Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Evaluation of asymptomatic .
Evaluation of Asymptomatic Microscopic Hematuria in Adults - Septembe.
http://www.aafp.org/afp/AFPprinter/990915ap/1143.html?print=yes
Evaluation of Asymptomatic Microscopic Hematuria in Adults
University of Kansas Medical Center, Kansas City, Kansas hematuria, written by the
Valley Urology Center, Renton, Washington
In patients without significant urologic symptoms, microscopic hematuria is occasionally detected on routine
urinalysis. At present, routine screening of all adults for microscopic hematuria with dipstick testing is not
recommended because of the intermittent occurrence of this finding and the low incidence of significant
associated urologic disease. However, once asymptomatic microscopic hematuria is discovered, its cause
should be investigated with a thorough medical history (including a review of current medications) and a
focused physical examination. Laboratory and imaging studies, such as intravenous pyelography, renal
ultrasonography or retrograde pyelography, may be required to determine the degree and location of the
associated disease process. Cystourethroscopy is performed to complete the evaluation of the lower
urinary tract. Microscopic hematuria associated with anticoagulation therapy is frequently precipitated by
significant urologic pathology and therefore requires prompt evaluation. (Am Fam Physician
Microscopic hematuria is defined as the excretion of more than three red bloodcells per high-power field in a centrifuged urine specimen.1 Because the degree of
hematuria bears no relation to the seriousness of the underlying cause, hematuriashould be considered a symptom of serious disease until proved otherwise.
The widespread use of dipstick urinalysis in clinical practice
and health screening has resulted in increased recognition of
microscopic hematuria and has raised concerns about the
appropriate diagnostic investigation. The prevalence of
the degree of hematuria does notcorrelate with the seriousness of the
asymptomatic microscopic hematuria in adult men and
postmenopausal women has been reported to range from 10percent to as high as 20 percent.2-4 Routine screening of all
adults for microscopic hematuria with dipstick testing is not currently recommended because of theintermittent occurrence of this finding and the low incidence of significant associated urologic disease. Detection of Hematuria
Evaluation of Asymptomatic Microscopic Hematuria in Adults - Septembe.
http://www.aafp.org/afp/AFPprinter/990915ap/1143.html?print=yes
Dipstick Tests for Hematuria
In clinical practice, dipstick urinalysis is the test most
commonly used to detect urinary tract disorders in
asymptomatic patients. In this test, cellulose strips dipped into
myoglobinuria or contamination withmenstrual fluid or oxidizing agents.
a urine specimen record the ability of hemoglobin to catalyze
the reaction between hydrogen peroxide and a chromogen. The
resulting reaction causes the chromogen to turn green, with the
degree of color change directly related to the amount ofhemoglobin present in the urine specimen. A spotted pattern to the dipstick indicates the presence of free
Dipstick testing has been shown to be 91 to 100 percent sensitive and 65 to 99 percent specific for thedetection of hemoglobin. False-positive test results have been reported in the presence of myoglobinuria
and oxidizing 7contaminants (e.g., hypochlorite, povidone and bacterial peroxidases), contamination of theurine specimen with menstrual blood, and dehydration with elevation of urine specific gravity.1,5 False-
negative results have been reported in the presence of reducing agents (e.g., ascorbic acid), a urinary pHof less than 5.1 and dipsticks that have been exposed to air.1,5
Urine Specimen Collection and Preparations
Several factors can influence the microscopic detection oferythrocytes in urine. Procurement of a urine sample using a
catheter may cause urethral trauma that results in variabledegrees of hematuria. A clean-catch midstream urine
specimen should be obtained using aseptic technique to avoidcontamination from the external genitalia. The first urine in the
morning is typically the best specimen because erythrocytesare heat preserved in acidic and concentrated urine. FIGURE 1. Typical morphology of erythrocytes from a urine specimen
A prolonged delay from specimen collection to analysis can
result in a false test interpretation. When a urine specimen
cannot be examined within one hour of collection, it should be
refrigerated to prevent overgrowth of bacteria, changes inurinary pH and disintegration of red and white cell casts.
These conditions may occur if the specimen remains at roomtemperature for a long period.
Standardization of the analysis procedure is also essential to
achieve an accurate result. Centrifugation is typicallyperformed on a fixed volume of urine (5 mL) for five minutes
at 3,000 rotations per minute, after which the supernatant is
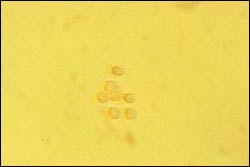
FIGURE 2. Dysmorphic erythrocytes from
poured off and the remaining sediment is resuspended in the
centrifuge tube by gently tapping the bottom of the tube. A
glomerular cause of microscopichematuria. (phase contrast microscopy, 3
pipette is used to sample the residual fluid and transfer it to a
glass slide; a coverslip is applied to the slide for themicroscopic evaluation.5 The specimen is examined under high magnification (3 400) to determine cell
type and distinct morphologic features. Results are recorded as the number of red blood cells perhigh-power field. Findings on Microscopy
On phase contrast microscopy, erythrocytes may display morphologic features that are helpful in
Evaluation of Asymptomatic Microscopic Hematuria in Adults - Septembe.
http://www.aafp.org/afp/AFPprinter/990915ap/1143.html?print=yes
differentiating glomerular and nonglomerular causes of microscopic hematuria8 (Figures 1 and 2).
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of
glomerular origin. Red blood cell casts are also associated with a glomerular cause of hematuria. Acanthocytes, which are ring-formed erythrocytes with one or more membrane protrusions of variable size
and shape, may represent an early form of dysmorphic erythrocytes and are a marker for hematuria ofglomerular origin.
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary
tract origin. Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tractbleeding.
The presence of both dysmorphic and isomorphic erythrocytes in urine represents a mixed morphologic
Diagnosis of Hematuria History and Physical Examination
The initial step in the evaluation of microscopic hematuria is a thorough
medical history, including a review of prescription and nonprescription
medications, a history of ingestion of certain foods and an inquiry for
specific conditions (Tables 1 and 2).9,10
The information obtained in the medical history is used to screen for the
multiple potential causes of both glomerular and nonglomerular conditions Beetsthat can lead to microscopic hematuria (Table 3).11-15 IgA nephropathy
(Berger's disease) is the most common cause of glomerular hematuria.
Drug-induced glomerular causes of hematuria include nonsteroidal
anti-inflammatory drugs and certain antibiotics associated with analgesic
nephropathy and interstitial nephritis (Table 2).9,10
Nitrofurantoin (Furadantin)Phenazopyridine (Pyridium)
One common nonglomerular medical cause of hematuria is papillary
necrosis. This condition should be considered in patients with diabetes
mellitus, black patients with sickle cell trait or disease, and patients
known to be analgesic abusers. Other common nonglomerular causes of
hematuria include urothelial tumors, urolithiasis, benign prostatic
hyperplasia (BPH) and urinary tract infection.
Physician 1989; 40(2):149-56,and Drugdex system.
The physical examination should take into account the multiple potential
Englewood: Colo.:Micromedex, Inc., 1999.
causes of hematuria and include the following points: evaluation of the
cardiovascular system for irregular cardiac rhythm, heart murmur or
hypertension; evaluation of the abdomen for organomegaly or flank mass;evaluation of the prostate and external genitalia; and evaluation of the extremities for peripheral edema,
petechiae or mottling (Table 4).
Urothelial cancers should also be considered in the evaluation of microscopic hematuria. Risk factors forthese malignancies, particularly transitional cell carcinoma, are listed in Table 5.16
Laboratory Tests
The initial laboratory studies are determined by pertinent information obtained from the medical historyand physical examination. Formal urinalysis is performed to document the degree of hematuria, determine
Evaluation of Asymptomatic Microscopic Hematuria in Adults - Septembe.
http://www.aafp.org/afp/AFPprinter/990915ap/1143.html?print=yes
the morphologic features of erythrocytes and evaluate urinary crystals and casts. If pyuria or bacteriuria is
present, a urine culture with sensitivity testing should be obtained to rule out infectious urinary tractpathogens. Screening laboratory tests typically consist of coagulation studies, a complete blood count,
serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medicalhistory.
Further urologic evaluation is warranted if more than three red blood cells per high-power field are found
on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (morethan 100 red blood cells per high-power field) is found on a single urinalysis.17 The only exceptions are
children with persistent microscopic hematuria without proteinuria, in whom the most likely diagnosesinclude thin glomerular basement membrane nephropathy, idiopathic hypercalciuria, IgA nephropathy and
Radiographic Investigation
The initial radiographic study is intravenous pyelography (IVP), or
excretory urography. The purpose of the study is to obtain an
anatomic and functional evaluation of the upper and lower urinary
tract. Before IVP is performed, the collected urine specimen should
undergo microscopic examination to exclude an infectious cause of
hematuria. Some centers use renal ultrasonography as an initial test
Mechanism Drugs
to avoid exposing patients to intravenous contrast media; however,
subtle findings in the renal collecting system may be difficult to
Risk factors for contrast uropathy have been described (Table 6).18
Because preexisting renal insufficiency is the most important risk
factor for renal failure, the serum creatinine concentration should
always be measured before any contrast examination is performed.
Early studies reported a 4.7 percent overall incidence of adverse
reactions to conventional ionic high-osmolar contrast media.19
Although most of these reactions were considered minor, true
anaphylactic reactions have been described. The incidence of death
after the intravenous administration of conventional contrast media
has been reported to be one case per 40,000 contrast-material
injections.19 Newer, nonionic low-osmolar contrast media are
associated with fewer adverse effects than traditional, less
Metformin (Glucophage) is an oral antihyperglycemic agent
commonly used in the management of type 2 diabetes (formerly
termed noninsulin-dependent diabetes). This drug is eliminated
primarily by the kidneys. Because of potential exacerbation of acute
renal failure and lactic acidosis, metformin should be discontinued at Urolithiasis Carbonic anhydrase
the time of radiologic studies involving intravascular administration
of iodinated contrast materials and for 48 hours subsequent to the
prodecure. Current recommendations include withholding metformin
for at least 48 hours before and after the radiographic procedure. The
drug should only be restarted after renal function has been
Evaluation of Asymptomatic Microscopic Hematuria in Adults - Septembe.
http://www.aafp.org/afp/AFPprinter/990915ap/1143.html?print=yes
With excretory urography, tomography is typically performed to
increase recognition of renal masses, fine renal calcifications and
paranephric structures. Oblique images are obtained to assist in
evaluation of ureteral lesions, differentiation of extrinsic and intrinsic NSAIDs = nonsteroidal
renal or ureteral masses and visualization of the posterolateral aspect Information from Restrepo NC,
of the bladder. Delayed images are helpful in cases of obstruction in Carey PO. Evaluating hematuria inwhich the nephrogram phase is seen on IVP but the collecting system adults. Am Fam Physician 1989;is not yet visualized.18
40(2):149-56, and Drugdex system. Englewood: Colo.: Micromedex,
If the use of intravenous contrast material is contraindicated or if
incomplete visualization of the lower urinary tract occurs, retrograde
pyelography should be performed. Typically, the combination ofretrograde pyelography and ultrasonography is employed to increase sensitivity in the detection of solid
renal masses. However, renal ultrasonography cannot detect the subtle mucosal abnormalities that occurwith transitional cell carcinoma or small, echogenic ureteral calculi. Compared with renal ultrasonography,
computed tomography (CT) is more sensitive in detecting renal masses and subtle filling defects of therenal collecting system.22 Recently, unenhanced helical CT scans have provided accurate evaluation of
patients with acute flank pain through the precise determination of calculus size and location.23 Despiteadvancements in radiographic imaging, the role of CT or ultrasonography as the primary imaging modality
in the work-up of microscopic hematuria has not been established. Lower Urinary Tract Investigation Whereas radiographic imaging allows evaluation of the upper urinary tract, cystourethroscopy provides
definitive evaluation of the lower urinary tract. In addition to direct visualization of the urethra, prostateand bladder, washings and biopsies of suspicious bladder lesions can be performed during
Cytology obtained from washings is useful in detecting poorly differentiated sessile and in situ bladderlesions. With in situ bladder cancer, the results of cytologic analysis are often positive before lesions are
TABLE 3 Glomerular and Nonglomerular Causes of Hematuria Glomerular causes Nonglomerular causes
Vascular disorders (nutcracker syndrome,15
malignant hypertension, sickle cell trait or
thrombosis or infarct, transplant rejection)
Familial condition (polycystic kidney disease,
Infection (acute or chronic pyelonephritis,
Evaluation of Asymptomatic Microscopic Hematuria in Adults - Septembe.
http://www.aafp.org/afp/AFPprinter/990915ap/1143.html?print=yes
Infections (cystitis, prostatitis, urinary
Systemic bleeding disorder or coagulopathy
Drugs (heparin, warfarin [Coumadin],cyclophosphamide [Cytoxan])
Adapted with permission from Ahmed Z, Lee J. Asymptomatic urinary abnormalities. Hematuria and proteinuria. Med Clin North Am 1997;81:641-52; additional information fromreferences 12 through 15. Other Investigations
When no cause for microscopic hematuria is found with cystourethroscopy and appropriate radiographicimaging, further studies may be considered. These studies include CT scanning, renal angiography and
flexible ureterorenoscopy. No consensus has been reached on the indications for renal biopsy in patientswith hematuria, but this procedure may be indicated to rule out glomerular causes of hematuria.1 Despite a
complete and exhaustive work-up, no specific cause is identified in approximately 20 percent of patientswith microscopic hematuria.24
Molecular markers recently introduced into clinical practice to Concurrent metformin (Clucophage)
assist with the follow-up evaluation of urothelial carcinomas
ingestion may precipitate lactic acidosis
have yet to be labeled for the evaluation of hematuria. The two and cute renal failure inassays currently labeled for clinical use by the U.S. Food and
patientsundergoing intravenouspyelography with iodinated contrast
Drug Administration are the bladder tumor antigen (BTA) test
and the nuclear matrix protein (NMP-22) test.17,25 The BTA testis a latex agglutination assay for the qualitative detection of a
basement membrane antigen in a voided urine specimen. The NMP-22 test involves the quantitativedetection of a specific nuclear matrix protein in a voided urine specimen. Although these assays offer
great potential for the early detection of recurrent bladder carcinoma, their role in the evaluation ofhematuria is still uncertain.
A standard reference algorithm for the evaluation and treatment of asymptomatic microscopic hematuria is
presented in Figure 3. This systematic approach can be useful in identifying and managing causes ofhematuria ranging from infection to BPH26 to cancer.
Evaluation of Asymptomatic Microscopic Hematuria in Adults - Septembe.
http://www.aafp.org/afp/AFPprinter/990915ap/1143.html?print=yes
Physical examination Cause of hematuria
associated with urinary calculi and obstruction
Information from Messing EM, Catalona W.
Urothelial tumors of the urinary tract. In:
Walsh PC, ed. Campbell's Urology. 7th ed.
Philadelphia: Saunders, 1998:2327-410.
Enlarged prostate Urinary tract infection
Special Considerations Hematuria During Anticoagulation
Microscopic hematuria is commonly encountered inpatients taking anticoagulant drugs. Although it may be
easy to attribute this hematuria solely to anticoagulation
therapy, significant urologic causes have been reported in
13 to 45 percent of such patients.27,28 Current
recommended anticoagulation schedules do not
predispose patients to hematuria.27 The most common
causes of anticoagulant-associated hematuria include
BPH, inflammatory conditions, urolithiasis, papillary
necrosis and cancers of the upper and lower urinary tract.
Seafood allergyOthers, including allergic reactions to
Hematuria Following Exercise
Asymptomatic microscopic hematuria resulting from
strenuous exercise has been well documented in
association with a variety of contact and noncontact sportsactivities.12-14 The degree of hematuria is believed to be
Information from Friedenberg RM. Excretory
related to the intensity and duration of exercise.12
urography in the adult. In: Walsh PC, ed.
Although exercise-induced hematuria is typically a benign, Campbell's Urology. 6th ed. Philadelphia:
self-limited process, coexisting urinary tract pathologymay exist and must be carefully excluded.
Evaluation of Asymptomatic Microscopic Hematuria in Adults - Septembe.
http://www.aafp.org/afp/AFPprinter/990915ap/1143.html?print=yes
Exercise-induced microscopic hematuria almost always resolves within 72 hours of onset in patients who
do not have underlying urinary tract abnormality. However, if the hematuria is present on repeat urinalysisafter 72 hours of rest, further urologic evaluation may be indicated. Final Comment
Asymptomatic microscopic hematuria is commonly nephric in origin, whereas gross hematuria is often
uroepithelial in origin. Gross, painless hematuria is often the first manifestation of a urothelial tumor. However, the degree of hematuria bears no relation to the seriousness of the underlying disease.
Consequently, the microscopic finding of blood in the urine should be considered a serious symptom untilsignificant pathology has been excluded.
Phase contrast microscopy is currently the best initial method of documenting microscopic hematuria. The
evaluation often includes intravenous pyelography, cystourethroscopy and urinary cytology.
Unfortunately, consensus is lacking regarding the management of persistent asymptomatic microscopichematuria of unknown etiology. Recommended surveillance schedules for patients with a previous
negative evaluation for unexplained microscopic hematuria include urinalysis and voided urinary cytologyannually until the hematuria resolves, or for up to three years if microscopic hematuria persists. Any
significant increase in the degree of microscopic hematuria (more than 50 red blood cells per high-powerfield), an episode of gross hematuria or the new onset of irritative voiding symptoms in the absence of
infection warrants a complete reevaluation.17
Additional large population-based studies of the prevalence of asymptomatic microscopic hematuria andits relationship with age and sex are needed before definitive recommendations can be formalized to
Hematuria
Evaluation of Asymptomatic Microscopic Hematuria in Adults - Septembe.
http://www.aafp.org/afp/AFPprinter/990915ap/1143.html?print=yes
FIGURE 3. Algorithm for the evaluation and treatment of hematuria. (RBC = red blood cell; WBC = white blood cell; BUN = blood urea nitrogen; CBC = complete blood count; PT = prothrombin time; PTT = partial thromboplastin time; IVP = intravenous pyelography; KUB = plain radiograph of kidney, ureter and bladder; CT = computed tomography; TURP = transurethral resection of the prostate) The Authors
is currently in private practice at Statesboro Urologic Clinic, P.C., Statesboro, Ga. He received hismedical degree from Louisiana State University School of Medicine in Shreveport and completed a
residency in urology at the University of Kansas Medical Center, Kansas City, Kan., where he served aschief resident.
is in private practice at Valley Urology Center, Renton, Wash. Dr. Wang completed a residency in urologyat the University of Minnesota, Minneapolis, and a fellowship in endourology at Baylor College of
Evaluation of Asymptomatic Microscopic Hematuria in Adults - Septembe.
http://www.aafp.org/afp/AFPprinter/990915ap/1143.html?print=yes
Address correspondence to Timothy R. Thaller, M.D., Statesboro Urologic Clinic, P.C., 412 NorthsideDrive East, Suite 300, Statesboro, GA 30458. Reprints are not available from the authors.
The authors thank Nicolle M. DiGerolamo-Thaller, R.N., B.S.N., for assistance in the preparation of the
manuscript, Scott M. Stanley for assistance in the laboratory and with preparation of the photomicrographs
and Sue Ulrich, R.Ph., for assistance in the preparation of pharmacologic tables in the manuscript.
1. Sutton JM. Evaluation of hematuria in adults. JAMA 1990;263:2475-80.
2. Mohr DN, Offord KP, Owen RA, Melton LJ 3d. Asymptomatic microhematuria and urologic disease. A
population-based study. JAMA 1986;256: 224-9.
3. Messing EM, Young TB, Hunt VB, Emoto SE, Wehbie JM. The significance of asymptomatic microhematuria in
men 50 or more years old: findings of a home screening study using urinary dipsticks. J Urol 1987;137:919-22.
4. Britton JP, Dowell AC, Whelan P, Harris CM. A community study of bladder cancer screening by detection of
occult urinary bleeding. J Urol 1992; 148:788-90.
5. Fogazzi GB, Ponticelli C. Microscopic hematuria diagnosis and management. Nephron 1996;72: 125-34.
6. Brender CB. Evaluation of the urologic patient. In: Walsh PC, ed. Campbell's Urology. 7th ed. Philadelphia:
7. Woolhandler S, Pels RJ, Bor DH, Himmelstein DU, Lawrence RS. Dipstick urinalysis screening of asymptomatic
adults for urinary tract disorders. I. Hematuria and proteinuria. JAMA 1989;262: 1214-9.
8. Fairley KF, Birch DF. Hematuria: a simple method for identifying glomerular bleeding. Kidney Int 1982;21:105-8.
9. Restrepo NC, Carey PO. Evaluating hematuria in adults. Am Fam Physician 1989;40(2):149-56.
10. Drugdex system. Englewood: Colo.: Micromedex, Inc., 1999. Accessed Sept. 24, 1998.
11. Ahmed Z, Lee J. Asymptomatic urinary abnormalities. Hematuria and proteinuria. Med Clin North Am
12. Abarbanel J, Benet AE, Lask D, Kimche D. Sports hematuria. J Urol 1990;143:887-90.
13. Gambrell RC, Blount BW. Exercise-induced hematuria. Am Fam Physician 1996;53:905-11.
14. Jones GR, Newhouse I. Sport-related hematuria: a review. Clin J Sport Med 1997;7:119-25.
15. Hohenfellner M, Steinbach F, Schultz-Lampel D, Schantzen W, Walter K, Cramer BM, et al. The nutcracker
syndrome: new aspects of pathophysiology, diagnosis and treatment. J Urol 1991;146: 685-8.
16. Messing EM, Catalona W. Urothelial tumors of the urinary tract. In: Walsh PC, ed. Campbell's Urology. 7th ed.
Philadelphia: Saunders, 1998:2327-410.
17. Mariani AJ. The evaluation of adult hematuria: a clinical update. AUA Update Series 1998;XVII:186-91.
18. Friedenberg RM. Excretory urography in the adult. In: Walsh PC, ed. Campbell's Urology. 6th ed. Philadelphia:
19. Dunnick NR, Sandler CM, Amis ES Jr, Newhouse JM. Functional renal anatomy, renal physiology, and contrast
media. In: Mitchell CW, ed. Textbook of uroradiology. 2d ed. Baltimore: Williams & Wilkins, 1997:86-115.
20. Keizur JJ, Das S. Intravascular contrast media in urologic imaging. AUA Update Series 1996;XV: 102-7.
21. Physicians' desk reference. 54th ed. Montvale, N.J.: Medical Economics, 2000:833.
22. Warshauer DM, McCarthy SM, Street L, Bookbinder MJ, Glickman MG, Richter J, et al. Detection of renal masses:
sensitivities and specificities of excretory urography/linear tomography, US, and CT. Radiology 1988;169:363-5.
23. Dalrymple NC, Verga M, Anderson KR, Bove P, Covey AM, Rosenfield AT, et al. The value of unenhanced helical
computerized tomography in the management of acute flank pain. J Urol 1998; 159:735-40.
24. Corwin HL, Silverstein MD. The diagnosis of neoplasia in patients with asymptomatic microscopic hematuria: a
decision analysis. J Urol 1988;139: 1002-6 [Published erratum in J Urol 1988;140: 1558].
25. Landman J, Chang Y, Kavaler E, Droller MJ, Liu BC. Sensitivity and specificity of NMP-22, telomerase, and BTA
in the detection of human bladder cancer. Urology 1998;52:398-402.
26. Sieber PR, Rommel FM, Huffnagle HW, Breslin JA, Agusta VE, Harpster LE. The treatment of gross hematuria
Evaluation of Asymptomatic Microscopic Hematuria in Adults - Septembe.
http://www.aafp.org/afp/AFPprinter/990915ap/1143.html?print=yes
secondary to prostatic bleeding with finasteride. J Urol 1998;159:1232-3.
27. Culclasure TF, Bray VJ, Hasbargen JA. The significance of hematuria in the anticoagulated patient. Arch Intern
28. Van Savage JG, Fried FA. Anticoagulant associated hematuria: a prospective study. J Urol 1995;153: 1594-6.
Copyright 1999 by the American Academy of Family Physicians.
This content is owned by the AAFP. A person viewing it online may make one printout of the material and may use that
printout only for his or her personal, non-commercial reference. This material may not otherwise be downloaded,
copied, printed, stored, transmitted or reproduced in any medium, whether now known or later invented, except as
September 15, 1999 Contents | AFP Home Page | AAFP Home | Search
S A F E T Y D A T A S H E E T C A F FE IN E C IT R A T E 1 . I D E N T I FI C A T I O N O F T H E S U B ST A N C E /P R E P A R A T I O N A N D T H E C O M P A N Y : P R O D U C T N A M E : C H EM I C A L N A M E 2 : 1,3,7-Trimethyl-1,2,6-tetrahydropurine, 2-hydroxy-1,2,3-propantricarbonic acid (1:1) P A R T N o .: S U P P L IE R : J M Loveridge plcSouthbrook Road, Southampt
Volume 29 Number 1 Spring 2002 Inland Waterways News Weil's Disease (Leptospirosis) Dr John Fleetwood Weil's Disease has been in the news recently. It is the most serious form of a group of illnesses known collectively as leptospirosis. When one examines the leptospirosis germs under a microscope, they look rather like corkscrews which wriggle actively



 Evaluation of Asymptomatic Microscopic Hematuria in Adults - Septembe.
Evaluation of Asymptomatic Microscopic Hematuria in Adults - Septembe.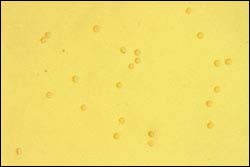
 Evaluation of Asymptomatic Microscopic Hematuria in Adults - Septembe.
Evaluation of Asymptomatic Microscopic Hematuria in Adults - Septembe.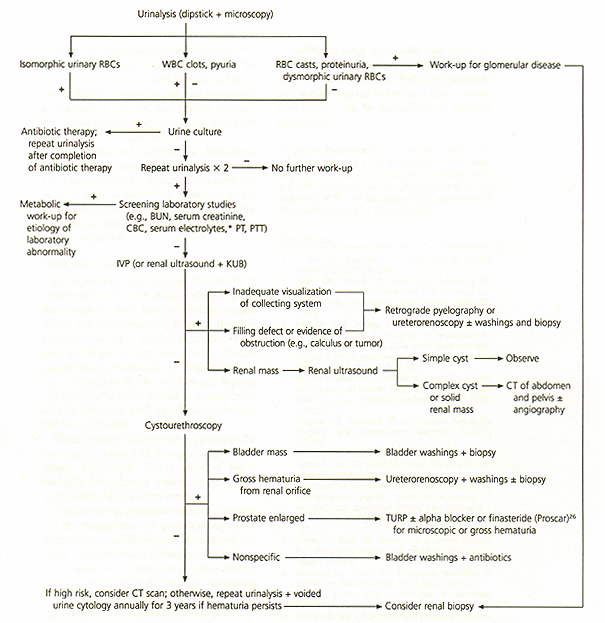 Evaluation of Asymptomatic Microscopic Hematuria in Adults - Septembe.
Evaluation of Asymptomatic Microscopic Hematuria in Adults - Septembe.