patients with RVT who continued LMWH for additional 6 months
Group A2: patients with RVT randomized to stop LMWH
Group B: patients without RVT who stopped LMWH
Figure legends
Figure 1. Evaluation of residual vein thrombosis.
RVT calculation = vein diameter during compression (diameter b) x 100 / vein diameter
Figure 2. Study design
A1 indicates patients with RVT who continued LMWH for additional 6 months; A2 indicates
patients with RVT randomized to stop LMWH treatment; B indicates patients without RVT
Figure 3. Trial profile
Figure 4. Kaplan-Meier curve for recurrent VTE in the three groups at 12 month follow-up.
Group B= patients without RVT and without anticoagulation; Group A1 and Group A2
patients with RVT which continue (for 6 months) or stop LMWH treatment.
Enrollment
Excluded (n= 62) ♦ Not meeting inclusion criteria (n=53) ♦ Declined to participate (n=9)
Allocation
♦ Received allocated intervention (n=119)
♦ Received allocated intervention (n=123)
Analysis
Figure 4. Kaplan-Meier curve for recurrent VTE in the three groups at 12-month follow-up
b o l l e t t i n o d ’ i n f o r m a z i o n e s u i f a r m a c i EDITORIALE Nasce prima il farmaco o la malattia? Chi non va di corpo spontaneamente almenoischemica, e poi riammesso in commercio contre volte la settimana da oltre sei mesi è affetto dasevere restrizioni. Ora la storia si ripete, perchéstitichezza cronica. Chi l’ha detto? È una delle de-anche il tegaserod, i
1 2 7 8 T H E Q U E E N S W A Y , E T O B I C O K E , O N , M 8 Z 1 S 3 P H O N E 4 1 6 8 4 8 9 7 9 5 • F A X 4 1 6 5 2 1 7 2 1 6 I R E N E F U N G , M D , F R C P C A L L E R G Y , A S T H M A A N D I M M U N O L O G Y **Note: for skin prick testing to be done at the clinic visit, the patient must refrain from taking oral antihistamines for at least 3 days prior to their appoin
 Enrollment
Enrollment 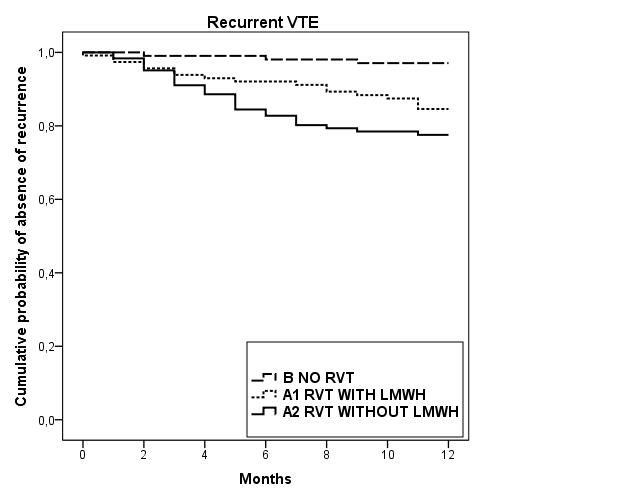 Figure 4. Kaplan-Meier curve for recurrent VTE in the three groups at 12-month
Figure 4. Kaplan-Meier curve for recurrent VTE in the three groups at 12-month