Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Whiplash rove beetle dermatitis among students at university sains malaysia: a case study of 28 year old boy and
International Journal of Pharmacy Teaching & Practices 2012, Vol.3, Issue 4, 429-433.
Role of Bisoprolol Adding oo Ace Inhibitor and Furosemide Combination on the Left Ventr icular Function in Systolic Heart Failure Patients Efta T riastuti 1*, Dadang Hendrawan2, Muha mmad Saifurrohman 3
1Study Program of Pharmacy, Faculty of Medicine, Brawijaya University, Malang, Indonesia
2,3Cardiovascular Department, Dr. Saiful Anwar Hospital, Malang, Indonesia
Introduction Research Article
Heart failure is defined as clinical syndromes (such
Please cite this paper as: Efta Triastuti 1*, Dadang Hendrawan2,
as: short of breathing, activities limitation, or
Muhammad Saifurrohman 3. Role of Bisoprolol Adding oo Ace
pulmonary obstruction) manifest from degradation
Inhibitor and Furosemide Combination on the Left Ventricular Function in Systolic Heart Failure Patients.
of heart function caused by various heart diseases.
This syndrome may lead to quality of life reduction
Corresponding Author:
with higher morbidity and mortality than other
Efta Triastuti
Study Program of Pharmacy, Faculty of Medicine, Brawijaya
American Heart Association guideline of heart failure
recommend β-blocker combined with ACE Inhibitors
and diuretics as an established therapeutic strategy
for stage C systolic heart failure patients throughout
contraindications are not found. Previous study
Abstract
found that this brought many benefits in morbidity
and mortality if given to stabile heart failure
Background: β-blocker is an established therapeutic strategy
patients4,5,6. In contrary, not many physicians
for stage C systolic heart failure based on the American Heart
confidence to prescribe β-blocker to the heart
Association guideline, nonetheless limited studies analyzed the
role of β-blocker primarily Bisoprolol adding to ACE inhibitor
and furosemide combination on the left ventricular function in
β-blocker inhibits the surge of β adrenergic activity.
The surge of β adrenergic activity in heart failure wil
Objectives: This study was designed to analyze the role of
Bisoprolol adding to ACE inhibitor and furosemide
vasocontriction, sodium and water retention which
combination on the ventricular function in patients with
lead to increase cardiac load and aggravate
systolic heart failure particularly on ejection fraction and
hypoperfusion due to inadequate ventricular
ejection. β-blocker act to decrease heart rate and
Subjects & Methods: 40 to 80 years old ambulatory patients
prolonged the ventricular fil ing time, then provide
(N=30) at Dr. Saiful Anwar General Hospital Malang diagnosed
adequate preload at diastolic phase and improve
as stage C systolic heart failure receiving optimum dose of
inhibitor ACE and furosemide combination for at least 2
months. Before Bisoprolol was added, the ejection fraction
Bisoprolol is one of selective β-blocker that available
and the quality of life was observed to assess the baseline left
in indonesia. It has prominently high β1 affinity, low
ventricular function then re-observed after 3 months.
bronchoconstriction effect, and it has no intrinsic
Results: After the adding of Bisoprolol, there were significant
simphatomimetic activity (high bradycardia effect)
differences in ejection fraction (measured by
and membrane stabileity activity therefore has
echocardiography) and quality of life (measured by Minnesota
minimum effect on cardiac conductance3,12.
quality of life living with heart failure questionnaire) with both
The aim of this study is to analyze the role of
P value equal to 0,000 (95% Confidence Interval).
Bisoprolol adding to ACE inhibitor and furosemide
Conclusions: The adding of Bisoprolol to ACE inhibitor and
combination on the ventricular function in patients
Furosemide combination seems to improve the left ventricular
with systolic heart failure particularly on ejection
function in stage C systolic heart failure patients particularly on
ejection fraction and quality of life measurements.
Keywords: heart failure, Bisoprolol, ejection fraction, echocardiography, quality of life
International Journal of Pharmacy Teaching & Practices 2012, Vol.3, Issue 4, 429-433.
Material and Method
differences in distribution, with the P value for those
are > 0.05. Comorbid condition (previous disease
Research was conducted in Dr. Saiful Anwar General Hospital
history) categorized in to three group then examined
Malang, Indonesia between february 2011 to january 2012.
by Chi-Square analysis and resulted P = 0.061. Chi-
This quasi-experimental study used a one group pretest-
Square analysis also conducted to determine the age
posttest design to compare the ejection fraction (by
(divided in to four groups in table 1) and gender
echocardiography) and quality of life (by Minessota Living with
differences and resulted P value 0.141 and 0.465
Heart Failure questionnaire) measurements before and after
respectively. Patients demographic data summarized
the adding of Bisoprolol to ACE inhibitor and furosemide
combination for three months at stage C systolic heart failure
TABLE 1. Patients Demographic Data
40 – 80 years of age stage C systolic heart failure patients with
EF reduction were included. Inclusion criterias were stabile
heart failure, already received the optimum dose of ACE
inhibitor and furosemide, fulfil for Bisoprolol indication.
Patients were excluded if already accepted Bisoprolol before
recruitment, had acute heart failure and needed positive
inotropic except digoxin, comorbid condition which affect to
quality of life such as mitral regurgitation and atrial fibrilation,
cardiogenic shock, bradycardia (heart rate below 60 times per
History of previous illness:
minute), hypotension with systolic pressure below 100 mmHg,
Ejection fraction measured by two operator using
echocardiography with Simpson method of measurement as a
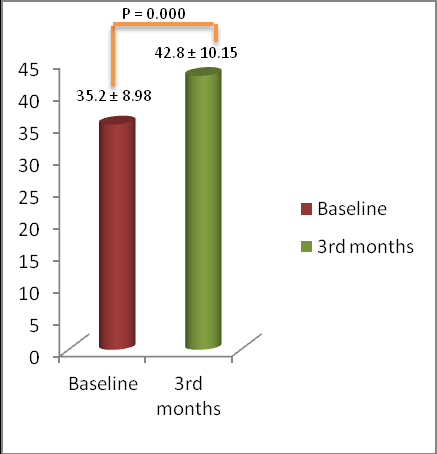
EJECTION FRACTION (EF)
gold standard. Minessota Living with Heart Failure
EF show the fraction of blood that ejected from the
Questionnaire is already used worldwide to measure the
left ventricle. Normal value of EF is in the range
quality of life of heart failure patients.
between 53% to 72% while in heart failure EF may
reduce to 50% or below. Lowest EF value at baseline
This study examined the ambulatory patients of Cardiovascular
was 17% while at endpoint was 24%. Highest EF
Department at Dr. Saiful Anwar General Hospital Malang.
value at baseline was 49% while at endpoint was
Patient adherence has significant contribution to the result of
this study, thus this study enclosed to the high adherence
patients (measured by patients adherence questionnaire).
Normality test for EF showed that endpoint EF data
did not meet Gaussian distribution so that data
DATA ANALYSIS
analysis should used nonparametric test for two
EF and quality of life are dependent variables measured in this
related samples that is Wilcoxon Signed Ranks Test.
study. Both variables show the left ventricular function.
Wilcoxon Signed Ranks Test results showed that
Baseline EF and quality of life were compared to those results
baseline EF were significantly differ from endpoint
three months after Bisoprolol addition using paired t test
EF with P value equal to 0.000 (95% Confidence
analysis in the Statistical Product and Service Solutions (SPSS)
Interval (CI); 0.00 to 0.27). Wilcoxon test results for
version 16. Normal distribution data is required for Paired t
test as a parametric analysis. This is examined by Shapiro-Wilk
analysis for smal size sample (below 50). Wilcoxon analysis is
TABLE 2. Wilcoxon Test Results for EF
the alternate analysis to compare baseline EF and quality of
EF percentage (%)
life to the endpoint if the data do not fulfil normal distribution.
Mean baseline Mean at 3rd months
Total patients who meet inclusion and exclusion criteria
EF mean at baseline and 3rd months comparison by
between february to October 2011 were 30 patients fol owed
Wilcoxon test was displayed to the bar charts in
up for three months with the endpoint measurements last on
January 2012. Chi-square statistical test using SPSS 16 carried out to see the distribution of patient demographic data. Sex, age, and previous disease history respectively did not show significant
International Journal of Pharmacy Teaching & Practices 2012, Vol.3, Issue 4, 429-433.
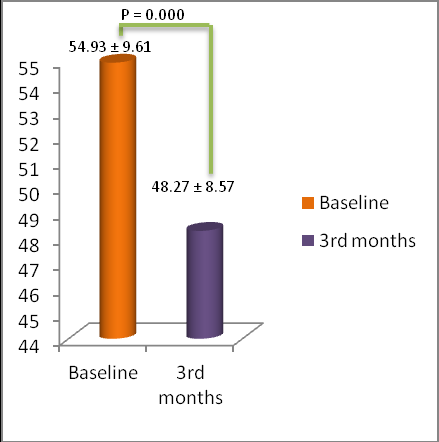
TABLE 3. Paired t Test Results for Sum Score of Minessota Living with Heart Failure Sum Score of Minessota Living with Heart Failure Mean baseline Mean at 3rd months Figure 1. Profile of Baseline Mean Ejection Fraction Compared to Those after the Adding of Bisoprolol for Three Months QUALITY OF LIFE Quality of life for heart failure patients measured by Minessota Living with Heart Failure questionnaire. This questionnaire consists of twenty one questions each questions contain six choices based on the symptoms frequencies which is valued 0, 1, 2, 3, 4, 5 respectively. The more frequent symptoms would provide the higher score for this questionnaire. The maximum score of this questionnaire is 105, which is explained that the heart failure condition has a very high impact to the reduction of quality of life.
Quality of life data taken from the the patients based on the
Figure 2. Profile of Mean Score of Minessota Living
questionnaire results in this study showed that the highest
with Heart Failure Questionnaire Comparison
score of Minessota Living with Heart Failure Questionnaire was
70 at baseline and 64 after three months receiving Bisoprolol.
Discussion
While the lowest score for this questionnaire was 37 at
Background setting in this study was conducted at
baseline and 30 at the endpoint after the adding of Bisoprolol
ambulatory clinic in cardiovascular department, Dr
Saiful Anwar General Hospital, Malang. Since
recruited samples were ambulatory patients, many
Normality test for patients quality of life showed that the
counfounding factor may had significant impact on
distribution data met Gaussian distribution (normal
the results. One of the method to minimize the
distribution) so that data analysis should used parametric test
effect of confounding factor to the results was by
for two related samples that is Paired t test.
limiting sample recruitment only to the adherence
Paired t test results showed that the baseline quality of life
questionnaire score were significantly differ from endpoint
Other confounding factors were gender, comorbid
score with P value equal to 0.000 (95% Confidence Interval
condition (history of previous chronic il ness), and
(CI); -18 to -1). Paired t test results for quality of life
age. Thus Chi-Square analysis conducted to
questionnaire score summarized in table 3.
determine whether those factors impact to the
examined variables such as ejection fraction and
Mean of Minessota Living with Heart Failure score at baseline
quality of life. Chi-Square analysis resulted that
and 3rd months comparison by Paired t test was displayed to
demographic data taken from the patients were
equivalent thus no classification based on gender,
comorbid condition, and age were needed in
International Journal of Pharmacy Teaching & Practices 2012, Vol.3, Issue 4, 429-433.
Previous studies (CIBIS I, II, III) demonstrated the improvement
after contraction phase this wil aggravate the left
in morbidity, mortality and length of hospitalization stay in
heart failure patients who were treated with Bisoprolol. While
previous studies did not analyze the role of Bisoprolol to the
EF can be measured by several methods. The best
left ventricular function, this study primarily examined the left
method which used to be a gold standard is Simpson
ventricular function due to ejection fraction and quality of life.
method. This method calculates the left ventricular
This study resulted that there were significantly improvement
volume in the end of diastolic and systolic phase
in left ventricular function which were shown in the increasing
then develope to the formula above. This method
of ejection fraction (P = 0.000) and decreasing score of quality
minimize the operator error in determine the cut
of life questionnaire (P = 0.000). This result probably delivered
point of the left ventricle. This study recruited two
by the reduction of cardiac oxygen demand as a result from
blinded operator to examine the ejection fraction to
the decreasing of heart rate so that ischemic related symptom
improved. Other mechanism of Bisoprolol in improving left
ventricular function was due to the antagonistic effect of
Baseline ejection fraction from the patients then
aldosteron by inhibits renin release so that decreasing in water
compare to themselves ejection fraction after
and sodium retention which bring to the reduction of cardiac
receiving Bisoprolol for three months. Comparison
load and decrease ischemic state9,10,13.
method was by Wilcoxon test since the baseline
ejection fraction showed non Gaussian distribution.
This study conducted a quasi-experimental with one group
As the results showed in table 2 there were
pretest-posttest design to compare the ejection fraction and
increasing of ejection fraction between baseline and
quality of life measurements before and after the adding of
three months after the adding of Bisoprolol in most
Bisoprolol to ACE inhibitor and furosemide combination for
of patients. Wilcoxon test indicated that EF mean
three months at stage C systolic heart failure patients. Before
were significantly difference by 95% confidence of
the adding of Bisoprolol, the patients should had accepted an
interval (P = 0.000). This incline trend may indicated
optimum dose of ACE inhibitor in order to ensure that the
the role of Bisoprolol in increasing left ventricular
improvements of left ventricular function was obtained by the
function by decreasing heart rate and promoting
adding of Bisoprolol to the combination of ACE inhibitor and
adequate fil ing phase in the left ventricle.
furosemide diuretic, since those combination had been proven
to decrease heart failure morbidity and increase left
Heart failure condition has very high impact on the
ventricular ejection fraction based on the research conducted
quality of life and should be examined frequently in
by Simon and Nishio at 2002 and 2008 respectively12,13.
order to predicted the worsening or improving left
Systolic heart failure condition usual y accompanied by left
ventricular function. The level of heart failure impact
ventricular hypertrophy. The left ventricular fil ing wil be
on the quality of life usual y measured by Minessota
disturbed in the left ventricular hypertrophy condition. So that
questionnaire which is contain twenty one questions
the cardiac afterload volume decrease then aggravated by the
each determines the frequencies of symptoms or
reduction of the left ventricular myocyte contraction. All of
the heart failure impact on phsycosocial life. The
this condition bring to the reduction of cardiac output and
more heart failure impact on the quality of life, the
hypoperfusion through al of the body thus change the cel ular
higher score were determined. The avarage of
metabolism in to anaerob metabolism. This anaerob
baseline and endpoint total scores for Minnesota
metabolism will lead to clinical manifestation such as fatigue
Living with Heart Failure questionnaire in patients
due to lactic acid accumulation and this may lead to metabolic
then compared by paired t test analysis since data
acidosis. Left ventricular function has important role in the
clinical manifestation in heart failure condition.
Paired t test analysis showed there were significantly
Ejection fraction describe the left ventricular function by
difference in the score of Minnesota Living with
measuring the fraction of the blood that ejected from the left
Heart Failure questionnaire before and after the
ventricle. Ejection fraction may be derivated by this formula:
adding of Bisoprolol by 95% confidence of interval (P = 0.000). The total score of Minnesota Living with
Heart Failure questionnaire tend to decrease after
the adding of Bisoprolol to ACE inhibitor and
A higher EF value means a higher blood fraction which is
furosemide for three months. This indicated that the
ejected from the left ventricle and by the reversed the lower
routine adding of Bisoprolol to the combination of
EF value means a lower blood fraction which is ejected from
ACE inhibitor and furosemide may improved the
the left ventricle and the worse left ventricular function. The
quality of life in heart failure patients.
reduction of cardiac output volume (EDV – ESV) due to
impairment of the left ventricular ejection induce the
This study limitation was the ignorance of the ACE
increasing of blood volume which is left in the left ventricle
inhibitor and furosemide to the improvement of ejection fraction and quality of life since previous
International Journal of Pharmacy Teaching & Practices 2012, Vol.3, Issue 4, 429-433.
study noted that those combination also improve left
9. Lechat, P., 1994. A Randomized Trial of β-
ventricular function in heart failure. This study also consider
Blockade in Heart Failure: The Cardiac Insufficiency
that dose variation do not take important role in improving left
Bisoprolol Study (CIBIS).Am Heart J. Vol. 90. pp
10. Lechat, P., Hulot, J.S., Escolano, S., Mal et, A.,
Further studies are needed to examine the role of dose
Leizorovics, A., Werhlen-Grandjean, M., Pochmalicki,
variation in heart failure therapy to the left ventricular
G., Dargie, H., 2001. Heart Rate and Cardiac Rhythm
improvement. Better study design such as randomized control
Relationships With Bisoprolol Benefit in Chronic
trial with the bigger sample size is needed to confirm our
Heart Failure in CIBIS II Trial. Am Heart J. Vol. 103.
results. As β-blocker monotherapy is not recommended in
heart failure condition, so that the single effect of β-blocker on
11. Lee, D.S., et. al., 2009. Relation of Disease
the left ventricular function is infeasible to be examined.
Pathogenesis and Risk Factors to Heart Failure With
Preserved or Reduced Ejection Fraction: Insights
Conclusion
From the Framingham Heart Study of the National
Heart, Lung, and Blood Institute. Am Heart J. Vol.
Result of this prospective study showed that the routine
addition of Bisoprolol to ACE inhibitor and furosemide
12. Nishio, M., Sakata, Y., Mano, T., Ohtani, T.,
combination may increase ejection fraction significantly by P =
Takeda, Y., Miwa, T., Hori, M., Masuyama, T., Kondo,
0.000 and 95% confidence of interval. Bisoprolol addition to
T., Yamamoto, K., 2008. Beneficial Effect of
ACE inhibitor and furosemide combination may also improve
Bisoprolol on The survival of Hypertensive Heart
quality of life in systolic heart failure patients significantly (P =
Failure. Eur J of Heart Failure. Vol. 10. pp 446-453
0.000 ; 95% confidence of interval) if measured by Minnesota
13. Simon, T., Mary-Krause, M., Funch-Brentano, C.,
Living with Heart Failure questionnaire.
Lechat, P., Jail on, P., on behalf of CIBIS II
Investigators, 2002. Bisoprolol Dose-Response
Acknowledgement
Relationship in Patients with Congestive Heart Failure: A Subgroup Analysis in The Cardiac
We are grateful to Research Development Unit, Medical
Insufficiency Bisoprolol Study (CIBIS II). Eur Heart J.
Faculty, Brawijaya University, Education Ministry of Indonesia
and Dr Saiful Anwar General Hospital for facilitating this study.
14. Silvestry, F.E., et.al. 2009. Echocardiography-
We also thank Diana Lyrawati, MSi., PhD for her
Guided Interventions. USA: American Society of
encouragement and valuable advice in publishing this
15. Tendera, M., 2004. The Epidemiology of Heart
Failure. J RAA Syst. Vol. 5 (Suppl 1), pp. S2-S6.
References
1. Abraham, W.T., 2000. β-Blockers The New Standar of
Therapy for Mild Heart Failure. Arch Intern Med, Vol. 160, pp. 1237-1247
AUTHORS’ CONTRIBUTIONS
2. Baliga, R.R., Pitt, B., Givertz, M.M., 2008. Management of heart failure. Volume 1: Medical. Springer-Verlag London
Authors contributed equal y to al aspects of the
Limited. P 1-46; 77-128 3. Bristow, M.R., 2000. β-Adrenergic Receptor Blokade in
Chronic Heart Failure. Am Heart J. Vol 101. pp 558-569 4. Feldman, A.M., 2006. Heart Failure: Pharmacologic
PEER REVIEW
Management. Blackwel Publishing. 199-207 5. Fletcher, P., 2000. Beta blocker in heart failure. Aust Prescr.
Not commissioned; external y peer reviewed
6. Hulsmann M, Berger R, Sturm B, et al. Prediction of outcome by neurohumoral activation, the six-minute walk test
CONFLICTS OF INTEREST
and the Minnesota Living with Heart Failure Questionnaire in an outpatient cohort with congestive heart failure. Eur Heart J.
The authors declare that they have no competing
2002; 23: 886-891. 7. Kukin, M.L., 1999. Prospective, Randomized Comparison of
Effect of Long-Term Treatment With Metoprolol or Carvedilol on Symptoms, Exercise, Ejection Fraction, and Oxidative Stress
in Heart Failure. Am Heart J. Vol. 118. pp. 149-157 8. Khan, M.G., 2006. Encyclopedia of Heart Disease. USA: Elsevier Academic Press. P 159-167; 206-209; 313-318; 327-346
Job Fairs July-August, 2013 page 1 What: Chicago Career Fair When: Tuesday, July 23, 2013 11:00 AM —2:00 PM Where: The Congress Plaza Hotel520 South Michigan Ave. Chicago, IL 60605 Positions: Accounting/Auditing, Administrative and Support Services, Advertising/Marketing/Public Relations, Banking, Consumer Products, Customer Service and Call Center, Finance/Economic
Liste des publications scientifiques de Laurent RIVIER 1. L. Rivier et P.E. Pilet (1971) Composés hallucinogènes indoliques naturels. Année Biologique 10 , 129-149. 2. L. Rivier and J.E. Lindgren (1972) Ayahuasca, the south-american hallucinogenicdrink - an ethnobotanical and chemical investigation. Economic Botany 26 , 101-129. 3. L. Rivier and P.E. Pilet (1974) Indolyl-3-acetic
 International Journal of Pharmacy Teaching & Practices 2012, Vol.3, Issue 4, 429-433.
Role of Bisoprolol Adding oo Ace Inhibitor and Fu rosemide Combination on the Left
International Journal of Pharmacy Teaching & Practices 2012, Vol.3, Issue 4, 429-433.
Role of Bisoprolol Adding oo Ace Inhibitor and Fu rosemide Combination on the Left  International Journal of Pharmacy Teaching & Practices 2012, Vol.3, Issue 4, 429-433.
Material and Method
International Journal of Pharmacy Teaching & Practices 2012, Vol.3, Issue 4, 429-433.
Material and Method 
 International Journal of Pharmacy Teaching & Practices 2012, Vol.3, Issue 4, 429-433.
International Journal of Pharmacy Teaching & Practices 2012, Vol.3, Issue 4, 429-433.

 International Journal of Pharmacy Teaching & Practices 2012, Vol.3, Issue 4, 429-433.
Previous studies (CIBIS I, II, III) demonstrated the improvement
after contraction phase this wil aggravate the left
in morbidity, mortality and length of hospitalization stay in
heart failure patients who were treated with Bisoprolol. While
previous studies did not analyze the role of Bisoprolol to the
EF can be measured by several methods. The best
left ventricular function, this study primarily examined the left
method which used to be a gold standard is Simpson
ventricular function due to ejection fraction and quality of life.
method. This method calculates the left ventricular
This study resulted that there were significantly improvement
volume in the end of diastolic and systolic phase
in left ventricular function which were shown in the increasing
then develope to the formula above. This method
of ejection fraction (P = 0.000) and decreasing score of quality
minimize the operator error in determine the cut
of life questionnaire (P = 0.000). This result probably delivered
point of the left ventricle. This study recruited two
by the reduction of cardiac oxygen demand as a result from
blinded operator to examine the ejection fraction to
the decreasing of heart rate so that ischemic related symptom
improved. Other mechanism of Bisoprolol in improving left
ventricular function was due to the antagonistic effect of
Baseline ejection fraction from the patients then
aldosteron by inhibits renin release so that decreasing in water
compare to themselves ejection fraction after
and sodium retention which bring to the reduction of cardiac
receiving Bisoprolol for three months. Comparison
load and decrease ischemic state9,10,13.
method was by Wilcoxon test since the baseline
ejection fraction showed non Gaussian distribution.
This study conducted a quasi-experimental with one group
As the results showed in table 2 there were
pretest-posttest design to compare the ejection fraction and
increasing of ejection fraction between baseline and
quality of life measurements before and after the adding of
three months after the adding of Bisoprolol in most
Bisoprolol to ACE inhibitor and furosemide combination for
of patients. Wilcoxon test indicated that EF mean
three months at stage C systolic heart failure patients. Before
were significantly difference by 95% confidence of
the adding of Bisoprolol, the patients should had accepted an
interval (P = 0.000). This incline trend may indicated
optimum dose of ACE inhibitor in order to ensure that the
the role of Bisoprolol in increasing left ventricular
improvements of left ventricular function was obtained by the
function by decreasing heart rate and promoting
adding of Bisoprolol to the combination of ACE inhibitor and
adequate fil ing phase in the left ventricle.
furosemide diuretic, since those combination had been proven
to decrease heart failure morbidity and increase left
Heart failure condition has very high impact on the
ventricular ejection fraction based on the research conducted
quality of life and should be examined frequently in
by Simon and Nishio at 2002 and 2008 respectively12,13.
order to predicted the worsening or improving left
Systolic heart failure condition usual y accompanied by left
ventricular function. The level of heart failure impact
ventricular hypertrophy. The left ventricular fil ing wil be
on the quality of life usual y measured by Minessota
disturbed in the left ventricular hypertrophy condition. So that
questionnaire which is contain twenty one questions
the cardiac afterload volume decrease then aggravated by the
each determines the frequencies of symptoms or
reduction of the left ventricular myocyte contraction. All of
the heart failure impact on phsycosocial life. The
this condition bring to the reduction of cardiac output and
more heart failure impact on the quality of life, the
hypoperfusion through al of the body thus change the cel ular
higher score were determined. The avarage of
metabolism in to anaerob metabolism. This anaerob
baseline and endpoint total scores for Minnesota
metabolism will lead to clinical manifestation such as fatigue
Living with Heart Failure questionnaire in patients
due to lactic acid accumulation and this may lead to metabolic
then compared by paired t test analysis since data
acidosis. Left ventricular function has important role in the
clinical manifestation in heart failure condition.
Paired t test analysis showed there were significantly
Ejection fraction describe the left ventricular function by
difference in the score of Minnesota Living with
measuring the fraction of the blood that ejected from the left
Heart Failure questionnaire before and after the
ventricle. Ejection fraction may be derivated by this formula:
adding of Bisoprolol by 95% confidence of interval (P = 0.000). The total score of Minnesota Living with
Heart Failure questionnaire tend to decrease after
the adding of Bisoprolol to ACE inhibitor and
A higher EF value means a higher blood fraction which is
furosemide for three months. This indicated that the
ejected from the left ventricle and by the reversed the lower
routine adding of Bisoprolol to the combination of
EF value means a lower blood fraction which is ejected from
ACE inhibitor and furosemide may improved the
the left ventricle and the worse left ventricular function. The
quality of life in heart failure patients.
reduction of cardiac output volume (EDV – ESV) due to
impairment of the left ventricular ejection induce the
This study limitation was the ignorance of the ACE
increasing of blood volume which is left in the left ventricle
inhibitor and furosemide to the improvement of ejection fraction and quality of life since previous
International Journal of Pharmacy Teaching & Practices 2012, Vol.3, Issue 4, 429-433.
Previous studies (CIBIS I, II, III) demonstrated the improvement
after contraction phase this wil aggravate the left
in morbidity, mortality and length of hospitalization stay in
heart failure patients who were treated with Bisoprolol. While
previous studies did not analyze the role of Bisoprolol to the
EF can be measured by several methods. The best
left ventricular function, this study primarily examined the left
method which used to be a gold standard is Simpson
ventricular function due to ejection fraction and quality of life.
method. This method calculates the left ventricular
This study resulted that there were significantly improvement
volume in the end of diastolic and systolic phase
in left ventricular function which were shown in the increasing
then develope to the formula above. This method
of ejection fraction (P = 0.000) and decreasing score of quality
minimize the operator error in determine the cut
of life questionnaire (P = 0.000). This result probably delivered
point of the left ventricle. This study recruited two
by the reduction of cardiac oxygen demand as a result from
blinded operator to examine the ejection fraction to
the decreasing of heart rate so that ischemic related symptom
improved. Other mechanism of Bisoprolol in improving left
ventricular function was due to the antagonistic effect of
Baseline ejection fraction from the patients then
aldosteron by inhibits renin release so that decreasing in water
compare to themselves ejection fraction after
and sodium retention which bring to the reduction of cardiac
receiving Bisoprolol for three months. Comparison
load and decrease ischemic state9,10,13.
method was by Wilcoxon test since the baseline
ejection fraction showed non Gaussian distribution.
This study conducted a quasi-experimental with one group
As the results showed in table 2 there were
pretest-posttest design to compare the ejection fraction and
increasing of ejection fraction between baseline and
quality of life measurements before and after the adding of
three months after the adding of Bisoprolol in most
Bisoprolol to ACE inhibitor and furosemide combination for
of patients. Wilcoxon test indicated that EF mean
three months at stage C systolic heart failure patients. Before
were significantly difference by 95% confidence of
the adding of Bisoprolol, the patients should had accepted an
interval (P = 0.000). This incline trend may indicated
optimum dose of ACE inhibitor in order to ensure that the
the role of Bisoprolol in increasing left ventricular
improvements of left ventricular function was obtained by the
function by decreasing heart rate and promoting
adding of Bisoprolol to the combination of ACE inhibitor and
adequate fil ing phase in the left ventricle.
furosemide diuretic, since those combination had been proven
to decrease heart failure morbidity and increase left
Heart failure condition has very high impact on the
ventricular ejection fraction based on the research conducted
quality of life and should be examined frequently in
by Simon and Nishio at 2002 and 2008 respectively12,13.
order to predicted the worsening or improving left
Systolic heart failure condition usual y accompanied by left
ventricular function. The level of heart failure impact
ventricular hypertrophy. The left ventricular fil ing wil be
on the quality of life usual y measured by Minessota
disturbed in the left ventricular hypertrophy condition. So that
questionnaire which is contain twenty one questions
the cardiac afterload volume decrease then aggravated by the
each determines the frequencies of symptoms or
reduction of the left ventricular myocyte contraction. All of
the heart failure impact on phsycosocial life. The
this condition bring to the reduction of cardiac output and
more heart failure impact on the quality of life, the
hypoperfusion through al of the body thus change the cel ular
higher score were determined. The avarage of
metabolism in to anaerob metabolism. This anaerob
baseline and endpoint total scores for Minnesota
metabolism will lead to clinical manifestation such as fatigue
Living with Heart Failure questionnaire in patients
due to lactic acid accumulation and this may lead to metabolic
then compared by paired t test analysis since data
acidosis. Left ventricular function has important role in the
clinical manifestation in heart failure condition.
Paired t test analysis showed there were significantly
Ejection fraction describe the left ventricular function by
difference in the score of Minnesota Living with
measuring the fraction of the blood that ejected from the left
Heart Failure questionnaire before and after the
ventricle. Ejection fraction may be derivated by this formula:
adding of Bisoprolol by 95% confidence of interval (P = 0.000). The total score of Minnesota Living with
Heart Failure questionnaire tend to decrease after
the adding of Bisoprolol to ACE inhibitor and
A higher EF value means a higher blood fraction which is
furosemide for three months. This indicated that the
ejected from the left ventricle and by the reversed the lower
routine adding of Bisoprolol to the combination of
EF value means a lower blood fraction which is ejected from
ACE inhibitor and furosemide may improved the
the left ventricle and the worse left ventricular function. The
quality of life in heart failure patients.
reduction of cardiac output volume (EDV – ESV) due to
impairment of the left ventricular ejection induce the
This study limitation was the ignorance of the ACE
increasing of blood volume which is left in the left ventricle
inhibitor and furosemide to the improvement of ejection fraction and quality of life since previous
 International Journal of Pharmacy Teaching & Practices 2012, Vol.3, Issue 4, 429-433.
study noted that those combination also improve left
9. Lechat, P., 1994. A Randomized Trial of β-
ventricular function in heart failure. This study also consider
Blockade in Heart Failure: The Cardiac Insufficiency
that dose variation do not take important role in improving left
Bisoprolol Study (CIBIS). Am Heart J. Vol. 90. pp
10. Lechat, P., Hulot, J.S., Escolano, S., Mal et, A.,
Further studies are needed to examine the role of dose
Leizorovics, A., Werhlen-Grandjean, M., Pochmalicki,
variation in heart failure therapy to the left ventricular
G., Dargie, H., 2001. Heart Rate and Cardiac Rhythm
improvement. Better study design such as randomized control
Relationships With Bisoprolol Benefit in Chronic
trial with the bigger sample size is needed to confirm our
Heart Failure in CIBIS II Trial. Am Heart J. Vol. 103.
results. As β-blocker monotherapy is not recommended in
heart failure condition, so that the single effect of β-blocker on
11. Lee, D.S., et. al., 2009. Relation of Disease
the left ventricular function is infeasible to be examined.
Pathogenesis and Risk Factors to Heart Failure With
Preserved or Reduced Ejection Fraction: Insights
Conclusion
International Journal of Pharmacy Teaching & Practices 2012, Vol.3, Issue 4, 429-433.
study noted that those combination also improve left
9. Lechat, P., 1994. A Randomized Trial of β-
ventricular function in heart failure. This study also consider
Blockade in Heart Failure: The Cardiac Insufficiency
that dose variation do not take important role in improving left
Bisoprolol Study (CIBIS). Am Heart J. Vol. 90. pp
10. Lechat, P., Hulot, J.S., Escolano, S., Mal et, A.,
Further studies are needed to examine the role of dose
Leizorovics, A., Werhlen-Grandjean, M., Pochmalicki,
variation in heart failure therapy to the left ventricular
G., Dargie, H., 2001. Heart Rate and Cardiac Rhythm
improvement. Better study design such as randomized control
Relationships With Bisoprolol Benefit in Chronic
trial with the bigger sample size is needed to confirm our
Heart Failure in CIBIS II Trial. Am Heart J. Vol. 103.
results. As β-blocker monotherapy is not recommended in
heart failure condition, so that the single effect of β-blocker on
11. Lee, D.S., et. al., 2009. Relation of Disease
the left ventricular function is infeasible to be examined.
Pathogenesis and Risk Factors to Heart Failure With
Preserved or Reduced Ejection Fraction: Insights
Conclusion