Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Medicinemcq.com
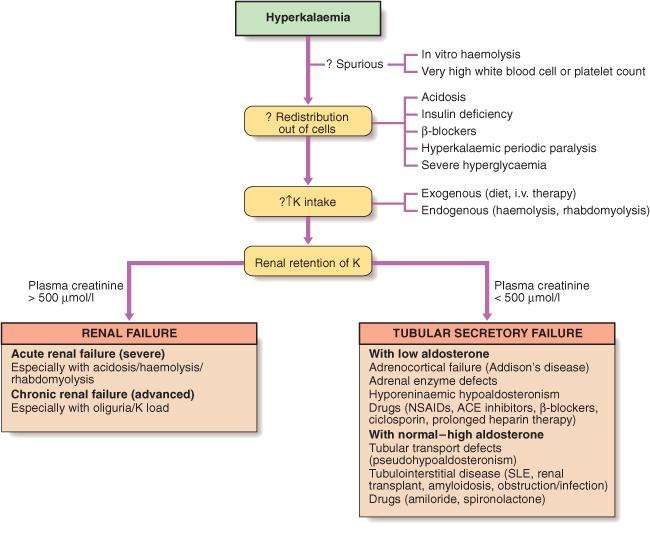
Page 1 of 14 DR. RAJENDRAN’S INSTITUTE OF MEDICAL EDUCATION HYPERKALEMIA 1) Hyperkalemia is plasma K+ concentration more than ----------- mEq/L T [ Hyperkalemia is defined as a plasma (not serum) K+ concentration > 5.0 mmol/L. Hyperkalemia may be due to release of K+ from cells or decreased renal loss. Increased dietary K+ intake does not usually cause hyperkalemia since renal K+ excretion increases in response to increases in dietary consumption.] www.medicinemcq.com
Page 2 of 14 2) What is/are the cause(s) of pseudohyperkalemia? a. Prolonged use of a tourniquet [ Pseudohyperkalemia is an increase in potassium concentration only in vitro (or in the local blood vessel). It has no physiological consequences. Pseudohyperkalemia is artificially elevated plasma K+ concentration due to movement of K+ out of cells. Normally, intracellular concentration of K+ is high (140mEq/L) and plasma concentration of K+ is low (5mEq/L). Small leaks of K+ out of blood cells can increase serum K+ levels considerably. When blood is allowed to clot before centrifugation, enough K is released from platelets to raise serum K by approximately 0.5 mEq/L. This is accounted for within normal limits. However, excessive errors can occur in the presence of marked thrombocytosis, marked leukocytosis, or hemolysis on obtaining blood samples. These conditions are referred to as ‘‘pseudohyperkalemia.’’ This can occur immediately prior to or following venepuncture. Prolonged use of a tourniquet with or without repeated fist clenching is a contributing factor. Prolonged use of a tourniquet with fist exercises can increase the serum potassium level by as much as l mEq/L.] b. Hemolysis [ In intravascular hemolysis, K+ is released from the hemolysed RBCs. As 98% of body potassium is located within cells, cell death can result in hyperkalemia.] c. Leukocytosis [ High leukocyte and platelet counts may also artificially elevate potassium levels due to lysis of these cells after the blood is drawn. The elevated serum K+ concentration is due to release of intracellular K+ following clot formation. If plasma (not serum) K+ concentration is measured, it should be normal.] d. Tumor lysis syndrome [ Tumor lysis syndrome is caused by the destruction of a large number of rapidly proliferating neoplastic cells. Potassium is the main intracellular cation. Therefore, massive destruction of malignant cells may cause hyperkalemia. Tumor lysis syndrome and rhabdomyolysis lead to K+ release from cells as a result of tissue breakdown. Muscle breakdown from crush injury or rhabdomyolysis increase serum K+ concentration.] e. All of the above T [ Suspect pseudohyperkalemia in an otherwise asymptomatic patient with no obvious underlying cause. In pseudohyperkalemia, no electrocardiographic abnormalities are present.] www.medicinemcq.com
Page 3 of 14 3) Which of the following is not raised in tumor lysis syndrome? a. Uric acid [ Tumor lysis syndrome is caused by the destruction of a large number of rapidly proliferating neoplastic cells. Effective treatment kills malignant cells and leads to increased serum uric acid levels from the turnover of nucleic acids. Uric acid can precipitate in the tubules, medulla, and collecting ducts of the kidney, leading to renal failure. Uric acid crystals in the urine strongly suggest uric acid nephropathy.] b. Phosphate [ Hyperphosphatemia is caused by the release of intracellular phosphate by tumor cell lysis. Hyperphosphatemia produces a reciprocal depression in serum calcium.] c. Potassium [ Potassium is the main intracellular cation. Therefore, massive destruction of malignant cells may cause hyperkalemia.] d. Lactic acid e. Calcium T [ Tumor lysis syndrome is characterized by various combinations of hyperuricemia, hyperkalemia, hyperphosphatemia, lactic acidosis, and hypocalcemia. Acute renal failure is a common complication of the syndrome.] 4) Tumor lysis syndrome is most frequently associated with a. Multiple myeloma b. Burkitt's lymphoma T [ Tumor lysis syndrome is most frequently associated with the treatment of Burkitt's lymphoma, acute lymphoblastic leukemia, and other high-grade lymphomas. The risk of tumor lysis syndrome in Burkitt's lymphoma is related to the tumor burden and renal function. Hyperuricemia and high serum levels of lactate dehydrogenase correlate with total tumor burden, also correlate with the risk of tumor lysis syndrome.] c. Ovarian carcinoma www.medicinemcq.com
Page 4 of 14 d. Hypernephroma 5) Useful in the treatment of tumor lysis syndrome a. Allopurinol [ Prevention is the most important step in the management. Allopurinol, urinary alkalinization, and aggressive hydration are the main preventive measures.] b. Rasburicase [ Rasburicase is recombinant urate oxidase. Urate oxidase catalyzes the conversion of poorly soluble uric acid to readily soluble allantoin. This enzyme is not present in humans. Rasburicase decreases uric acid levels within hours. Rasburicase is contraindicated in patients with glucose-6-phosphate dehydrogenase deficiency.] c. Dialysis [ Hemodialysis is often necessary and should be considered early in the course.] d. All of the above T [ Prognosis is excellent.] 6) Cause of hyperkalemia a. Metabolic acidosis [ In metabolic acidosis, hydrogen ions enter the cells and potassium ions come out of the cells.] b. Insulin deficiency [ Insulin stimulates entry of glucose and potassium into cells. Thus, insulin lowers plasma potassium and is used in the treatment of hyperkalemia. Insulin deficiency and hypertonicity due to hyperglycemia promote K+ shift from the ICF to the ECF.] www.medicinemcq.com
Page 5 of 14 c. Exercise [ Exercise-induced hyperkalemia is due to release of K+ from muscles. The severity of exercise-induced hyperkalemia is related to the degree of exertion. It is rapidly reversible and is often associated with rebound hypokalemia. Hyperkalemic periodic paralysis is a rare autosomal dominant disorder characterized by episodic weakness or paralysis. It is precipitated by stimuli that normally lead to mild hyperkalemia (e.g., exercise).] d. Beta blockers [ Treatment with beta blockers rarely causes hyperkalemia.] e. All of the above T [ Hyperkalemia may occur with severe digitalis toxicity due to inhibition of the Na-K-ATPase pump.] 7) What is the most common cause of acute hyperkalemia? a. Renal failure T [ Acute renal failure is the most common cause of rapid onset of hyperkalemia. Acute decreases in GFR lead to marked decreases in distal delivery of salt and water, which secondarily decrease distal K secretion. Thus, when acute renal failure is oliguric, hyperkalemia is frequent. When acute renal failure is nonoliguric, distal sodium and water delivery is usually sufficient and hyperkalemia is unusual.] b. Spiranolactone [ Spironolactone, triamterene, beta-blockers, cyclosporine and tacrolimus may cause hyperkalemia.] c. Hemorrhagic infarction of both adrenal glands [ Damage to the adrenals can result in hyperkalemia.] d. Reperfusion of ischemic skeletal muscle [ Reperfusion injury occurs at the completion of arterial injury repair. Rhabdomyolysis leads to release of K+. Sodium bicarbonate can prevent hyperkalemia and cardiac arrest. Give bolus IV infusion of sodium bicarbonate immediately before reperfusion of the ischemic tissues by release of the arterial clamp. The bicarbonate shifts potassium from the ECF across the cell membrane into ICF.] www.medicinemcq.com
Page 6 of 14 8) What is the most common cause of chronic hyperkalemia? a. Hyperkalemic periodic paralysis [ Hyperkalemic periodic paralysis is a rare autosomal dominant disorder due to a mutation in the gene for the skeletal muscle Na+ channel. It is characterized by episodic weakness or paralysis. It is precipitated by stimuli that normally lead to mild hyperkalemia (e.g., exercise).] b. Succinylcholine [ Succinylcholine can increase the plasma K+ concentration, especially in patients with massive trauma, burns, or neuromuscular disease.] c. Decreased renal K+ excretion T [ Chronic hyperkalemia is almost always due to decreased renal K+ excretion due to hyporeninemic hypoaldosteronism.] d. Angiotensin-converting enzyme inhibitors [ Patients getting ACE inhibitors or angiotensin receptor antagonists are at increased risk of hyperkalemia. Patients with diabetes mellitus, renal insufficiency, decreased effective circulating arterial volume, and bilateral renal artery stenosis are particularly at risk. Concurrent use of K+-sparing diuretics or NSAIDs also increases the risk.] e. NSAIDs [ NSAIDs inhibit renin secretion and the synthesis of vasodilatory renal prostaglandins. Hyperkalemia may develop due to decrease in GFR and K+ secretion.] 9) What is/are the cause(s) of hyporeninemic hypoaldosteronism? a. Renal insufficiency b. Diabetic nephropathy [ Hyporeninemic hypoaldosteronism is the most common cause of aldosterone deficiency states. It is the commonest cause of chronic hyperkalemia among nondialysis patients. Hyporeninemic hypoaldosteronism is characterized by euvolemia or ECF volume expansion and suppressed renin and aldosterone levels. As a rule, the degree of hyperkalemia due to hypoaldosteronism is mild in the absence of increased K+ intake or renal dysfunction. Diabetic nephropathy and interstitial renal disease are the most common causes of hyporeninemic hypoaldosteronism.] www.medicinemcq.com
Page 7 of 14 c. Chronic tubulointerstitial disease [ Diseases associated with inflammation in the tubulointerstitium (e.g., SLE, renal transplant) can cause aldosterone resistance. When there is aldosterone resistance, tubular secretion of potassium is impaired, even in the presence of high aldosterone levels. Aldosterone resistance can also occur during therapy with potassium- sparing diuretics.] d. All of the above T [ Drugs that inhibit the release of renin may provoke hyperkalemia (ACE inhibitors, nonsteroidal anti-inflammatory agents, beta-blockers). Therapy with angiotensin receptor antagonists, NSAIDs or beta-blocking drugs can cause hyporeninaemic hypoaldosteronism.] 10) Which one of the following drugs decreases aldosterone synthesis? a. Trimethoprim [ Trimethoprim and pentamidine block distal nephron Na+ reabsorption and thus impair K+ secretion.] b. Heparin T [ Heparin inhibits production of aldosterone by the cells of the zona glomerulosa. Heparin can cause severe hyperkalemia in patients with underlying renal disease, diabetes mellitus, or those receiving K+-sparing diuretics, ACE inhibitors, or NSAIDs. Two other causes of decreased aldosterone synthesis are Addison's disease (primary adrenal insufficiency) or congenital adrenal enzyme deficiency.] c. Spironolactone [ Spironolactone is a competitive aldosterone antagonist.] d. Amiloride [ Amiloride and triamterene block the apical Na+ channel of the principal cell. Amiloride and triamterene inhibit Na reabsorption, which abolishes the lumen negative potential and therefore inhibits K secretion.] e. 9a-fludrocortisone [ 9a-fludrocortisone is a synthetic Mineralocorticoid.] www.medicinemcq.com
Page 8 of 14 11) Renal cause(s) of hyperkalemia a. Acute oliguric renal failure [ Hyperkalemia is a common complication of acute oliguric renal failure. Hyperkalemia is due to increased K+ release from cells (acidosis, catabolism) and decreased excretion.] b. Chronic renal failure [ Increased distal flow rate and K+ secretion by surviving nephrons may maintain normal plasma K+ concentration. However, these adaptive mechanisms eventually fail to maintain K+ balance when the GFR falls below 10 to 15 mL/min or oliguria ensues.] c. Urinary tract obstruction [ Urinary tract obstruction is an often overlooked cause of hyperkalemia.] d. Diabetic nephropathy [ Other nephropathies associated with impaired K+ excretion include drug-induced interstitial nephritis, lupus nephritis, sickle cell disease, and diabetic nephropathy.] e. All of the above 12) What is/are the clinical manifestion(s) of hyperkalemia? a. Quadriparesis [ The resting membrane potential is related to the ratio of the ICF to ECF K+ concentration. Therefore, hyperkalemia partially depolarizes the cell membrane. The most important manifestation of prolonged depolarization is muscle weakness. The muscle weakness may progress to flaccid paralysis.] b. Hypercapnia [ Hypoventilation develops if the respiratory muscles are involved.] c. Metabolic acidosis [ Hyperkalemia inhibits renal ammonia synthesis and reabsorption of NH4+ in the thick ascending limb of the loop of Henle. Thus, H+ ion excretion is impaired and results in metabolic acidosis. Metabolic acidosis further exacerbates the hyperkalemia due to K+ movement out of cells.] www.medicinemcq.com
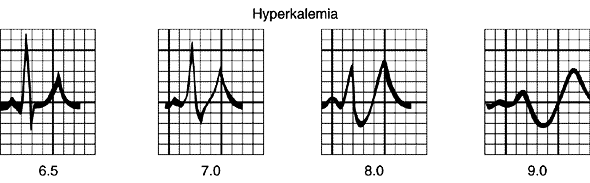
Page 9 of 14 d. Ventricular fibrillation [ The most serious effect of hyperkalemia is cardiac toxicity. It does not correlate well with the plasma K+ concentration. The earliest ECG change is either increased T-wave amplitude or peaked T waves. Ventricular fibrillation or asystole is usually a terminal event.] e. All of the above T [ Patients typically present with progressive muscular weakness, but sometimes there are no symptoms until cardiac arrest occurs. Potentially fatal hyperkalemia rarely occurs unless the plasma K+ concentration exceeds 7.5 mEq/L and is usually associated with profound weakness and absent P waves, QRS widening, or ventricular arrhythmias on the electrocardiogram.] 13) What is the earliest electrocardiographic change of hyperkalemia? a. Peaked T waves T [ Cardiac toxicity does not correlate well with the plasma K+ concentration. The earliest ECG change is either increased T-wave amplitude or peaked T waves. See figure below.] b. Prolonged PR interval [ More severe degrees of hyperkalemia result in a prolonged PR interval and QRS duration, atrioventricular conduction delay, and loss of P c. Widening of the QRS complex [ Progressive widening of the QRS complex and merging with the T wave produces a sine wave pattern. Peaking of the T wave is an early ECG sign, but widening of the QRS complex presages a dangerous cardiac arrhythmia. The terminal event is usually ventricular fibrillation or asystole.] d. Atrioventricular conduction delay e. Loss of P waves www.medicinemcq.com
Page 10 of 14 14) What is the first step in the differential diagnosis of hyperkalemia? a. Rule out pseudohyperkalemia T [ The first step in the differential diagnosis of hyperkalemia is to rule out pseudohyperkalemia. ECG abnormalities of hyperkalemia are absent in pseudohyperkalemia. The absence of ECG changes does not eliminate true hyperkalemia because ECG changes are rare in chronic hyperkalemia. Pseudohyperkalemia should be suspected in conditions known to cause pseudohyperkalemia, such as thrombocytosis or in vitro hemolysis (pink serum). In pseudohyperkalemia due to thrombocytosis, both serum and plasma K+ should be obtained simultaneously.] b. Measurement of a 24-hour urine K+ [ Once pseudohyperkalemia is ruled out, the next step is to differentiate among the three major causes of hyperkalemia: increased K+ intake, shift of K+ from the cell, and impaired renal excretion. A careful dietary history will be sufficient to rule out hyperkalemia due to increased intake. Measurement of a 24-hour urine K+ will distinguish increased intake from the other two causes. Although hyperkalemia due to a shift of K+ from the cell would result in an increased urinary excretion of K+, renal excretion of K+ is often not increased because impaired renal excretion of K+ often contributes to hyperkalemia.] c. Blood urea and serum creatinine [ Among the renal causes of hyperkalemia, acute renal failure is the most common cause of acute hyperkalemia. This will be obvious from serum creatinine and BUN.] www.medicinemcq.com
Page 11 of 14 d. Urinary excretion of Na+ and K+ [ Chronic hyperkalemia is almost always due to impaired renal excretion. For differential diagnosis of chronic hyperkalemia of renal causes, the first step is to measure plasma renin activity, plasma aldosterone, and urinary excretion of Na+ and K+. A very low urinary Na+ and a low K+ in the absence of polyuria suggest that the aldosterone effect is normal. If urinary Na+ is adequate (> 20 mEq/L), plasma renin activity and aldosterone should be measured.] e. Plasma renin activity [ Low PRA and low aldosterone suggest hyporeninemic hypoaldosteronism. High PRA and low aldosterone suggest Addison's disease, heparin therapy, and aldosterone biosynthetic defect. Treatment with potassium-sparing diuretics (e.g., amiloride, triamterene, and spironolactone) increase both PRA and aldosterone.] www.medicinemcq.com
Page 12 of 14 15) Treatment of hyperkalemia a. Calcium gluconate IV [ Calcium gluconate decreases membrane excitability. Calcium antagonizes the depolarization effect of elevated K+.] b. Insulin [ Insulin causes K+ to shift into cells from ECF and will temporarily lower the plasma K+ concentration. Insulin is given with glucose to prevent hypoglycemia.] c. NaHCO3 IV [ Alkalosis caused IV NaHCO3 therapy can also shift K+ into cells.] d. Beta 2 adrenergic agonists [ Beta 2 adrenergic agonists promote cellular uptake of K+ when administered parenterally or in nebulized form. The onset of action is 30 min and the effect lasts 3 hours.] e. All of the above [ Potentially fatal hyperkalemia rarely occurs unless the plasma K+ concentration exceeds 7.5 mEq/L and is usually associated with profound weakness and absent P waves, QRS widening, or ventricular arrhythmias on the electrocardiogram.] 16) What is the most rapid and effective way of lowering the plasma K+ concentration? a. Loop diuretics [ Loop and thiazide diuretics, often in combination, enhance K+ excretion if renal function is adequate.] b. Cation-exchange resin [ Sodium polystyrene sulfonate is a cation- exchange resin that binds potassium in the gut lumen (promotes the exchange of Na+ for K+ ). Each gram binds 1 mEq of K+ and releases 2 to 3 mmol of Na+. It can be given by mouth or as a retention enema. Chronic hyperkalemia associated with renal dysfunction can be managed by oral or rectal administration of sodium polystyrene sulfonate.] www.medicinemcq.com
Page 13 of 14 c. Hemodialysis T [ Hemodialysis is the most rapid and effective way of lowering the plasma K+ concentration. It is indicated in patients with renal failure and those with severe life-threatening hyperkalemia unresponsive to other treatments. Hemodialysis is the most reliable method for controlling hyperkalemia in patients with acute renal failure. Peritoneal dialysis is only 20% as effective as hemodialysis.] d. Correction of metabolic acidosis e. Mineralocorticoid 17) What is the first treatment in hyperkalemia with ECG changes? a. Infusion of calcium gluconate T [ If ECG changes are present, the first step should be infusion of calcium gluconate to stabilise conductive tissue membranes. Calcium has the opposite effect of potassium on conduction of an action potential.] b. Insulin and glucose [ Also use measures to shift potassium from the ECF to the ICF. These act rapidly and may avert cardiac complications of hyperkalaemia.] c. IV frusemide [ This will remove K+ from the body if adequate renal function is present.] d. Ion-exchange resins [ In renal failure, use ion-exchange resins acting through the gastrointestinal tract and arrange for urgent dialysis.] e. Urgent dialysis www.medicinemcq.com
Page 14 of 14 TREATMENT OF HYPERKALAEMIA Mechanism Stabilise cell membrane potential IV calcium gluconate (if ECG changes suggestive of hyperkalaemia and/or K > 7 mEq/L) Shift K into cells Inhaled beta 2 agonist IV glucose and insulin IV sodium bicarbonate (if acidosis present) Remove K from body IV furosemide and normal saline (if adequate residual renal function) Ion-exchange resin Dialysis www.medicinemcq.com
Work and Kinetic Energy Homework Problems1. An intern pushes a 72 kg patient on a 15 kg gurney, producing an acceleration of 0.60 a. How much work does the intern do by pushing the patient and the gurney through a distance of 2.5 m? Assumed the gurney moves without frictionb. How far must the intern push the gurney to do 140 J of work?2. One species of Darwins finch, Geospiza magnirostris ,
Diagnosis and therapy of tuberculous meningitis in childrenDepartment of Maternal and Pediatric Sciences, Università degli Studi di Milano, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico,Via Commenda 9, 20122 Milan, ItalyChildren are among the subjects most frequently affected by tuberculous meningitis (TBM) due to theirrelative inability to contain primary Mycobacterium tuber
 Page 10 of 14
Page 10 of 14 
 Page 11 of 14
Page 11 of 14