Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Leviatan.ifisiol.unam.mx
Am J Physiol Endocrinol Metab 282: E1154–E1162, 2002. First published January 2, 2002; 10.1152/ajpendo.00470.2001.
Effect of IGF-I therapy on VLDL apolipoprotein B100metabolism in type 1 diabetes mellitus
EMANUEL R. CHRIST,1 PAUL V. CARROLL,2 ELAINE ALBANY,2A. MARGOT UMPLEBY,2 PETER J. LUMB,3 ANTHONY S. WIERZBICKI,3PETER H. SO
1Department of Endocrinology and Diabetology of the Adult, University Hospital of Bern,Inselspital, CH-3010 Bern, Switzerland; and Departments of 2Medicine and 3Chemical Pathology,King’s College London, St. Thomas’ Hospital Campus, London SE1 7EH, United Kingdom
Received 18 October 2001; accepted in final form 17 December 2001
Christ, Emanuel R., Paul V. Carroll, Elaine Albany,
ute to the observed excess cardiovascular risk. Usually,
A. Margot Umpleby, Peter J. Lumb, Anthony S. Wier-
the lipid profiles in well-controlled patients with type 1
zbicki, Peter H. So ¨ nksen, and David L. Russell-Jones.
diabetes mellitus are similar to those seen in matched,
Effect of IGF-I therapy on VLDL apolipoprotein B100 metab-
healthy control subjects (17). Poor diabetic control,
olism in type 1 diabetes mellitus. Am J Physiol Endocrinol
however, is often associated with an increase in total
Metab 282: E1154–E1162, 2002. First published January 2,
cholesterol, triglycerides, and a decrease in high-den-
2002; 10.1152/ajpendo.00470.2001.—Abnormal lipid metab-olism may be related to the increased cardiovascular risk in
sity lipoprotein (HDL)-cholesterol (C; see Ref. 17).
type 1 diabetes. Secretion and clearance rates of very low
Important determinants of the lipid profile are the
density lipoprotein (VLDL) apolipoprotein B100 (apoB) de-
secretion and clearance rates of the apolipoprotein 100
termine plasma lipid concentrations. Type 1 diabetes is char-
(apoB)-containing lipoproteins [very low density li-
acterized by increased growth hormone (GH) secretion and
poprotein (VLDL), intermediate density lipoprotein
decreased insulin-like growth factor (IGF) I concentrations.
(IDL), low density lipoprotein (LDL); see Ref. 36]. Be-
High-dose IGF-I therapy improves the lipid profile in type 1
cause VLDL apoB is the precursor of IDL and LDL,
diabetes. This study examined the effect of low-dose (40
plasma lipid concentrations are dependent on VLDL
g⅐kgϪ1⅐dayϪ1) IGF-I therapy on VLDL apoB metabolism,
apoB metabolism (36). Hepatic overproduction of
VLDL composition, and the GH-IGF-I axis during euglyce-
VLDL apoB has been demonstrated in type 2 diabetes
mia in type 1 diabetes. Using a stable isotope technique,
mellitus and in several hyperlipidemic conditions as-
VLDL apoB kinetics were estimated before and after 1 wk of
sociated with premature atherosclerosis (14, 15, 29,
IGF-I therapy in 12 patients with type 1 diabetes in adouble-blind, placebo-controlled trial. Fasting plasma triglyc-
30). VLDL apoB is constitutively expressed (20), and
eride (P Ͻ 0.03), VLDL-triglyceride concentrations (P Ͻ
VLDL apoB secretion is essentially regulated by intra-
0.05), and the VLDL-triglyceride-to-VLDL apoB ratio (P Ͻ
hepatic lipid substrate availability (triglycerides and
0.002) significantly decreased after IGF-I therapy, whereas
cholesterol esters; see Ref. 40), whereas VLDL apoB
VLDL apoB kinetics were not significantly affected by IGF-I
clearance depends on a complex interaction between an
therapy. IGF-I therapy resulted in a significant increase in
enzyme (lipoprotein lipase) and receptors (LDL recep-
IGF-I and a significant reduction in GH concentrations. The
tors; see Ref. 36). Insulin-like growth factor I (IGF-I) is
mean overnight insulin concentrations during euglycemia
known to promote lipid oxidation (25), which may lead
decreased by 25% after IGF-I therapy. These results indicate
to a decrease in hepatic lipid supply and consequently
that low-dose IGF-I therapy restores the GH-IGF-I axis in
to a reduced VLDL apoB secretion. By increasing in-
type 1 diabetes. IGF-I therapy changes fasting triglyceride
sulin sensitivity, IGF-I may increase lipoprotein lipase
concentrations and VLDL composition probably because of
activity and therefore VLDL apoB clearance (46). In
contrast, VLDL remnant clearance is unlikely to be
type 1 diabetes mellitus; insulin-like growth factor I; growth
influenced by IGF-I, since studies in rats suggest that
hormone secretion; very low density lipoprotein apolipopro-
IGF-I does not significantly affect hepatic expression of
tein B turnover study; stable isotope technique
LDL receptor (3), although growth hormone (GH) hasbeen shown to upregulate hepatic LDL receptors inhumans (39).
TYPE 1 DIABETES MELLITUS is associated with an increased
The GH-IGF-I axis is disordered in type 1 diabetes,
risk of atherosclerosis (31). Although type 1 diabetes
resulting in low levels of IGF-I and, consequently,
appears to be an independent risk factor for cardiovas-
decreased feedback in GH hypersecretion (2). The ele-
cular disease, abnormalities in lipoprotein metabolism
vated GH concentrations, in particular at night, are
(17) and lipoprotein composition (26, 42) may contrib-
The costs of publication of this article were defrayed in part by the
Address for reprint requests and other correspondence: E. Christ,
payment of page charges. The article must therefore be hereby
Dept. of Endocrinology and Diabetology of the Adult, Inselspital,
marked ‘‘advertisement’’ in accordance with 18 U.S.C. Section 1734
CH-3010 Bern, Switzerland (E-mail: Emanuel.Christ@insel.ch).
0193-1849/02 $5.00 Copyright 2002 the American Physiological Society
thought to contribute to the reduced insulin sensitivity
UK) and were injected with 40 g ⅐ kgϪ1 ⅐ dayϪ1 IGF-I/placebo
(16) and have been associated with diabetic microvas-
subcutaneously at night (10:00 P.M.) for seven consecutive
cular complications (18). Exogenous IGF-I administra-
tion has been shown to decrease GH concentrations in
Identical metabolic investigations were performed before
adolescents (1, 4, 10, 44) and in adults (9) with type 1
(study 1) and after (study 2) 1 wk of IGF-I/placebo treatment. On each occasion, all long-acting insulin had been discontin-
diabetes and to improve insulin sensitivity (1, 4, 9, 10,
ued at least 16 h before admission. Empirically with the first
44). Furthermore, IGF-I treatment results in a de-
dose of IGF-I/placebo, the usual dose of evening isophane
crease in fasting triglycerides, total cholesterol, and
(NPH) insulin was decreased by 50%. The patients remained
LDL-C concentrations in patients with type 1 diabetes
in daily contact with the investigators, and the insulin doses
(9). The mechanism, however, remains unknown.
were adjusted on a daily basis according to blood glucose
Using a stable isotope technique, we aimed, there-
fore, to investigate overnight VLDL apoB kinetics dur-
On the days of study, the subjects were admitted to the
ing euglycemic conditions in 12 patients with type 1
metabolic ward at 7:00 PM, having last eaten a snack at 3:00
diabetes before and after 1 wk of IGF-I treatment in a
PM. They were studied in a semirecumbent position and
randomized, double-blind, placebo-controlled trial. In
were allowed to drink water. An indwelling cannula was
addition, VLDL composition, the overnight GH secre-
placed in a superficial vein of the antecubital fossa for ad-ministration of infusions (isotope tracer and insulin), and
tion profile, and insulin concentrations were assessed
another venous cannula was placed in the contralateral arm
to determine the relationship between these variables
for blood sampling. Insulin infusion was started at 7:30 PM,
and euglycemia was obtained by 10:00 PM.
At 10:00 PM, baseline blood samples were taken to mea-
sure isotope background enrichment and hemoglobin A1C. Experimental subjects. Twelve adult patients with type 1
[1-13C]leucine (15 mg/ml, 13C enrichment 99%; Tracer Tech-
diabetes mellitus participated in the study. Their clinical and
nologies, Somerville, MA) was administered as a primed
metabolic characteristics are summarized in Table 1. All
(1 mg/kg) constant infusion (1 mg ⅐ kgϪ1 ⅐ hϪ1) for 10 h. Blood
patients had stable metabolic control and were on subcuta-
glucose concentrations were measured every 15–30 min
neous soluble and isophane insulin. The patients were in
throughout the night, and insulin infusion was adapted to
good general health without evidence of diabetic complica-
maintain glucose concentrations between 5 and 7 mmol/l.
tions and had normal thyroid, renal, and hepatic function. All
EDTA-plasma (5 ml) samples were collected for VLDL apoB
of the patients had a C-peptide concentration of Ͻ0.3 nmol/l,
enrichment at baseline, at 30-min intervals for 2 h, and
and the female patients were taking the combined oral con-
hourly thereafter. Lithium heparin samples (5 ml) were
traceptive pill. St. Thomas’ Hospital Ethics Committee ap-
taken at baseline and after 0.5, 1, 2, 4, and 10 h to determine
proved the study, and all patients provided informed written
13C enrichment of ␣-ketoisocaproate (␣-KIC), the deaminated
consent. The effects of IGF-I therapy on glucose and pro-
product of leucine that provides a measure of intracellular
tein metabolism in these patients have been reported previ-
leucine enrichment (33). At baseline and after 2, 4, 6, 8, and
10 h of infusion, 10-ml EDTA-plasma samples were collected
Study protocol. The study was randomized, double blind,
to determine free fatty acids (FFA), VLDL-triglycerides
and placebo controlled. Patients were instructed in self-ad-
(VLDL-TG), VLDL-C, and VLDL apoB concentrations. GH
ministration of IGF-I (Pharmacia & Upjohn, Milton-Keynes,
concentrations were measured every 30 min from 10:00 PM
Table 1. Clinical characteristics of patients with type 1 diabetes mellitus
BMI, body mass index; apo, apolipoprotein; F, female; M, male; IGF-I, insulin-like growth factor I. Unpaired t-testing and 2 analysis (*)
were used to compare clinical characteristics of the patients in the placebo and the IGF-I groups. AJP-Endocrinol Metab • VOL 282 • MAY 2002 • www.ajpendo.org
until 7:30 AM, and insulin, IGF-binding protein-1 (IGFBP-1),
the equation of Friedewald et al. (19). HbA1C was measured
and IGF-binding protein-3 (IGFBP-3) concentrations were
by anion exchange liquid chromatography (interassay CV
determined at baseline and two times hourly thereafter. At
8%; Primus). GH was measured by an in-house double-anti-
8:00 AM the next morning, 10-ml EDTA-plasma samples
body RIA with a detection limit of 0.3 mU/l. Intra-assay CV
were collected for measurement of total cholesterol, triglyc-
was 10, 4, and 5.4% at 1.7, 12.1 and 22.2 mU/l, respectively.
erides, apolipoprotein E phenotype, and HDL-C, and 5 ml of
Serum IGF-I concentrations were measured by a double-
serum were collected for measurement of total IGF-I concen-
antibody RIA after an ethanol/hydrochloric acid extraction
(intra-assay CV 6%; see Ref. 43). Plasma immunoreactive
Body composition. Body weight was measured on an elec-
insulin concentration was determined by double-antibody
tronic balance with subjects wearing light clothes and without
RIA (interassay CV 6%; see Ref. 41). An immunoradiometric
shoes at the beginning of each study. Height was assessed by a
assay was used for the measurement of IGFBP-1 and
stadiometer. Bioelectrical impedance analysis was measured in
IGFBP-3 [IRMA (Diagnostics Systems Laboratories); inter-
the erect position after voiding using a TBF-105 body fat ana-
assay CV for IGFBP-1 was 5%; interassay CV for IGFBP-3
lyzer (Tanita, Chicago, IL). Fat mass and lean body mass were
was 1%]. Plasma FFA concentrations were measured enzy-
calculated using a preprogrammed equation based on densito-
matically [FFA kit (Wako Chemicals); interassay CV 3.6%].
metric data in a healthy population (6).
The apoE phenotype was determined by Western blotting
Isolation and measurement of isotopic enrichment of VLDL
after isoelectric focusing on a Pharmacia Phast system (Am-
apoB. All EDTA-plasma samples were stored at 4°C and
ersham-Pharmacia, Beaconsfield, UK; see Ref. 34).
analyzed within 24 h of collection. A 2-ml aliquot of plasma
Calculation of VLDL apoB secretion and clearance rates.
was overlaid with 3 ml of sodium chloride density solution
VLDL apoB enrichment with [13C]leucine and [13C]KIC en-
(1.006 kg/l) and ultracentrifuged for 16 h at 147,000 g (Cen-
richment (precursor pool) was calculated using the following
trikon T-2070 ultracentrifuge; Kontron Instruments, Zurich,
formula (12): Et ϭ [Rt Ϫ R0/(1 ϩ Rt Ϫ R0)] ϫ 100, where Rt is
Switzerland). The supernatant containing VLDL was iso-
the 13C-to-12C ratio at time t and R0 is the 13C-to-12C ratio at
lated by aspiration. ApoB was precipitated by the tetra-
baseline before tracer infusion. Fractional catabolic rate
methylurea method, which is highly specific (specificity 97%)
(FCR) and fractional secretion rate (FSR) of VLDL were
for apoB (15). The precipitate was delipidated by incubation
estimated by a multicompartmental model with an intrahe-
with 3 ml ether-ethanol solution (1:3, vol/vol) at Ϫ20°C for
patic delay function by use of SAMM II software (SAMM,
12 h. After recentrifugation (2,000 revolutions/min, 30 min,
Seattle, WA). The precursor compartment for the incorpora-
4°C), the supernatant was removed by aspiration. The delipi-
tion of [13C]leucine into the VLDL particles (forcing function)
dated apoB precipitate was dried under oxygen-free nitrogen
was the steady-state tracer-to-tracee ratio of ␣-KIC. FSR of
(OFN; BOC, Guildford, UK) for 20 min at 25°C and then
VLDL is subject to an intrahepatic delay. The catabolic rate
hydrolyzed in 2 ml of 6 M hydrochloric acid. The samples
of VLDL apoB from plasma is expressed as FCR. Throughout
were heated for 24 h at 115°C to ensure complete hydrolysis
the study, the patients were in steady state, as shown by
and reconstituted in 0.5 ml of 50% acetic acid. Amino acids
constant VLDL apoB concentrations (data not shown). In this
were eluted by cation-exchange chromatography [70 m fil-
case, FSR equals FCR. The model parameters (intrahepatic
ter plastic columns (Bioconnections, Leeds, UK) and Hϩ form
delay and FCR) were estimated from the tracer-to-tracee
cation-exchange resin (Bio-Rad, Richmond, VA)] using 2 ml
ratio of VLDL apoB. A total of 13 time points over the 10-h
of 3 M ammonia. The eluted amino acids were frozen
tracer infusion was included in the mathematical analysis.
(Ϫ70°C), lyophilized, and then stored at Ϫ20°C until deriva-
The absolute VLDL apoB secretion rate was calculated as
tization. The samples were derivatized using 100 l acetoni-
the product of FCR and the VLDL apoB pool size divided by
trile and 100 l N-(tert-butyldimethylsilyl)-N-methyltriflu-
body weight. Pool size was determined as the product of
oroacetamide (Aldrich, Dorset, UK) to form the bis(tert-
plasma volume and VLDL apoB concentration (mean of 6
butyldimethylsilyl) derivative. Excess reagent was removed
samples taken during the study). The plasma volume was
by blowing down under OFN, and the sample was reconsti-
derived as 4.5% of body weight (22), and metabolic clearance
tuted in 100 l decane for gas chromatography-mass spec-
rate was calculated as the product of FCR and plasma
trometry. Isotopic enrichment was determined by selected
ion monitoring of fragments with a mass-to-charge ratio
Statistical analyses. Results are expressed as means Ϯ SE.
(m/z) of 303 and 302 by use of a gas chromatograph-mass
Skewed variables (plasma total and VLDL-TG concentra-
spectrometer (VG Biotech TRIO-2; VG Biotech) in the elec-
tions) were examined after log transformation. Baseline
tron impact ionization mode. The quinoxalinol-tert-butyldim-
characteristics between the placebo and the IGF-I groups
ethylsilyl derivative of ␣-KIC was prepared, and isotope
were compared using unpaired t-testing and, where appro-
enrichment was determined by selected ion monitoring of
priate, 2-analysis. The responses of each parameter (⌬ val-
fragments at m/z 259 and 260 (GC-MS analysis; Hewlett
ues) in the placebo and the IGF-I groups were analyzed for
Packard 5890A, Bracknell, UK). Analytical precision of the
between-group comparison using unpaired t-testing or,
method [coefficient of variation (CV)] has been shown to be
where appropriate, nonparametric testing (kinetic data). For
Ͻ8% for isotopic enrichment (E) of leucine and ␣-KIC (15).
analysis of data from more than two time points, ANOVA
Quantification of VLDL apoB and other analytes. Glucose
was performed. Analysis of GH secretion was performed
concentrations were measured using the glucose oxidase
using Pulsar analysis (9) with nonparametric testing for
method (glucose analyzer, YSI model 23AM; Yellow Springs
comparisons of variables. P values Ͻ0.05 were considered
Instruments). VLDL apoB concentration was determined us-
ing the Lowry method (13). Plasma total cholesterol andtriglyceride concentrations were measured by an enzymatic
method (Boehringer-Mannheim, Mannheim, Germany) usinga Cobas Fara II analyzer (Roche, Welwyn Garden City, UK). Patients. The clinical and metabolic characteristics
HDL-C was separated by precipitation of apoB-containing
were similar in the placebo and IGF-I groups. All
lipoproteins with dextran sulfate/magnesium chloride and
subjects did not experience any side effects during the
measured enzymatically. LDL-C was calculated according to
study period except subject 9 (randomized to placebo),
AJP-Endocrinol Metab • VOL 282 • MAY 2002 • www.ajpendo.org
who had a hypoglycemic episode the day after study 1.
and VLDL-TG-to-VLDL-apoB ratios (P Ͻ 0.002),
Total body weight and body composition did not change
whereas no significant changes were observed after
placebo treatment. The reduction in nonesterified free
Mean overnight glucose concentrations were similar
fatty acid (NEFA) concentrations after IGF-I therapy
in both groups on both occasions (IGF-I group 5.4 Ϯ 0.1
did not reach statistical significance (P ϭ 0.09; Tables
vs. 5.6 Ϯ 0.1 mmol/l, pre- vs. posttreatment, ANOVA
P ϭ 0.49; placebo group 6.3 Ϯ 0.3 vs. 6.5 Ϯ 0.2 mmol/l,
Kinetic characteristic of VLDL apoB metabolism. As
pre- vs. posttreatment, ANOVA P ϭ 0.25). In the IGF-I
shown in Figs. 1 and 2, apoB kinetics were in steady
group, one patient was heterozygous for apoE2 and one
state, since VLDL apoB concentrations did not show a
for apoE4. In the placebo group, two patients were
significant change at the selected time points through-
heterozygous for apoE2 and two for apoE4. The re-
out the study. Precursor pool enrichment as measured
maining patients presented the phenotype apoE3/E3
by ␣-[13C]KIC remained constant throughout the study
periods (Fig. 1, A and B). Because of technical problems
IGF-I and insulin concentrations. Pretreatment se-
(insufficient enrichment of VLDL apoB), we were not
rum IGF-I concentrations were similar in the two
able to include turnover data of subjects 4 (placebo
groups. IGF-I therapy led to a significant rise in circu-
group) and 12 (IGF-I group). The calculated values of
lating IGF-I within the normal range, whereas there
all the kinetic measurements were not statistically
were no changes in the placebo group (IGF-I group
different between the groups before treatment. After
28.2 Ϯ 2.4 vs. 42.7 Ϯ 3.8 nmol/l, pre- vs. posttreatment;
IGF-I or placebo therapy, VLDL apoB pool size, FCR,
placebo group 34.2 Ϯ 4.0 vs. 29.3 Ϯ 3.2 nmol/l, pre- vs.
VLDL apoB secretion, and clearance rate did not
change significantly in either group (Figs. 1 and 2 and
Pretreatment overnight insulin concentrations dur-
ing euglycemia were not significantly different be-
Overnight GH secretion. Mean overnight GH concen-
tween the IGF-I and placebo groups. IGF-I therapy
trations were significantly decreased after IGF-I ther-
resulted in a 25% decrease in mean overnight insulin
apy, whereas no change was observed after placebo
concentrations, whereas no significant change was ob-
(IGF-I group 23.6 Ϯ 3.8 vs. 10.5 Ϯ 1.3 mU/l pre- vs.
served in the placebo group (IGF-I group 35.6 Ϯ 6.7 vs.
posttreatment; placebo group 13.5 Ϯ 1.8 vs. 14.3 Ϯ 1.6
27.0 Ϯ 7.0 mU/l, pre- vs. posttreatment; placebo group
mU/l pre- vs. posttreatment, P Ͻ 0.007). With the use
29.9 Ϯ 4.6 vs. 29.4 Ϯ 3.1 mU/l, pre- vs. posttreatment,
of pulsar analysis, this reduction was attributable to a
reduction in GH peak amplitude (IGF-I group 31.7 Ϯ
Lipid profile. There were no statistically significant
6.3 vs. 21.5 Ϯ 7.2 mU/l, pre- vs. posttreatment; placebo
differences in fasting plasma lipid profiles between the
group 23.0 Ϯ 3.9 vs. 30.4 Ϯ 5.2 mU/l, pre- vs. posttreat-
two groups before treatment. IGF-I therapy signifi-
ment, P Ͻ 0.02) and peak length (IGF-I group 1.5 Ϯ 0.3
cantly decreased total plasma triglyceride concentra-
vs. 1.3 Ϯ 0.2 h, pre- vs. posttreatment, placebo group
tions (P Ͻ 0.03), VLDL-TG concentrations (P Ͻ 0.05),
1.3 Ϯ 0.1 vs. 1.7 Ϯ 0.2 h, pre- vs. posttreatment, P Ͻ
Table 2. Fasting lipid profile in patients with type 1 diabetes mellitus before (study 1)and after (study 2) IGF-I or placebo therapy
Mean Ϯ SE 4.16 Ϯ 0.28 4.03 Ϯ 0.39 2.55 Ϯ 0.24 2.44 Ϯ 0.35 1.17 Ϯ 0.10 1.14 Ϯ 0.09 0.95 Ϯ 0.15 1.01 Ϯ 0.16 0.80 Ϯ 0.05 0.93 Ϯ 0.11
Mean Ϯ SE 4.30 Ϯ 0.51 4.22 Ϯ 0.35 2.11 Ϯ 0.56 2.11 Ϯ 0.39 1.60 Ϯ 0.30 1.53 Ϯ 0.24 1.30 Ϯ 0.26 0.95 Ϯ 0.17 0.86 Ϯ 0.18 0.74 Ϯ 0.13P value
TC, total cholesterol; TG, triglycerides; LDL-C, LDL-cholesterol; HDL-C, HDL-cholesterol; NEFA, nonesterified fatty acid. At baseline, the
placebo- and the IGF-I groups were not statistically different. P values shown here correspond to the results of a comparison of the responses(delta values) of each parameter between the placebo and the IGF-I groups using unpaired t-testing. TG results were analyzed after logtransformation. AJP-Endocrinol Metab • VOL 282 • MAY 2002 • www.ajpendo.org
Table 3. VLDL lipid composition before (study 1) and after (study 2) IGF-I/placeboin patients with type 1 diabetes mellitus
C, cholesterol; VLDL, very low density lipoprotein. At baseline, the placebo- and the IGF-I groups were not statistically different. P values
correspond to the results of a comparison of the responses (delta values) of each parameter between the placebo and the IGF-I groups usingunpaired t-testing. TG results were analyzed after log transformation. * Mean of six pooled samples.
0.03). No change was observed in either the frequencyof peaks or the length of intervals between peaks ineither group. Total area under the GH curve was sig-nificantly decreased by IGF-I, whereas no significantchanges were observed in the placebo group (IGF-Igroup 131.6 Ϯ 46.5 vs. 67.3 Ϯ 25.8 mU ⅐ lϪ1 ⅐ hϪ1 pre- vs. posttreatment; placebo group 82.4 Ϯ 11.9 vs. 91.1 Ϯ15.4 mU ⅐ lϪ1 ⅐ hϪ1 pre- vs. posttreatment, P Ͻ 0.04). IGFBP. Before treatment, IGFBP-1 and IGFBP-3
concentrations were similar in the IGF-I-treated andplacebo groups. Mean IGFBP-1 concentrations in-creased 1.5-fold after IGF-I therapy (IGF-I group82.1 Ϯ 10.1 vs. 124.9 Ϯ 15.8 ng/ml pre- vs. posttreat-ment; placebo group 71.5 Ϯ 13.7 vs. 87.5 Ϯ 13.0 ng/mlpre- vs. posttreatment, ANOVA P Ͻ 0.001). IGFBP-3concentrations did not change significantly in eithergroup (IGF-I group 2,311.4 Ϯ 196.0 vs. 2,541 Ϯ 168.8ng/ml pre- vs. posttreatment; placebo group 2,611.6 Ϯ273.9 vs. 2,694.3 Ϯ 239.9 ng/ml pre- vs. posttreatment,ANOVA P ϭ 0.12). DISCUSSION
This study demonstrates that low-dose IGF-I ther-
apy in adult patients with type 1 diabetes significantlydecreases fasting triglyceride and VLDL-TG concen-trations without affecting VLDL apoB kinetics. AfterIGF-I, overnight GH secretion and mean overnightinsulin concentrations decreased, whereas IGFBP-I
Fig. 1. Mean very low density lipoprotein (VLDL) apolipoprotein(apo) B enrichment with [13C]leucine in patients with type 1 diabetes
concentrations significantly increased.
before (study 1) and after (study 2) 1 wk of insulin-like growth factor
Decreased fasting triglyceride concentrations after
(IGF) I (A) or placebo (B) therapy. Precursor pool enrichment of
IGF-I therapy are consistent with findings in patients
␣-[13C]ketoisocaproate (␣-[13C]KIC) before (KIC study 1) and after
with type 2 (47) and type 1 diabetes mellitus (9).
(KIC study 2) IGF-I (A) or placebo therapy (B) is also shown. Based
Increasing evidence suggests that triglyceride concen-
on the individual curve of each patient’s kinetic parameters of VLDL,apoB metabolism was calculated. No statistically significant differ-
trations may be a significant risk factor for cardiovas-
ences were observed after IGF-I or placebo therapy. APE, atom
cular disease (24) and that lowering triglycerides (32,
AJP-Endocrinol Metab • VOL 282 • MAY 2002 • www.ajpendo.org
crease in insulin sensitivity. Therefore, it is likely thatthe IGF-I-induced improvement in insulin sensitivityhas led to the reduction of triglyceride and VLDL-TGconcentrations. In contrast to previous studies, totalcholesterol and LDL-C did not change significantlyafter IGF-I therapy in this study (9, 47). This may bebecause only 40% of the previous dose of IGF-I wasadministered in this study. Alternatively, the smallsample size did not have enough statistical power todetect statistically significant differences in fastingcholesterol concentrations.
It has been shown previously (26) that, even in
well-controlled diabetic patients, fasting VLDL compo-sition is altered with an increase in lipid content (inparticular triglycerides) within the VLDL fraction com-pared
VLDL-TG concentrations have been associated with aparallel increase in small dense LDL, a subfraction ofLDL particles that are known to be particularly athero-genic (26, 36, 42). In this study after IGF-I therapy,VLDL-TG concentration decreased, as did the VLDL-
Fig. 2. A: VLDL apoB concentrations (means
TG-to-VLDL-apoB ratio. This may indicate a reversal
type 1 diabetes mellitus before (■) and after (ᮀ) IGF therapy.
of the impaired VLDL composition and may be associ-
B: VLDL apoB concentrations (means Ϯ SE) in patients with type 1
ated with improvements in the LDL subfraction profile
diabetes mellitus before (Œ) and after (‚) placebo. No significant
(26, 36, 42). A possible explanation of the findings of
changes in VLDL apoB concentrations were observed during theVLDL apoB turnover studies, indicating a steady-state condition.
this study is that the decrease in GH secretion leads toa reduction in peripheral lipolysis and a decrease in
38) can reduce this risk. These clinical findings are
NEFA flux to the liver (6). The reduced hepatic NEFA
supported by the fact that triglyceride-rich lipoproteins
content, in turn, may result in decreased lipid esterifi-
(i.e., VLDL and IDL) have been identified in human
cation and lower incorporation of triglycerides into
atherosclerotic plaques, and these particles are associ-
VLDL particles (40). This hypothesis is supported by
ated with progression of coronary lesions (45). In-
the tendency for a reduction in NEFA concentrations
creased triglyceride concentrations are associated with
with IGF-I therapy seen here. In addition, administra-
decreased insulin sensitivity (42). A decrease in insulin
tion of GH to healthy subjects in a dose mimicking the
concentrations for a similar glycemic control (euglyce-
increased GH secretion in type 1 diabetes results in a
mia) measured in the current study suggests an in-
compositional change of VLDL particles with an in-
Table 4. Kinetic characteristics of VLDL apoB metabolism in patients with type 1 diabetes mellitusbefore (study 1) and after (study 2) IGF-I/placebo therapy
PV, plasma volume; FCR, fractional catabolic rate; ASR, absolute secretion rate; MCR, metabolic clearance rate. At baseline, the placebo
and IGF-I groups were not statistically different. P values correspond to the results of the comparison of responses (delta values) of eachparameter between the placebo and IGF-I groups using nonparametric testing. AJP-Endocrinol Metab • VOL 282 • MAY 2002 • www.ajpendo.org
crease in triglyceride content (35), supporting our hy-
and the IGF-I groups were not ideally matched for the
apoE phenotype; hence, we cannot exclude that this
The finding of unchanged VLDL apoB kinetics de-
may have influenced our findings. However, differ-
spite a decrease in fasting triglyceride concentrations
ences in VLDL apoB kinetics have been shown only in
is intriguing. It may be related to the small number of
apoE2 homozygous patients (37), not included in the
patients included in this study. A mean reduction in
current study. It is therefore unlikely that the present
VLDL apoB secretion of 33% after IGF-I therapy, al-
results were confounded by the differences in apoE
though not significant statistically, may support this
hypothesis. Alternatively, it is well known that the
In conclusion, the current results indicate that low-
VLDL fraction is heterogeneous, consisting of triglyc-
dose IGF-I therapy (40 g ⅐ kgϪ1 ⅐ dayϪ1) is well toler-
eride-rich (large VLDL) and cholesterol-rich (small
ated and restores the disordered GH-IGF-I axis in type
VLDL) subfractions that are independently secreted by
1 diabetes. IGF-I therapy does not significantly influ-
the liver (36). Insulin is known to act primarily on the
ence VLDL apoB kinetics but changes fasting triglyc-
triglyceride-rich VLDL subfraction (36). The observed
eride concentrations and the composition of VLDL par-
increase in insulin sensitivity may, therefore, primarily
ticles probably because of an increase in insulin
affect the kinetics of triglyceride-rich VLDL subfractions,
sensitivity. The decreased triglyceride content within
which were not assessed separately in this study.
In patients with adult GH deficiency, GH replace-
the VLDL particles leading to a reduction in athero-
ment therapy has been demonstrated to increase whole
genic small dense LDL particles and an increase in
VLDL apoB turnover (11). The current study, however,
IGFBP-1 concentrations may favorably influence the
suggests that VLDL apoB metabolism is unchanged
macrovascular risk profile in type 1 diabetes. In addi-
after IGF-I therapy despite a reduction in GH secre-
tion, by reducing GH secretion, IGF-I may have a
tion. A possible explanation for this effect includes the
beneficial effect on microvascular complications. Fur-
fact that insulin is a powerful regulator of VLDL apoB
ther long-term studies are required to investigate a
metabolism, and, if euglycemia is maintained, it out-
possible role of low-dose IGF-I therapy in the manage-
weighs any possible effects of GH. Alternatively, he-
ment of patients with type 1 diabetes mellitus.
patic GH resistance may occur, as has been suggested,especially in adolescents with type 1 diabetes (1, 4, 10,
We thank Dr. R. Jones, St. Thomas’ Hospital, London, and R. W.
James, Geneva, for reviewing the manuscript.
44). GH is the principal regulator of hepatic synthesis
E. R. Christ was supported by a grant from the Swiss National
of IGFBP-3 (6). Unchanged IGFBP-3 concentrations
Foundation and the Walther and Margarethe Lichtenstein Founda-
after IGF-I therapy despite a decrease in GH secretion
tion (Basel, Switzerland). P. V. Carroll was supported by the Special
are consistent with previous results (28, 44) and sup-
Trustees of St. Thomas’ Hospital. The study was supported by a
port the hypothesis of GH resistance. Possible mecha-
grant from the Juvenile Diabetes Foundation.
nisms include insufficient portal insulinization, lead-ing to decreased hepatic expression of GH receptors
REFERENCES
(23) and/or to insufficient synthesis of IGF-I (5).
1. Acerini CL, Patton CM, Savage MO, Kernell A, Westphal
Reduced IGFBP-1 concentrations are associated
O, and Dunger DB. Randomised placebo-controlled trial of
with an increased prevalence of cardiovascular disease
human recombinant insulin-like growth factor-I plus intensive
in patients with type 2 diabetes (21) and in an elderly
insulin therapy in adolescents with insulin dependent diabetes
nondiabetic population (28). The increase in IGFBP-1
mellitus. Lancet 350: 1199–1204, 1997.
2. Amiel SA, Sherwin RS, Hintz R, Gertner JM, Press CM,
concentrations in the current study may, therefore,
and Tamborlane WV. Effect of diabetes and its control on
indicate a beneficial effect on the cardiovascular risk
insulin-like growth factors in the young subject with type 1
profile in type 1 diabetes mellitus. Our findings are
diabetes. Diabetes 33: 1175–1179, 1984.
consistent with results in some (4), but not in all, of the
3. Angelin B and Rudling M. Growth hormone and hepatic
previous studies (8, 44). Interestingly, the 2.5–5 times
lipoprotein metabolism. Curr Opin Lipidol 5: 160–165, 1994.
lower dose of IGF-I administered in the current study
4. Bach MA, Chin E, and Bondy CA. The effects of subcutaneous
insulin-like growth factor-I infusion in insulin-dependent diabe-
increased IGFBP-1 concentrations to a very similar
tes mellitus. J Clin Endocrinol Metab 79: 1040–1045, 1994.
degree compared with the previous results (4). This is
5. Boni-Schnetzler M, Schmid C, Meier PJ, and Froesch ER.
most likely because of the concomitant insulin treat-
Insulin regulates insulin-like growth factor-I mRNA in rat hepa-
ment. In the current study, euglycemia was achieved
tocytes. Am J Physiol Endocrinol Metab 260: E846–E851, 1991.
by intravenous insulin, whereas in the previous stud-
6. Carroll PV and Christ ER. Members of Growth Hormone
ies subcutaneous intermediate and soluble insulin was
Research Society Scientific Committee. Growth hormone defi-ciency in adulthood and the effects of growth hormone replace-
used, leading to a less tight glycemic control (4, 8).
ment: a review. J Clin Endocrinol Metab 83: 382–395, 1997.
This study has its limitations. First, it was designed
7. Carroll PV, Christ ER, Umpleby AM, Gowrie I, Jackson N,
to investigate VLDL composition, VLDL apoB me-
Bowes SB, Hovorka R, Croos P, So ¨ nksen PH, and Russell-
tabolism, and hormone profiles during euglycemia,
Jones DL. IGF-I treatment in adults with type 1 diabetes.
acutely induced by insulin. It is conceivable that long-
Effects on glucose and protein metabolism in the fasting state
term metabolic control influences these variables and
and during a hyperinsulinaemic-euglycaemic amino acid clamp. Diabetes 49: 789–796, 2000.
should therefore be addressed in further studies. Sec-
8. Carroll PV, Umpleby AM, Alexander EL, Egel VA, Callison
ond, apoE polymorphisms have been shown to influ-
¨ nksen PH, and Russell-Jones DL. Recombinant hu-
ence apoB metabolism (37). The patients in the placebo
man insulin-like growth factor-1 therapy in adults with type 1
AJP-Endocrinol Metab • VOL 282 • MAY 2002 • www.ajpendo.org
diabetes mellitus: effects on IGFs, IGF-binding proteins, glucose
26. James RW and Pometta D. Differences in lipoprotein subfrac-
levels and insulin treatment. Clin Endocrinol (Oxf) 49: 739–746,
tion composition and distribution between type 1 diabetic men
and control subjects. Diabetes 39: 1158–1164, 1990.
9. Carroll PV, Umpleby AM, Ward GS, Imuere S, Alexander
27. Janssen JA, Jacobs ML, Derkx FHM, Weber RFA, Van der E, Dunger D, So ¨ nksen PH, and Russell-Jones DL. RhIGF-I Lely AJ, and Lamberts SWJ. Free and total insulin-like
administration reduces insulin requirement, decreases growth
growth factor I (IGF-I), IGF-binding protein-1 (IGFBP-1) and
hormone secretion, and improves the lipid profile in adults with
IGFBP-3 and their relationships to the presence of diabetic
IDDM. Diabetes 46: 1453–1458, 1997.
retinopathy and glomerular hyperfiltration in insulin-dependent
10. Cheetham T, Jones J, Taylor AM, Holly J, Matthews DR,
diabetes mellitus. J Clin Endocrinol Metab 82: 2809–2815, 1997. and Dunger DB. The effects of recombinant insulin-like growth
28. Janssen JAMJL, Stolk RP, Pols HAP, Grobbee DE, and
factor-I administration on growth hormone levels and insulin
Lamberts SWJ. Serum total IGF-I, free IGF-I and IGFBP-1
requirements in adolescents with type I (insulin-dependent)
levels in an elderly population: relation to cardiovascular risk
diabetes mellitus. Diabetologia 36: 678–681, 1993.
factors and disease. Arterioscler Thromb Vasc Biol 18: 277–282,
11. Christ ER, Cummings MH, Albany E, Umpleby AM, Lumb PJ, Wierzbicki AS, Naoumova RP, Boroujerdi MA,
29. Kesaeniemi YA, Beltz WF, and Grundy SM. Comparisons of ¨ nksen PH, and Russell-Jones DL. Effects of growth hor-
metabolism of apolipoprotein B in normal subjects, obese pa-
mone (GH) replacement therapy on very low density lipoprotein
tients, and patients with coronary heart disease. J Clin Invest
apolipoprotein B100 kinetics in patients with adult GH defi-
ciency: a stable isotope study. J Clin Endocrinol Metab 84:
30. Kissebah AH, Alfarsi S, Evans DJ, and Adams PW. Inte-
grated regulation of very low density lipoprotein triglyceride and
12. Cobelli C, Toffolo G, and Foster DM. Tracer-to-tracee ratio
apolipoprotein B kinetics in non-insulin dependent diabetes mel-
for analysis of stable isotope tracer data: link with radioactive
litus. Diabetes 31: 217–225, 1982.
kinetic formalism. Am J Physiol Endocrinol Metab 262: E968–
31. Krolewski AS, Kosinski EI, Warram JH, Leland OS, Busick EJ, Asmal AC, Rand LI, Christlieb AR, Bradley RF,
13. Cummings MH, Watts GF, Lumb PJ, and Slavin BM. Com- and Kahn CR. Magnitude and determinants of coronary artery
parison of immunoturbimetric and Lowry methods for measur-
disease in juvenile-onset, insulin dependent diabetes mellitus.
ing concentration of very low density lipoprotein apolipoprotein
Am J Cardiol 59: 750–755, 1987.
B-100 in plasma. J Clin Pathol 47: 176–178, 1994.
32. Mack WJ, Krauss RM, and Hodis HN. Lipoprotein subclasses
14. Cummings MH, Watts GF, Umpleby AM, Hennessy TR,
in the Monitored Atherosclerosis Regression Study (MARS). Naoumova RP, Slavin BM, Thompson GR, and So
Treatment effects and relation to angiographic progression. Ar-PH. Increased hepatic secretion of very low density lipoprotein terioscler Thromb Vasc Biol 16: 697–701, 1996.
apolipoprotein B100 in NIDDM. Diabetologia 38: 959–967,
33. Matthews DE, Schwartz HP, Yand RD, Motil KJ, Young VR, and Bier DM. Relationship of plasma leucine and alpha-
15. Cummings MH, Watts GF, Umpleby AM, Hennessy TR,
ketoisocaproate during L-[1-13C]leucine infusion in man: a
Quiney JR, and So ¨ nksen PH. Increased hepatic secretion of
method for measuring human intracellular leucine tracer en-
very low density lipoprotein apolipoprotein B100 in heterozy-
richment. Metabolism 31: 1105–1112, 1982.
gous familial hypercholesterolaemia: a stable isotope study. Ath-
34. Menzel HJ and Utermann G. Apolipoprotein E phenotyping erosclerosis 113: 79–89, 1995.
from serum Western blotting. Electrophoresis 7: 492–495, 1986.
16. Dunger DB, Cheetham TD, and Crowne EC. Insulin-like
35. Moller A, Rasmussen LM, Thuesen L, and Christiansen
growth factors (IGFs) and IGF-I treatment in the adolescent
JS. Impact of human growth hormone on plasma lipoprotein
with insulin-dependent diabetes mellitus. Metabolism 44, Suppl
concentrations. Horm Metab Res 21: 207–209, 1989.
36. Packard CJ and Shepherd J. Lipoprotein heterogeneity and
17. Dunn FL. Plasma lipid and lipoprotein disorders in IDDM.
apolipoprotein B metabolism. Arterioscler Thromb Vasc Biol 17:
Diabetes 41, Suppl 2: 102–106, 1992.
18. Flyvbjerg A. Growth factors and diabetic complications. Diabet
37. Riches RM; Watts GF, van Bockxmeer FM, Hua J, Song S, Humphries SE, and Talmud PJ. Apolipoprotein B signal
19. Friedewald WT, Levy RI, and Fredrickson DS. Estimation
peptide and apolipoprotein E genotype as determinants of the
of the concentration of low density lipoprotein cholesterol in
hepatic secretion of VLDL apoB in obese men. J Lipid Res 39:
plasma without the use of the ultracentrifuge. Clin Chem 18:
38. Rubins HB, Robins SJ, Collins D, Fye CL, Anderson JW,
20. Gibbons GF. Assembly and secretion of hepatic very low-den- Elam MB, Faas F, Linares E, Schaefer EJ, Schectman GH,
sity lipoprotein. Biochem J 268: 1–13, 1990. Wilt TJ, and Wittes J. Gemfibrozil for the secondary preven-
21. Gibbson JM, Westwood M, Young RJ, and White A. Re-
tion of coronary heart disease in men with low levels of high-
duced insulin-like growth factor binding protein-1 (IGFBP-1)
density lipoprotein cholesterol. N Engl J Med 341: 410–418,
correlates with increased cardiovascular risk in non-insulin de-
pendent diabetes. J Clin Endocrinol Metab 81: 860–863, 1996.
39. Rudling M, Norstedt G, Olivecrona H, Reihner E, Gus-
22. Gregersen MI and Rawson RA. Blood volume. Physiol Rev 39: tafsson JA, and Angelin B. Importance of growth hormone for
the induction of hepatic low density lipoprotein receptor. Proc
23. Hanaire-Broutin H, Sallerin-Craute B, Poncet MF, Tauber Natl Acad Sci USA 89: 6983–6987, 1992. M, Bastide R, Rosenfeld R, and Tauber JP. Insulin therapy
40. Sniderman AD and Cianflone K. Substrate delivery as a
and GH-IGF-I axis disorders in diabetes:impact of glycaemic
determinant of hepatic apoB secretion. Arterioscler Thromb 13:
control and hepatic insulinisation. Diabetes Metab 22: 245–250,
¨ nksen PH. Hormones in Human Blood. Cambridge, MA:
24. Hokanson JE and Austin MA. Plasma triglyceride level is a
Harvard Univ Press, 1976. p. 176–199.
risk factor for cardiovascular disease independent of high-den-
42. Taskinen MR. Quantitative and qualitative lipoprotein abnor-
sity lipoprotein cholesterol level: a meta-analysis of population-
malities in diabetes mellitus. Diabetes 2: 12–17, 1992.
based prospective studies. J Cardiovasc Risk 3: 213–217, 1996.
43. Teale JD and Marks V. Inappropriately elevated plasma insu-
25. Hussain MA, Schmitz O, Mengel A, Keller A, Christiansen
lin-like growth factor II in relation to suppressed insulin-like
JS, Zapf J, and Froesch ER. Insulin-like growth factor-I
growth factor I in the diagnosis of non-islet cell tumor hypogly-
stimulates lipid oxidation, reduces protein oxidation and en-
caemia. Clin Endocrinol (Oxf) 33: 97–98, 1990.
hances insulin sensitivity in humans. J Clin Invest 95: 2249–
44. Thraikill K, Quattrin T, Baker L, Litton J, Dwigun K, Rearson M, Poppenheimer M, Kotlovker L, Giltinan D, AJP-Endocrinol Metab • VOL 282 • MAY 2002 • www.ajpendo.org
Gesundheit N, and Paul M. Dual hormonal replacement ther-
46. Zenobi PD, Graf S, Ursprung H, and Froesch ER. Effects
apy with insulin and recombinant human insulin-like growth
of insulin-like growth factor-I on glucose tolerance, insulin
factor-I in insulin-dependent diabetes mellitus: effects on the
levels and insulin secretion. J Clin Invest 89: 1908 – 1913,
growth hormone/IGF/IGF-binding protein system. J Clin Endo-crinol Metab 82: 1181–1187, 1997.
47. Zenobi PD, Jaeggi-Groisman SE, Riesen WF, Roder ME,
45. Williams KJ, Petrie KA, Broacia RW, and Swenson TL. and Froesch ER. Insulin-like growth factor-I improves glucose
Lipoprotein lipase modulates net secretory output of apolipopro-
and lipid metabolism in type II diabetes mellitus. J Clin Invest
tein B in vitro. J Clin Invest 88: 1300–1306, 1991. AJP-Endocrinol Metab • VOL 282 • MAY 2002 • www.ajpendo.org
Each school site shal fol ow its school discipline plan and consider suspension from school only when other means have not been successful or where the student's presence would constitute a danger to persons or property or seriously disrupt the educational process. This comprises sufficient prior warning to students and parents of the consequences of misconduct. Suspension: the temporary removal o
PATIENT PAIN ASSESSMENT Part A: Body and Pain Scale Please mark, on the drawings below, the areas where you feel pain. Write “E” if external or “I” if internal. Write “EI” if both external and internal. Please use numbered pain scores and additional descriptive words like: neuropathic, intense (deep or surface), sharp, hot, dull, cold, sensitive, tender, itchy, shooti
 Am J Physiol Endocrinol Metab 282: E1154–E1162, 2002.
Am J Physiol Endocrinol Metab 282: E1154–E1162, 2002.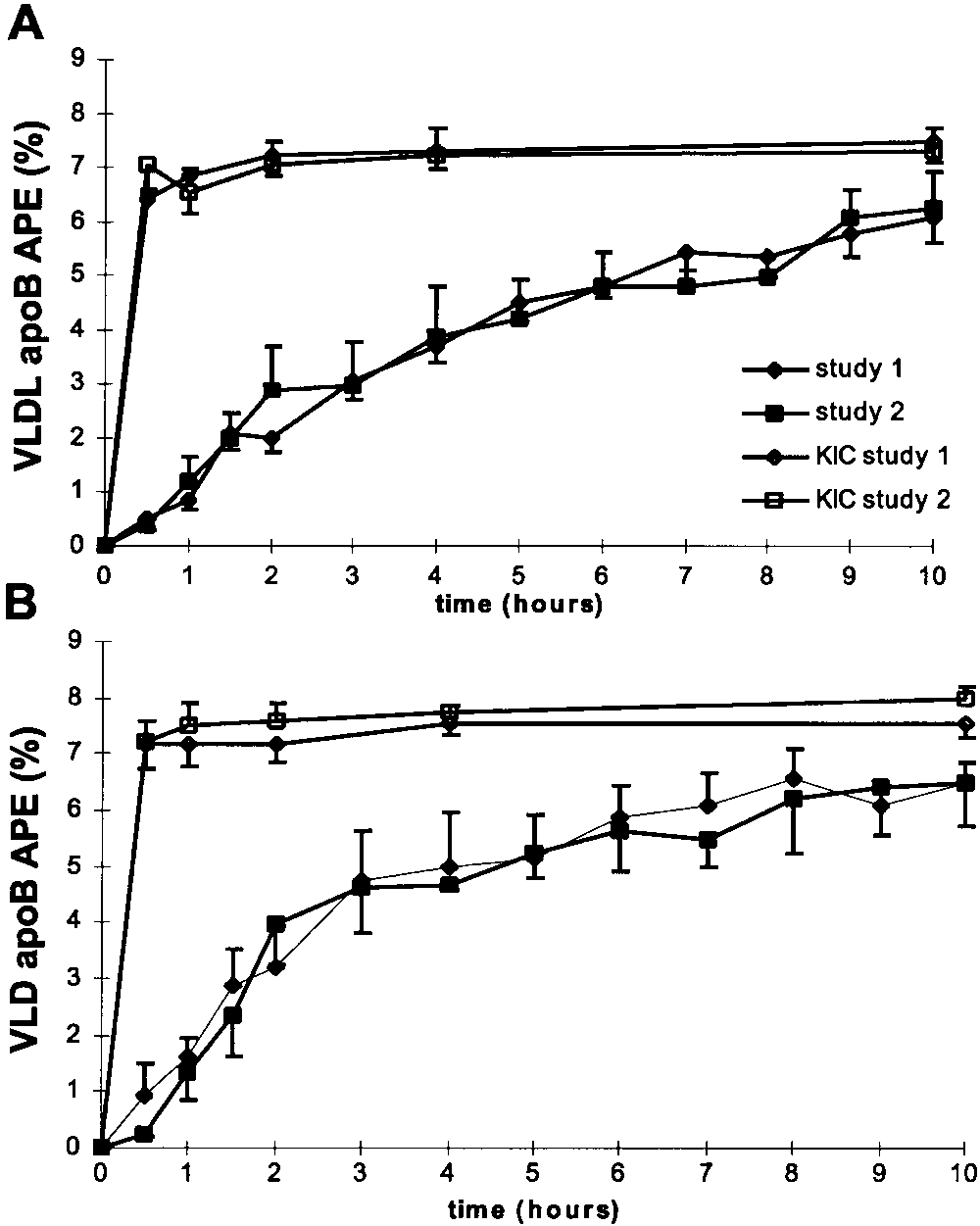 Table 3. VLDL lipid composition before (study 1) and after (study 2) IGF-I/placeboin patients with type 1 diabetes mellitus
C, cholesterol; VLDL, very low density lipoprotein. At baseline, the placebo- and the IGF-I groups were not statistically different. P values
correspond to the results of a comparison of the responses (delta values) of each parameter between the placebo and the IGF-I groups usingunpaired t-testing. TG results were analyzed after log transformation. * Mean of six pooled samples.
Table 3. VLDL lipid composition before (study 1) and after (study 2) IGF-I/placeboin patients with type 1 diabetes mellitus
C, cholesterol; VLDL, very low density lipoprotein. At baseline, the placebo- and the IGF-I groups were not statistically different. P values
correspond to the results of a comparison of the responses (delta values) of each parameter between the placebo and the IGF-I groups usingunpaired t-testing. TG results were analyzed after log transformation. * Mean of six pooled samples.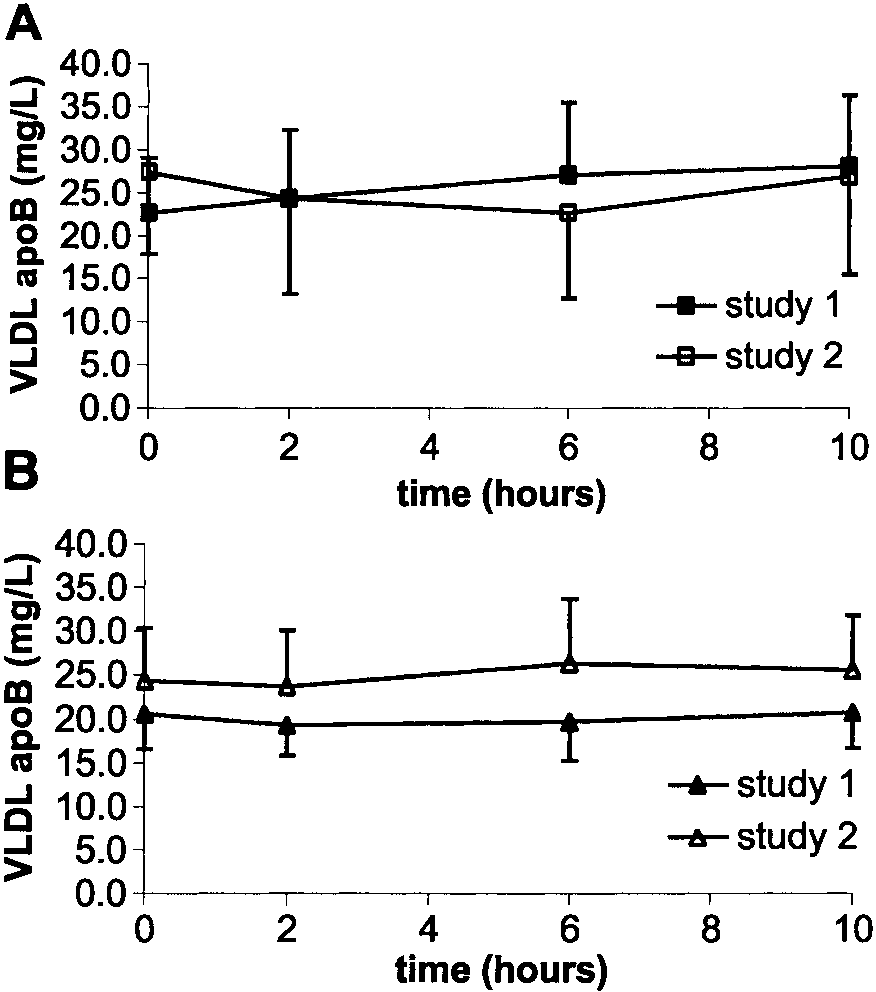 crease in insulin sensitivity. Therefore, it is likely thatthe IGF-I-induced improvement in insulin sensitivityhas led to the reduction of triglyceride and VLDL-TGconcentrations. In contrast to previous studies, totalcholesterol and LDL-C did not change significantlyafter IGF-I therapy in this study (9, 47). This may bebecause only 40% of the previous dose of IGF-I wasadministered in this study. Alternatively, the smallsample size did not have enough statistical power todetect statistically significant differences in fastingcholesterol concentrations.
crease in insulin sensitivity. Therefore, it is likely thatthe IGF-I-induced improvement in insulin sensitivityhas led to the reduction of triglyceride and VLDL-TGconcentrations. In contrast to previous studies, totalcholesterol and LDL-C did not change significantlyafter IGF-I therapy in this study (9, 47). This may bebecause only 40% of the previous dose of IGF-I wasadministered in this study. Alternatively, the smallsample size did not have enough statistical power todetect statistically significant differences in fastingcholesterol concentrations. Gesundheit N, and Paul M. Dual hormonal replacement ther-
Gesundheit N, and Paul M. Dual hormonal replacement ther-