Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Dental analgesics
Dr. Smith will present a review of two important areas of dental pharmacotherapeutics, analgesics and seda-
tives. Besides discussing the basic pharmacology of the most commonly used drugs in these two therapeutic
groups, he will also address the clinical considerations dental practitioners should weigh before treating pa-
tients with these agents, including drug/drug interactions, drug/disease interactions and rational treatment
• Understand the difference in effi cacy between opioid and nonopioid analgesics in treating dental pain.
• Appreciate the difference in mechanism of action between opioid and nonopioid analgesics.
• Become familiar with some less common NSAIDs that can be useful in dental patients with various health
• Be aware of the most signifi cant side effects of dental analgesic groups.
• Understand how the effi cacies of new analgesic drugs is assessed and know how this relates to actual
clinical effi cacy in the dental setting.
• Understand how the compounding of commercial drugs affects their effi cacies and be able to use this
understanding to select the drugs that are best for the dental patient.
• Appreciate the relationship between how the analgesic is taken by the patient and the extent of pain
• Be able to identify the most signifi cant interactions associated with dental analgesics.
• Understand the mechanism of action of the benzodiazepine antianxiety drugs.
• Appreciate the major drawbacks associated with the use of benzodiazepines,
• Identify patients that are poor candidates for the use of benzodiazepines.
• Appreciate the differences in clinical characteristics among the long-acting, intermediate-acting, and
Dr. Smith, recently retired as Professor of Pharmacology in the Department of Integrative Biosciences at the OHSU
School of Dentistry where he taught from 1982 until July of this year. Dr. Smith received his M.S. and Ph.D in phar-
macology/toxicology from Oregon State University and completed a postdoctoral fellowship in neuropharmacol-
ogy at the University of Washington. After two years of teaching at Southern Illinois University’s School of Dentistry
he returned to the west coast to take a position as Senior Researcher at the OSU Marine Science Center. In 1982
he moved to the then Department of Pharmacology and Toxicology at the OHSU School of Dentistry. At the time
of his retirement Dr Smith was the course director for all pharmacology classes offered to dental resident students
and undergraduate dental students at OHSU SD.
PHARMACOLOGY UPDATE Analgesics and Oral Sedatives John R. Smith, Ph.D. November 8, 2013 I. NONOPIOID ANALGESICS
A. NSAIDs Pharmacology
1. Mechanism of action: NSAIDs inhibit the catalytic activity of the enzyme, cyclo-oxygenase (COX),
which converts arachidonic acid to prostaglandins (PGs) … PGs sensitize mechanical and chemical receptors.
a. COX-1 is the constitutive form and provides PGs that are used routinely by the body for
maintenance of normalfunctions (hemostasis, gastric protection, renal function).
b. COX-2 is the inducible form and provides PGs found in traumatized tissues and during inflammation.
a. Flurbiprofen (ANSAID): Not specifically indicated for analgesia (unlabeled indication) … Greater efficacy & longer acting than ibuprofen
b. Ketoprofen (ORUDIS, ORUDIS-KT, ACTRON): Analgesia is a labeled indication… Partial
inhibition of lipoxygenase reported … bit longer acting than ibuprofen … More dyspepsia than ibuprofen
c. Sulindac (CLINORIL): Is a prodrug … “renal sparing” but still use caution in patients with
impaired renal blood flow … 16 hr T½ ⇒ 2-3/day dosing
d. Diclofenac (CATAFLAM): Efficacious as ibuprofen but more pronouncedGI side effects …
Major advantage is lack of accumulation in patients with renal or liver disease
e. Etodolac (LODINE): As efficacious as ibuprofen … producing less GI side effects than other
f. Meloxicam (MOBIC): Similar to etodolac … effective moderate analgesic with less GI effects g. Ketorolac (TORADOL): parenteral form is a strong analgesic; oral = ibuprofen-level pain
relief … parenteral form MUST be given prior to initiating a course of oral administration … maximum treatment course is 5 days. CONTRAINDICATIONS (box warnings):
active or history of peptic ulcer or gastrointestinal bleeding
• before or during any surgery where hemostasis is critical
• suspected or confirmed cerebrovascular bleeding
• epidural or intrathecal administration
• use with aspirin or other NSAID • use with probenecid
3. Selective NSAIDs (COX-2 inhibitors): The Grail wasn't that holy!
a. The HOPE of the "Grail." – Relieve pain without causing G.I. ulceration and hemorrhage or renal failure … based on the concept of "good" and "bad" cyclo-oxygenases
b. Constitutive COX-1 vs Inducible COX-2: Generally true but notable exceptions have arisen and
more anticipated … i.e., COX-1 activity not all good & COX-2 activity not all bad.
B. NSAIDs – Adverse Effects
a. Experienced in predisposed individuals (rarely in kids; 0.3% in general popn; 20-25% in patients
with asthma & nasal polyps).
b. Mechanism is unknown but appears to be related to a shift to the lipoxygenase pathway
It is a CONTRAINDICATION to administer ANY NSAID to a patient who
has ever demonstrated this bronchospastic response to any NSAID.
2. Pregnancy: No well-controlled studies in women … Avoid if possible especially in the 3rd trimester.
a. Category B:
ketoprofen, naproxen, ibuprofen flurbiprofen, diclofenac
b. Category C:
etodolac, ketorolac, mefenamic acid, nabumetone, oxaprozin, tolmetin, bromfenac, piroxicam, rofecoxib, celecoxib
3. Low-dose aspirin patients: To maintain normal antiplatelet aggregating effects of aspirin it should be
taken 1-2 hours prior to any other NSAID.
4. NSAID "withdrawal": small scale, early studies suggest that sudden cessation of NASID's after long term use increases the risk of stroke and M.I. in the first month … low-dose aspirin has also been implicated … may be wise to "ramp down" after long term use. II. OPIODS
A. Opioid pharmacology
1. Mechanism of action: Through stimulation of various receptors, opioid analgesics raise the threshold of pain perception and foster indifference to pain once it is perceived
a. Mu receptors (µ): clinically most significant … associated with analgesia, euphoria, respiratory depression, miosis, GI motility changes
b. Kappa receptors (κ): activation is associated with analgesia (spinal cord level) c. Delta receptors (δ): activation is associated with analgesia and positive reinforcing effects
a. Direct actions in the dorsal horn … decreases pain input to CNS b. Activation of the descending aminergic inhibitory system … the body's endogenous analgesia
c. Peripheral inhibition of primary afferent nociceptors > decreasing or inhibiting action potential propagation > inhibiting the release of excitatory neuropeptides ,e.g., substance P, from damaged nerves.
> active inflammation a prerequisite to see these peripheral effects … PMNs carry opioids. Selected Opioid Analgesics
1. Propoxyphene (DARVON): analgesia = aspirin … “Most dangerous drug in the U.S.,”… FDA
2. Meperidine (DEMEROL): a synthetic agent that is a strong analgesic given parenterally … half as
effective given orally … short duration and antimuscarinic properties … schedule II agent
3. Pentazocine (TALWIN-Nx):ORALLY effective, moderate analgesic … less GI effects than
morphine … Can increase heart rate and blood pressure . avoid use in CV patients … in high doses psychotomimetic effects have been reported … schedule IV drug . TALWIN Nx has far less abuse potential because it contains naloxone, a µ-receptor antagonist
4. Butorphanol (STADOL): •profile of action similar to pentazocine … less psychomimetic side
effects than pentazocine … caution in CV patients … parenteral & nasal spray (STADOL NS) forms only … now a schedule IV drug … short duration (2-3 hrs)
5. Tramadol (ULTRAM):orally effective with similar profile of action to pentazocine … slow onset
of action (1 hr) . not currently a scheduled drug … blocks reuptake of NE and serotonin into nerves … does not induce withdrawal but should not be used in patients with history of opioid addiction … CONTRAINDICATED in patients allergic to an opioid or taking SSRIs 6. Tapentadol (NUCYNTA): similar to tramadol … FDA Schedule II. Opioid Adverse Effects
a. The medullary respiration center of the brain is EXQUISITELY sensitive to the effects of
b. Apnea: The hypoxicdrive to respiration is resistant to morphine effects … O2 via positive pressure should respiration fail. > CONTRAINDICATED in patients suffering from C.O.P.D. & recent head injury
a. Nausea & Emesis: very predictable! b. Constipation: Propulsive waves in small and large intestine decrease … Nonpropulsive waves
in small and large intestine increase … The anal and pyloric sphinctersincrease tone
c. delay in stomach opening time too … interferes with drug absorption
3. Opioid Allergy: good histamine releasers … mimics allergic reaction … few true allergies
4. Opioid "resistance": Some patients receive little relief from codeine & hydrocodone … they are prodrugs … CYP2D6 produces the active metabolites a. genetic cause … poor CYP2D6 activity b. synthetics may be better (tramadol, pentazocine) … oxycodone does not need activation c. some drugs inhibit CYP2D6 activity … may interfere with some opioid analgesia … SSRIs, Trends in opioid analgesia
1. Peripherally acting κ-receptor agonists … avoids central side effects. 2. Peripherally acting µ-receptorantanogists … leaves central analgesia intact … methylnaltrexone III. DENTAL ANALGESIC THERAPY
1. Therapeutic goal: To obtund pain to where the patient can perform routine tasks … pain is a reminder
2. Ceiling analgesic effect: highest degree of pain relief achievable by an agent … maximum efficacy
… can compare efficacies with the dental pain model = extraction of impacted 3rd molars
3. Ceiling analgesic dose: The smallest dose of a drug that can produce its ceilinganalgesic effect. NONOPIOID ANALGESICS OPIOID ANALGESICS
a 60 mg of codeine is an arbitrary CAD because even though the true CAD is 120mg few patients
will tolerate the side effects associated with doses > 60 mg
b Clinically recognized CADs based upon true ceiling efficacy or reasonable patient compliance.
B. Factors influencing the choice of analgesic
1. The Level of Pain: By using your clinical judgement you must estimate the pain level that will
result in this paticular patient from the procedure to be performed.
The principle to be applied is that you want to choose a product that will achieve just the appro- priate level of pain control through the delivery of a CAD in the maximum doserecommended
2. Compounding:
a. WARNING: Not all products will contain the CAD of the active ingredient(s) in the dosage regimen indicated on the package insert. FULL STRENGTH LESS EFFECTIVE PRODUCTSa COUNTERPARTS LORTAB 2.5/500 5mg hydrocodone + 500mg acetaminophenb 2.5mg hydrocodone + 500mg acetaminophen MARGESIC #3 TYLENOL #3 30mg codeine + 650mg acetaminophen 30mg codeine + 300mg acetaminophen PERCOCET 5mg oxycodone + 500mg acetaminophen 5mg oxycodone + 325mg acetaminophen
a The component in combination products that provides the bulk of the analgesia in situations of dental pain is the NONOPIOID agent.
b FDA … in one year no combo product will be able to contain more than 350mg of acetaminophen
• ULTRACET: 37.5mg tramadol + 325mg acetaminophen … recommended dose: 2 qid
• COMBUNOX: 400mg ibuprofen + 5mg oxycodone … 1 tab ~ 2 VICODIN
• REPREXAIN: 200mg ibuprofen + 5mg hydrocodone
c. NSAID + Acetaminophen combinations: additive effects have been theorized . different Recommendation: 600 mg ibuprofen + 1000 mg acetaminophen q6h . do not exceed 2400 mg ibuprofen or 4000 mg acetaminophen/day
C. Considerations involving analgesic regimens
a. WHEN? In situations where the treatment plan involves surgical techniques that will lead to
considerable tissue trauma, eg, oral surgery, endo.
b. RATIONALE: By blocking COX before trauma occurs less prostaglandins will be produced
which will limit nociceptor sensitization and therefore DELAY onset of postoperative pain & REDUCE the magnitude of the pain.
2. Rigid dosing schedule vs PRN dosing:
a. For the first 24 hours after treatment the patient should be put on a rigid dosing schedule that
should startbefore the local anesthetic has a chance to wear off.
b. RATIONALE:first 24 hours is the time of most intense pain . by keeping the pain well
controlled in this period less discomfort will occur in the subsequent days.
3. Long-acting local anesthetics: In situations where there has been considerable tissue trauma a long-
acting local anesthetic can reduce the amount of postoperative analgesics needed by inhibiting nociceptive sensitization in the first few hours of recovery.
4. Total dose: In general, after 2 days most postoperative treatment can be handled adequately with
D. Relative efficacies of dental analgesics.
1. Systematic review of randomized, double-blind, single dose studies indicates that ibuprofen (600 –
800mg) would appear to be the drug of choice … Barden, et al., BDJ, 197(7): 407 (2004)
2. Diclofenac (100mg) performs comparably with ibuprofen 3. 800mg ibuprofen shows better mean pain relief than 600mg of but confidence intervals overlap.
1. Antihypertensives: Just 3 classes to worry about .
angiotensin converting enzyme inhibitors beta-blockers diuretics
These drugs rely upon renal prostaglandin (Pg) mechanisms for their therapeutic effects
a. ACEIs: secondary antihypertensive mechanism = increase in bradykinin ⇒ ⇑ Pgs ⇒ ⇑ renal
perfusion ⇒ ⇓ blood pressure . NSAIDs will block Pg production.
b. Beta-blockers: high doses ⇑ prostacyclin synthesis ⇒ vasodilation & NSAIDs will block this
c. Diuretics: act by facilitating secretion of Na+ and H2O . NSAIDs ⇒ ⇑ Na+ absorption
2. Anticoagulants: Typical NSAIDs will increase the hemorrhage potential of warfarin
(COUMADIN®) and ticlodipine (TICLID®) .
a. Mechanism: (1) displace from plasma proteins; (2) inhibit production of thromboxane A2; (3)
b. Aspirin is CONTRAINDICATED . use others with caution
c. COX-2 inhibitors may not be much better with long term use . acute use probably OK
d. Elderly are at particular risk . less plasma proteins
e. Acetaminophen has been reported to increase the INR in warfarin patients . conflicting
3. Methotrexate (RHEUMATREX®): NSAIDs ⇓ renal clearance of methotrexate ⇒ kidney damage
. significant with high dose methotrexate (CONTRAINDICATED)
4. Oral hypoglycemics: Aspirin (not other NSAIDs) will displace O.H.s from plasma binding sites
a. Gastric irritation of ethanol enhances the hemorrhage potential of NSAIDs b. acetaminophen: In patients that consume alcohol on a regular basis acetaminophen is safe as
long as they CONTINUE TO CONSUME alcohol while taking acetaminophen
· 5% of acetaminophen is converted to a highly reactive toxin by CYP2E1 · ethanol induces CYP2E1 which also metabolizes ethanol · ethanol and acetaminophen compete as enzyme substrates · without ethanol there is an increase in acetaminophen conversion to its toxic metabolite
6. Alendronate (FOSAMAX), etc: NSAIDs can exacerbate gastrointestinal irritations of these agents
1. Monoamine oxidase inhibitors (MAOIs):
a. Meperidine is CONTRAINDICATED . other procarbazine (MATULANE)
b. CNS depression, agitation, hypertension,
c. Not reversed by naloxone . possibly a toxic secondary metabolite of meperidine.
2. Selective Serotonin Reuptake Inhibitors (SSRIs): Opioids have been associated with risk of
“serotonin syndrome”, i.e., hypertension, agitation, seizure. . avoid this combination
fluoxetine (PROZAC) . paroxetine (PAXIL) . sertraline (ZOLOFT)
fluvoxamine (LUVOX) . citalopram (CELEXA) . escitalopram (LEXAPRO)
ANTIANXIETY AGENTS (anxiolytics) BENZODIAZEPINES
A. Pharmacodynamics: Prototype = diazepam (VALIUM); still a frequently used agent in dentistry to
manage the dentalphobic patient.
When diazepam binds to its specific receptors it initiates a series of
events that facilitates the actions of the inhibitory neurotransmitter, gama-aminobutyric acid (GABA).
a. The GABA receptors are linked to chloride channels and occupation by GABA causes an
opening of the channels → a passive influx of Cl- → cellular hyperpolarization.
b. The GABA receptor oscillates between a high affinity and low affinity states.
c. The benzodiazepine receptor (BenzR) is a binding site located on one of the proteins that
make up the GABA-receptor/Cl- channel complex.
d. When diazepam occupies the BenzR it locks the GABA-receptor into a high affinity state.
Thus with diazepam present there are more high affinity GABA-receptors available and thus
the probability of GABA stimulation ↑→↑ inhibition of the CNS.
2. Given the proper dose of diazepam an anxious patient should become calm and have little
appearance of being sedated (sleepy). This separation of calming from sedation is not as distinct with many of the other benzodiazepines. Diazepam is the drug of choice when dealing with an EXTREMELY dentalphobic patient.
1. Absorption: Diazepam is very lipid soluble and thus is absorbed from the small intestine very rapidly . Peak blood levels will occur in 1 hr. with significant calming earlier.
2. Distribution: It crosses the BBB quite readily however only about 1% of the drug in the blood is
in its free form . other benzodiazepines do not bind as tenaciously to plasma proteins as diazepam.
3. Metabolism: One of the MAJOR DRAWBACKS to the use of diazepam is its prolonged duration of action that is due to the;
a. EXTREMELY long T2 of the parent comp. (24-48 hrs.) . undergoes enterohepatic cycling
b. long T2 of its pharmacologically activemetabolites.
1. Sedation and ataxia: The MOST frequently reported side effects of diazepam. All patients
should be accompanied to and from the dental appointment if any benzodiazepine is to be used. They should also restrict their activity for at least 24 hours due to subtle impairments of judgment and motor control. Children and the elderly are particularly susceptible!
2. Respiratory depression: This can occur in an overdose situation but is highly unlikely in a
dental setting due to the extremely wide margin of safety of diazepam and the other benzodiazepines . therapeutic dose = 2-10mg vs toxic dose = 700mg . toxicity is “self- limiting” since there is only a limited supply of endogenous GABA & diazepam has no direct effects.
a. Flumazenil (ROMAZICON7) can be used to reverse benzodiazepine-induced respiratory
depression (1-5mg, IV over 2-10 min.) . It is a specific competitive pharmacological antagonist for benzodiazepines.
3. Paradoxical Excitement: This is an infrequent response seen in predisposed individuals. It
can manifest itself through a wide variety of forms (hostility, garrulousness, agitation, hysteria, nightmares, etc.). This reaction unpredictable but can be reversed with flumazanil (ROMAZICON7) administered as indicated for an overdose.
4. Teratogenesis: The use of diazepam in the first trimester has been reported to be associated with
the development of cleft palate. Diazepam is classified as a Pregnancy Category D drug. FDA Category D: Positive evidence of human fetal risk exists, but
benefits in certain situations (e.g. life-threatening situations or diseases
for which safer drugs cannot be used or are ineffective) may make use
of the drug acceptable despite its risks.
AVOID USE IN WOMEN OF CHILDBEARING AGE!!
1. Narrow angle glaucoma: Diazepam is CONTRAINDICATED for patients with this problem.
Its antimuscarinic actions can lead to dilation of the pupil with blockade of the Canals of Schlem . pain and detached retina are possible .
2. Severe liver disease (cirrhosis, etc.): This can greatly prolong the metabolism of diazepam and
its metabolites which can lead to a significant increase in the magnitude and DURATION of action of diazepam. Benzodiazepines that are directly glucuronidated would be safer.
1. Intermediate-acting agents: These agents have T2's of 6- Oxazepam (SERAX7)
a. They have shorter durations of action than diazepam
and show little "hangover" effects.
b. They have no intermediate metabolites but are directly glucuronidated so they are less sensitive to changes in liver function.
c. Same contraindications as diazepam . category D drugs too.
2. Short-acting agents: These agents have T2's <6 hrs
a. The shortest acting of the benzodiazepines. Recovery is
rapid but patients still must be accompanied to and from the office.
b. They have active metabolites but these are so rapidly metabolized by glucuronidation that no
c. Midazolam comes in injectible form and also now in an oral form which is esp. useful in
oral dose for children = 0.5mg/kg
measure out the midazolam yourself and administer to the child in the office . do not let the parent do it at home
use a specific measuring device for dosing . NOT a teaspoon NEVER readminister if effects are not acceptable . oral absorption is very unpredictable and it is difficult to estimate time to peak effect.
Nuclear Bailout: The Costs and Consequences of Renovating the U.S. Nuclear Weapons Complex Executive Summary Despite President Obama’s recent pledge to seek a world free of nuclear weapons, the Department of Energy’s National Nuclear Security Administration (NNSA) is proposing a major upgrade to the nation’s nuclear weapons complex. • If the United States invests in a state-of
Vorhofflimmern Arbeitsgruppe Herzschrittmacher und Elektrophysiologie der SGK Vorhofflimmern (VHF) ist die häufigste supraventrikuläre Rhythmusstörung und kann paroxysmal oder chronisch auftreten. Insbesondere ist die Diagnose des chronischen VHF einfach und kann meist bereits klinisch anhand des absolut arrhythmischen Pulses und des peripheren Pulsdefizites vermutet werden. Elekt
 Dr. Smith will present a review of two important areas of dental pharmacotherapeutics, analgesics and seda-
tives. Besides discussing the basic pharmacology of the most commonly used drugs in these two therapeutic
groups, he will also address the clinical considerations dental practitioners should weigh before treating pa-
tients with these agents, including drug/drug interactions, drug/disease interactions and rational treatment
• Understand the difference in effi cacy between opioid and nonopioid analgesics in treating dental pain.
Dr. Smith will present a review of two important areas of dental pharmacotherapeutics, analgesics and seda-
tives. Besides discussing the basic pharmacology of the most commonly used drugs in these two therapeutic
groups, he will also address the clinical considerations dental practitioners should weigh before treating pa-
tients with these agents, including drug/drug interactions, drug/disease interactions and rational treatment
• Understand the difference in effi cacy between opioid and nonopioid analgesics in treating dental pain.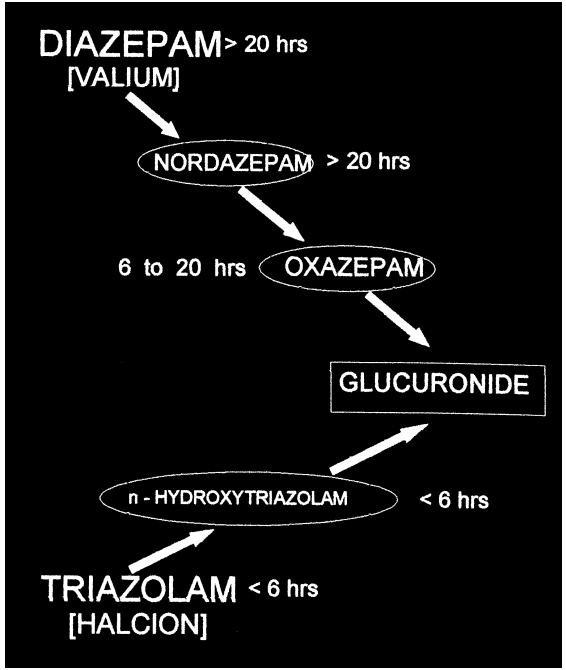 distinct with many of the other benzodiazepines. Diazepam is the drug of choice when dealing
distinct with many of the other benzodiazepines. Diazepam is the drug of choice when dealing