Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Lup-07086503 281.288
Previous antimalarial therapy in patients diagnosed with lupus nephritis: Influence on outcomes and survival
A Sisó, M Ramos-Casals, A Bové, P Brito-Zerón, N Soria, S Muñoz, A Testi, J Plaza, J Sentís and A Coca
The online version of this article can be found at:
http://lup.sagepub.com/cgi/content/abstract/17/4/281
can be found at: Lupus Additional services and information for Citations
Previous antimalarial therapy in patients diagnosed
with lupus nephritis: Influence on outcomes and survival
A Sisó1,2, M Ramos-Casals1, A Bové1, P Brito-Zerón1, N Soria1, S Muñoz1, A Testi1, J Plaza1, J Sentís3 and A Coca4
1Department of Autoimmune Diseases, Laboratory of Autoimmune Diseases “Josep Font”, Institut d’Investigacions Biomèdiques August Pi i Sunyer
(IDIBAPS), Statistical Unit, Barcelona, Spain; 2Centre d’Assistència Primària ABS Les Corts, GESCLINIC, Barcelona, Spain; 3Department of Public
Health, School of Medicine, University of Barcelona, Barcelona, Spain; and 4Hypertension Unit, Institut Clínic de Medicina i Dermatologia, Hospital
The aim of this study was to analyze the effect of exposure to antimalarial drugs at diagnosis oflupus nephritis on the outcome of the disease, especially renal failure, comorbid processes, andsurvival. We analyzed a cohort of 206 consecutive patients with biopsy-proven lupus nephritis. Renal biopsies were categorized according to the classification proposed by the ISN/RPS in 2003. Exposure to antimalarial drugs (chloroquine and hydroxychloroquine) was defined as the use ofthese drugs before the diagnosis of lupus nephritis independent of dose and duration. Fifty-six(27%) patients had received antimalarials before the diagnosis of lupus nephritis. During thefollow-up, these patients had a lower frequency of creatinine values >4 mg/dL (2% vs 11%,P = 0.029) and end-stage renal failure (2% vs 11%, P = 0.044) in comparison with those nevertreated with antimalarials. Patients exposed to antimalarials also had a lower frequency of hyper-tension (32% vs 50%, P = 0.027), infections (11% vs 29%, P = 0.006), and thrombotic events (5% vs17%, P = 0.039). Twenty patients (10%) died during the study period. Patients exposed to antima-larials had a lower mortality rate at the end of the follow-up (2% vs 13% for those not exposed toantimalarials, P = 0.029). Multivariate analysis identified thrombosis and infections as statisticallysignificant independent variables. Kaplan–Meier plots showed a lower rate of end-stage renal fail-ure (log rank = 0.04) in patients exposed to antimalarials. In conclusion, exposure to antimalarialsbefore the diagnosis of lupus nephritis was negatively associated with the development of renalfailure, hypertension, thrombosis and infection, and with a better survival rate at the end of thefollow-up. This, together with other published data, suggests that antimalarials should be consid-ered a mandatory therapeutic option in all patients diagnosed with systemic lupus erythemato-sus.
Key words: antimalarials; cardiovascular disease; hydroxychloroquine; lupus nephropathy;mortality; systemic lupus erythematosus; thrombosis
bidity and mortality of the overwhelmingly youngfemale population with SLE. Patients with glomerulo-
Systemic lupus erythematosus (SLE) is considered the
nephritis have a higher mortality rate in comparison
most clinically and serologically diverse systemic auto-
with those without renal involvement, and nearly 10%
immune disease because it may affect any organ with
of patients with lupus nephritis (LN) develop end-
a broad spectrum of manifestations. The disease
mainly involves the skin, joints, kidneys, blood cells,
and nervous system,1 and the diversity of clinical and
After decades of empirical use, antimalarial drugs
analytical features lead to very different forms of pre-
(chloroquine and hydroxychloroquine) are currently
sentation. Renal disease plays a key role in the prog-
considered as a key therapy in SLE. The use of anti-malarials has been associated with a decreased risk of
nosis of SLE and contributes significantly to the mor-
developing lupus flares and thrombotic events,4–6 less-accrued chronic damage, and a better survival rate in
Correspondence to: Dr Manuel Ramos-Casals, Servei de Malalties
comparison with patients not treated with these drugs,
Autoimmunes, Hospital Clínic, C/Villarroel, 170, 08036-Barcelona, Spain.
even after adjusting for patient characteristics. How-
E-mail: mramos@clinic.ub.esReceived 27 August 2007; accepted 25 October 2007
ever, the possible beneficial effects of antimalarial
2008 SAGE Publications Los Angeles, London, New Delhi and Singapore
Antimalarials and outcomes of lupus nephritis
drugs in patients diagnosed with LN have not yet been
Chronic renal failure, defined as raised creatinine
levels (>2 mg/dL in two consecutive analytical
We analyze the influence of exposure to antimalar-
determinations, separated by at least 3 months).
ials at LN diagnosis in the outcome of 206 patients
We also recorded creatinine levels higher than
followed in a single reference center, especially renal
4 mg/dL. End-stage renal failure was defined as
failure, comorbid processes [cardiovascular disease
the need for dialysis or renal transplantation.
(CVD), infections, and neoplasia] and survival.
Cardiovascular risk factors, including hyperten-sion
>140 mmHg and/or diastolic blood pressure
>90 mmHg in two or more consecutive visits), dys-lipidemia (hypercholesterolemia – total cholesterolhigher than 250 mg/dL – and/or hypertriglyceride-
mia – triglycerides higher than 150 mg/dL), and/or
Patients with SLE consecutively followed in our
diabetes mellitus (fasting glycemia higher than
department from 1970 until 2006 were evaluated. All
126 mg/dL in at least two determinations).
patients fulfilled the 1997 revised criteria for the clas-
Cardiovascular events, including cerebrovascular
sification of SLE.7 Of this cohort, patients with
accident (confirmed by computed tomography
biopsy-proven LN were selected as the study popula-
and/or magnetic resonance imaging scans) or ische-
tion. Renal biopsies were reviewed by two patholo-
mic heart disease (confirmed clinically by elevatedcardiac enzyme levels and/or electrocardiogram).
gists and categorized according to the recent classifi-
Thrombotic events, including deep vein thrombo-
cation proposed by the ISN/RPS in 20048: class I
sis (confirmed by Doppler studies and/or phlebo-
(minimal mesangial LN), class II (mesangial prolifer-
graphy), pulmonary embolism (diagnosed by ven-
ative LN), class III (focal LN), class IV (diffuse LN),
tilation/perfusion pulmonary scintigraphy), and/or
class V (membranous LN), and class VI (advanced
peripheral arterial thrombosis (diagnosed by
sclerosing LN). The time of LN diagnosis, defined as
the point when the first (diagnostic) renal biopsy was
Infections, defined according to a previous report.11
performed, was the starting point for the follow-up in
Complications related to the use of corticosteroids,
all patients. All patients were prospectively followed
including osteopenia, osteoporosis, Cushing dis-
with regular visits at 6 to 12-month intervals. The indi-
vidual follow-up for each patient was measured from
the time of LN diagnosis until the last hospital visit,
transfer out or death. Clinical and laboratory datawere collected and computerized according to ourstandard department protocol.9 The design of the
study conformed to the ethical standards currently
Categorical data were compared using the chi-squared
applied in Spain. Because of the anonymous nature
and Fisher’s exact tests. Continuous variables were
of the study, informed patient consent was not
analyzed with the Student’s t-test in large samples of
similar variance and with the nonparametric Mann–
Exposure to antimalarial drugs (chloroquine and
Whitney U-test for small samples, with results indi-
hydroxychloroquine) was defined as the use of these
cated as mean ± standard error of the mean (SEM). A
drugs before the diagnosis of LN independent of dose
two-tailed value of P < 0.05 was taken to indicate sta-
and duration, according to the definition used by
tistical significance. When several independent vari-
Alarcón et al.10; exposure was recorded as present if
ables appeared to have statistical significance in the
documented at the time of the diagnosis of LN or
univariate analysis, a multiple logistic regression anal-
when antimalarials had been administered at least
ysis was performed, taking the dichotomized variable
50% of the period between the diagnosis of SLE and
exposure to antimalarial drugs (yes/no) as the depen-
the diagnosis of LN. None of our patients had
dent variable and those variables that were statistically
received more than 400 mg of hydroxychloroquine
significant in the univariate analysis as independent
variables. The multivariate analysis was adjusted byage at diagnosis of LN, gender, length of follow-up,and the variables that were statistically significant
when the baseline characteristics of patients treated
The following outcomes were recorded during the
with antimalarials or not were compared. A multivar-
iate Cox regression analysis using a backward step-
Antimalarials and outcomes of lupus nephritisA Sisó, et al.
wise method allowing adjustment for age, gender,
diagnosis of 27.73 ± 3.79 months. Renal biopsies
length of follow-up and development of cardiovascu-
showed class IV in 81 (39%) patients, class III in 49
lar events, and end stage renal failure was used to
(24%), class II in 34 (16%), class V in 31 (15%), class I
evaluate the effect of antimalarial exposure at LN
in eight (4%), and class VI in three (2%) patients.
diagnosis on survival. The hazard ratios (HRs) and
Induction therapy included oral prednisone at a dose
their 95% confidence intervals (CIs) obtained in the
of 1 mg/kg/day in 174 (84%) patients and intravenous
adjusted regression analysis were calculated. The
results of the analysis of continuous variables are indi-cated as mean ± SEM. Kaplan–Meier survival curves
Comparison according to antimalarial exposure
for the development of chronic renal failure and deathwere compared using the log-rank and Breslow tests.
We classified patients with LN into two groups:
The statistical analysis was performed using the SPSS
patients who never received antimalarial therapy
(n = 150) and those who had received antimalarials(n = 56) before the diagnosis of LN. We comparedthe main baseline epidemiological, clinical, and immu-
nological features at LN diagnosis (Table 1). Patientsnever treated with antimalarials had a shorter meantime of SLE evolution (28.98 vs 31.29 months,
P = 0.001), a higher prevalence of previous corticoste-
A total of 206 patients (185 women and 21 men, 95%
roid treatment (58% vs 32%, P < 0.001), and a higher
Caucasian) with LN were included. The mean age at
frequency of raised levels of creatinine at LN diagno-
SLE diagnosis was 30.0 years (SEM 0.88, range 8–67)
sis (23% vs 11%, P = 0.05) in comparison with
and 31.3 years (SEM 0.32, range 8–67) at diagnosis of
patients treated with antimalarials, although only pre-
LN, with a mean time of evolution of SLE until LN
Baseline characteristics at diagnosis of lupus nephritis of patients treated or not with antimalarials
Antimalarial exposure before the diagnosis of LN
Previous treatment with immunosuppressant
Abbreviations: LN: lupus nephritis; SLE: systemic lupus erythematosus; dsDNA: double stranded DNA. *Statistically significant in multivariate analysis.
Antimalarials and outcomes of lupus nephritis
independent variable in the multivariate analysis. No
treated with antimalarials. Thus, patients exposed to
significant differences were found in the comparison
antimalarials had a lower mortality rate at the end of
of the main epidemiological features, LN classes,
the follow-up (2% vs 13% for those not exposed to
immunological markers at LN diagnosis or induction
antimalarials, P = 0.029). The causes of death are
shown in Table 3. Overall, infections were the mostfrequent causes of death in patients not exposed to
antimalarials, followed by renal failure, CVD, andneoplasia. In the patient treated with antimalarials
At the end of follow-up (mean follow-up 148 months),
who died, death was due to primary pulmonary
patients treated with antimalarials had a lower fre-
quency of creatinine values >4 mg/dL (2% vs 11%,
Multivariate analysis adjusted by age, gender,
P = 0.044) and end-stage renal failure (end-stage
length of follow-up, and the significant variables
renal disease, ESRD) (2% vs 11%, P = 0.029) in com-
from Table 1 identified thrombosis (P = 0.014) and
parison with those never treated with antimalarials
infections (P = 0.03) as statistically significant inde-
(Table 2). With respect to CVD, patients exposed to
pendent variables associated with antimalarial expo-
antimalarials had a lower frequency in the develop-ment of cardiovascular risk factors, especially arterialhypertension (32% vs 50%, P = 0.027), and a lower
Cardiovascular events and causes of death in patients
frequency of cardiovascular events in comparison
treated or not with antimalarials before the diagnosis of LN
with those never treated with antimalarials, although
the difference was not statistically significant (9% vs
15%, P = 0.264). Patients exposed to antimalarials
before LN diagnosis also had a lower frequency ofcomorbid complications, especially infections (11%
vs 29%, P = 0.006) and thrombotic events (5% vs
Twenty patients (10%) died during the study
period. Mean age at the time of death was
46.5 ± 4.13 years, with a mean follow-up to death of
154.60 ± 23.66 months. Nineteen of the 20 deaths
(95%) occurred in patients who had never received
antimalarials, compared with only one (5%) patient
Abbreviation: LN: lupus nephropathy; APS: antiphospholipid syndrome.
Outcomes of patients with lupus nephropathy treated or not with antimalarials before the diagnosis of LN
Antimalarial exposure before the diagnosis of LN
Abbreviation: LN: lupus nephritis. aPatients with creatinine >2 mg/dL at diagnosis of LN were not included. bPatients with creatinine >4 mg/dL at diagnosis of LN were not included. *Significant independent variables in the adjusted multivariate analysis.
Antimalarials and outcomes of lupus nephritisA Sisó, et al.
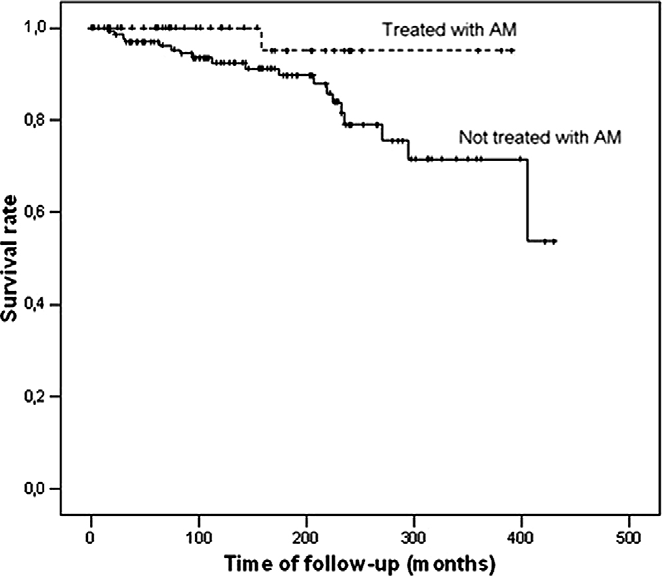
antimalarial exposure (P = 0.042, HR 0.233, CI 95%0.051–0.981) and gender (P = 0.016, HR 0.225, CI95% 0.072–0.706) for survival.
The course of LN is difficult to predict for variousreasons, including the heterogeneity of its clinical pre-sentation, the different classification criteria, the inci-dence of histological transformation, and the differenttherapeutic schedules used.12 No single factor seems tobe determinant in estimating the prognosis of LN, anda range of demographic, clinical, laboratory, and his-topathological parameters are usually used to analyzethe prognosis and response to therapy.13
Antimalarials are a long-standing safe, inexpensive
therapy for SLE. Reports have shown that antimalar-ials are effective in controlling mild/moderate SLE.13,14
Kaplan–Meier plots showing end-stage renal failure in
Recent studies from the Hopkins Lupus15 and
patients with lupus nephritis (LN) treated (dotted line) or not
LUMINA cohorts5 suggest that hydroxychloroquine
(continuous line) with antimalarials before the diagnosis of LN(log rank = 0.04).
may have a long-term protective effect on SLE-relatedorgan damage. In addition, Costedoat-Chalumeauet al.16 have recently reported that low whole-bloodhydroxychloroquine concentrations are a strong pre-dictor of SLE exacerbation, whereas the randomizeddiscontinuation trial by the Canadian Hydroxychloro-quine Study Group17 found that the relative risk ofsevere SLE exacerbation in patients who discontinuedhydroxychloroquine was six times greater than thatobserved in those who continued hydroxychloroquine. A possible etiopathogenic explanation could be basedin the capacity of antimalarials to inhibit the activationof intracellular toll-like receptors.18
Few studies have supported a role for antimalarial
therapy in severe SLE involvement such as vasculitis,central nervous system involvement, or nephritis. Ourresults show that patients treated with antimalarialsbefore the diagnosis of LN had a fivefold lower prev-alence of end-stage renal failure at the end of thefollow-up in comparison with patients never treatedwith antimalarials. This suggests that the use of anti-
Kaplan–Meier plots showing survival rates of patients
malarials before the diagnosis of LN may be a protec-
with lupus nephritis (LN) treated (dotted line) or not (continuousline) with antimalarials before the diagnosis of LN (log
tive factor for the development of further renal failure.
Some recent studies have suggested beneficial effectsfor antimalarials in patients with LN. Kasitanonet al.19 found that the concurrent use of hydroxychlor-
sure. Figures 1 and 2 show Kaplan–Meier plots for
oquine has a statistically significant positive effect on
end-stage renal failure (log rank = 0.04) and the sur-
renal remission in patients with membranous LN trea-
vival rate (log rank = 0.07) of patients treated or not
ted with mycophenolate. In a follow-up study by the
with antimalarials at the time of the diagnosis of LN,
Canadian Hydroxychloroquine Study Group,20 the
respectively. Multivariate Cox regression analysis
rate of nephritis flares was reduced by 74% in patients
identified antimalarial exposure as statistically signifi-
who continued on hydroxychloroquine, although the
cant independent variable (P = 0.05, HR 0.294, CI
difference was not statistically significant in compari-
95% 0.026–1.009) for the development of ESRD and
son with those who discontinued the drug. Barber
Antimalarials and outcomes of lupus nephritis
et al.21 found that patients with LN with sustained
the addition of chloroquine to conventional treatment
remission were more likely to have been treated with
hydroxychloroquine than those who did not attain
improved survival in patients with glioblastoma multi-
forme. A recent data has also suggested a possible
Antimalarials not only have anti-inflammatory
protective effect for antimalarials in the development
of neoplasia in patients with SLE. Ruiz-Irastorza
et al.30 found a prevalence of neoplasia of 13% in
hyperglycemic effects.4,22,23 We found a lower fre-
patients never treated with antimalarials in compari-
quency of CVD in patients exposed to antimalarials,
son with 1.3% in those who had received antimalar-
including both risk factors and events. Similar results
ials, with an adjusted hazard ratio for cancer of 0.15.
were found by Bessant et al.,24 who reported that SLE
Interestingly, none of our patients with LN exposed to
patients with CVD were less likely to have received
antimalarials developed neoplasia during the follow-
treatment with hydroxychloroquine than those with-
up, in comparison with five (3%) of those not exposed.
out CVD. Our results showed a modest effect of anti-
After a mean follow-up of more than 12 years, only
malarials in reducing diabetes or dyslipidemia in our
one of our 56 patients with LN exposed to antimalar-
LN patients compared with the effect found in
ials died, in comparison with 19 of the 150 patients not
patients with rheumatoid arthritis25 or other SLE
exposed, a sevenfold difference. A recent study by
populations.26,27 This may be due to the lower preva-
Alarcón et al.10 showed that hydroxychloroquine
lence of diabetes and dyslipidemia found in our
exerts a clear protective effect in terms of survival
patients. In contrast, we found a significant reduction
regardless of whether clinical and socio-demographic
in the development of hypertension during the follow-
characteristics are taken into consideration. Ruiz-
up of our patients with LN, suggesting that the pre-
Irastorza et al.30 also found that the majority of deaths
diagnostic use of antimalarials in patients with LN
in their SLE cohort occurred in patients who were
may play a protective role against the development
never treated with antimalarials. This protective role
of one of the main cardiovascular complications
of antimalarials in the survival of patients with SLE is
probably due to their effect in preventing flares and
Ruiz-Irastorza et al.6 have recently suggested that
limiting accrued chronic damage, both factors closely
antimalarials may have a protective effect against
related to mortality.5,15,31,32 We also found that our
thrombosis in patients with SLE, results which we
patients exposed to antimalarials had a lower fre-
confirmed. During the follow-up, our patients with
quency of the main adverse outcomes associated
LN exposed to antimalarials had three-times less
with LN (renal failure, CVD, infections, and neopla-
thrombotic events than those never exposed to anti-
sia). Logically, this is reflected by the increased sur-
malarials. These results suggest the possible use of
vival in these patients, none of whom died of causes
antimalarials as a safe, effective option in both pri-
related to renal or CVD, infections, or neoplasia.
mary and secondary prophylaxis of thrombosis in
This uncontrolled, retrospective study has some
patients with antiphospholipid syndrome, either pri-
limitations. As it was an observational cohort study,
treatment allocation was based only on the clinical
We also found that patients exposed to antimalar-
judgement of the treating physician. As a result, the
ials had nearly two-third less infections during the
observed effects attributed to antimalarials may be
follow-up than those not exposed, a difference that
biased by confounding variables that could influence
was statistically significant in the adjusted multivari-
the treatments administered. In addition, the possible
ate analysis. In addition, exposure to antimalarials
influence of exposure to antimalarials subsequent to
was associated with a lower frequency of complica-
the diagnosis of LN was not analyzed, although more
tions related to the corticosteroid use, although the
than 95% of patients were taking antimalarials at the
difference was not statistically significant. Thus, the
last study visit. A statistical approach using a time-
pre-diagnostic use of antimalarials in patients with
dependent analysis would have being more convincing
LN might prevent the side effects associated with the
and the results more solid. In spite of these limitations,
prolonged use of corticosteroids, such as metabolic
the importance of performing observational studies
alterations or osteonecrosis (as recently suggested by
analyzing large cohorts of ‘real-world’ patients with
Calvo-Alén et al.28) and the high susceptibility to
In conclusion, this study shows that exposure to
Recent data point to a potential influence for anti-
antimalarials before the diagnosis of LN is negatively
malarials in the development of malignancies. In a
associated with the development of the main adverse
randomized clinical trial, Sotelo et al.29 showed that
outcomes during the follow-up of patients with SLE.
Antimalarials and outcomes of lupus nephritisA Sisó, et al.
Protective effects of antimalarials in patients with SLE: studies published in the last 5 years
Protection against thrombosisIncreased survival
Increased clearance of low-density lipoprotein
Protection against end-stage renal failureLower risk of developing HTAProtection against thrombosisProtection against infectionsIncreased survival
Abbreviations: SLE: systemic lupus erythematosus; LN: lupus nephropathy; MLN: membranous LN; HTA: hypertension.
The protective effect was especially significant for end-
8 Weening, JJ, D’Agati, VD, Schwartz, MM, et al. International
stage renal failure, hypertension, thrombosis, and
Society of Nephrology Working Group on the Classification ofLupus Nephritis, Renal Pathology Society Working Group on the
infection and was associated with a better survival
Classification of Lupus Nephritis. The classification of glomerulone-
rate at the end of the follow-up. This, together with
phritis in systemic lupus erythematosus revisited. Kidney Int 2004; 65:
other published data (Table 4), suggests that antima-
9 Font, J, Cervera, R, Ramos-Casals, M, et al. Clusters of clinical and
larials should be considered a mandatory therapeutic
immunologic features in systemic lupus erythematosus: analysis of 600
option in all patients diagnosed with SLE.
patients from a single center. Semin Arthritis Rheum 2004; 33: 217–230.
10 Alarcon, GS, McGwin, G, Bertoli, AM, et al. for the LUMINA
Study Group. Effect of hydroxychloroquine on the survival of
patients with systemic lupus erythematosus: data from LUMINA, amultiethnic US cohort (LUMINA L). Ann Rheum Dis 2007; 66:
This work is dedicated to the memory of Dr Josep
Font (1953–2006), who was principally responsible
11 Bosch, X, Guilabert, A, Pallares, L, et al. Infections in systemic lupus
erythematosus: a prospective and controlled study of 110 patients.
for the creation and follow-up of one of the largest
European cohorts of patients with SLE for more
12 Font, J, Ramos-Casals, M, Cervera, R, et al. Cardiovascular risk fac-
than 30 years. We thank David Buss for his editorial
tors and the long-term outcome of lupus nephritis. QJM 2001; 94: 19–26.
13 Golbus, J, McCune, WJ. Lupus nephritis: classification, prognosis,
immunopathogenesis and treatment. Rheum Dis Clin North Am1994; 20: 213–241.
14 Rudnicki, RD, Gresham, GE, Rothfield, NF. The efficacy of antima-
larials in systemic lupus erythematosus. J Rheumatol 1975; 2: 323–30.
15 The Canadian Hydroxychloroquine Study Group. A randomized
1 D’Cruz, DP, Khamashta, MA, Hughes, GR. Systemic lupus erythe-
study of the effect of withdrawing hydroxychloroquine sulphate in sys-
matosus. Lancet 2007; 369: 587–596.
temic lupus erythematosus. N Engl J Med 1991; 324: 150–154.
2 Mok, CC, Ying, KY, Ng, WL, et al. Long-term outcome of diffuse
16 Petri, M. Hydroxychloroquine prevents later damage in SLE.
proliferative lupus glomerulonephritis treated with cyclophospha-
mide. Am J Med 2006; 119: 355.e25–e33.
17 Costedoat-Chalumeau, N, Amoura, Z, Hulot, JS, et al. Low blood
3 Huong, DL, Papo, T, Beaufils, H, et al. Renal involvement in sys-
concentration of hydroxychloroquine is a marker for and predictor
temic lupus erythematosus. A study of 180 patients from a single cen-
of disease exacerbations in patients with systemic lupus erythemato-
ter. Medicine (Baltimore) 1999; 78: 148–166.
sus. Arthritis Rheum 2006; 54: 3284–90.
4 Petri, M. Hydroxychloroquine use in the Baltimore Lupus Cohort:
18 Lafyatis, R, York, M, Marshak-Rothstein, A. Antimalarial agents:
effects on lipids, glucose and thrombosis. Lupus 1996; 1: S16–S22.
closing the gate on Toll-like receptors? Arthritis Rheum 2006; 54:
5 Fessler, BJ, Alarcon, GS, McGwin, G, et al. Systemic lupus erythe-
matosus in three ethnic groups: XVI. Association of hydroxychloro-
19 Kasitanon, N, Fine, DM, Haas, M, Magder, LS, Petri, M.
quine use with reduced risk of damage accrual. Arthritis Rheum 2005;
Hydroxychloroquine use predicts complete renal remission within 12
months among patients treated with mycophenolate mofetil therapy
6 Ruiz-Irastorza, G, Egurbide, MV, Pijoan, JI, et al. Effect of antima-
for membranous lupus nephritis. Lupus 2006; 15: 366–370.
larials on thrombosis and survival in patients with systemic lupus
20 Tsakonas, E, Joseph, L, Esdaile, JM, et al. The Canadian
erythematosus. Lupus 2006; 15: 577–583.
Hydroxychloroquine Study Group. A long-term study of hydroxy-
7 Tan, EM, Cohen, AS, Fries, J, et al. The 1982 revised criteria for clas-
chloroquine withdrawal on exacerbations in systemic lupus erythema-
sification of SLE. Arthritis Rheum 1982; 25: 1271–1272.
Antimalarials and outcomes of lupus nephritis
21 Barber, CE, Geldenhuys, L, Hanly, JG. Sustained remission of lupus
results of a nested matched case–control study. Ann Rheum Dis
nephritis. Lupus 2006; 15: 94–101.
22 Wallace, DJ. Antimalarials: the ‘real’ advance in lupus. Lupus 2001;
29 Sotelo, J, Briceno, E, Lopez-Gonzalez, MA. Adding chloroquine to
conventional treatment for glioblastoma multiforme: a randomized,
23 Andrade, RM, Alarcon, GS. Antimalarials in systemic lupus erythe-
double-blind, placebo-controlled trial. Ann Intern Med 2006; 144:
matosus: benefits beyond disease activity. Future Rheumatol 2006; 1:
30 Ruiz-Irastorza, G, Ugarte, A, Egurbide, MV, et al. Antimalarials
24 Bessant, R, Duncan, R, Ambler, G, et al. Prevalence of conventional
may influence the risk of malignancy in systemic lupus erythematosus.
and lupus-specific risk factors for cardiovascular disease in patients
with systemic lupus erythematosus: A case–control study. Arthritis
31 Nived, O, Jonsen, A, Bengtsson, AA, Bengtsson, C, Sturfelt, G. High
predictive value of the Systemic Lupus International Collaborating
Clinics/American College of Rheumatology damage index for sur-
25 Wasko, MC, Hubert, HB, Lingala, VB, et al. Hydroxychloroquine
vival in systemic lupus erythematosus. J Rheumatol 2002; 29: 1398–
and risk of diabetes in patients with rheumatoid arthritis. JAMA
32 Alarcón, GS, McGwin, G, Bastian, HM, et al. Systemic lupus erythe-
26 Tam, LS, Gladman, DD, Hallett, DC, Rahman, P, Urowitz, MB.
matosus in three ethnic group VII: Predictors of early mortality in the
Effect of antimalarial agents on the fasting lipid profile in systemic
LUMINA cohort. Arthritis Rheum 2001; 45: 191–202.
lupus erythematosus. J Rheumatol 2000; 27: 2142–2145.
33 Urowitz, MB, Gladman, DD. Contribution of observational cohort
27 Sachet, JC, Borba, EF, Bonfa, E, Vinagre, CG, Silva, VM,
studies in systemic lupus erythematosus: the University of Toronto
Maranhao, RC. Chloroquine increases low-density lipoprotein
Lupus Clinic experience. Rheum Dis Clin N Am 2005; 31: 211–221.
removal from plasma in systemic lupus patients. Lupus 2007; 16:
34 Molad, Y, Gorshtein, A, Wysenbeek, AJ, et al. Protective effect of
hydroxychloroquine in systemic lupus erythematosus. Prospective
28 Calvo-Alen, J, McGwin, G, Toloza, S, et al. LUMINA Study Group.
long-term study of an Israeli cohort. Lupus 2002; 11: 356–361.
35 Roman, MJ, Shanker, BA, Davis, A, et al. Prevalence and correlates
(LUMINA): XXIV. Cytotoxic treatment is an additional risk factor
of accelerated atherosclerosis in systemic lupus erythematosus. N Engl
for the development of symptomatic osteonecrosis in lupus patients:
DOB: 03/06/**** Current Dr.: Dr. *** Symptoms/Issue(s): Daily Pressure/Pain behind breastbone into mid back, pressure in esophagus, bloating, nausea, and pain causing her to bend forward. Date When Symptoms Started: 03/01/2008 Prior Diagnosis: IBS, Esophageal spasms, GERD, pulled muscle in the back, costal chondritis, Posture, General Pain, Nerve Receptors, Gallbladder,
 Previous antimalarial therapy in patients diagnosed with lupus nephritis: Influence on outcomes and
Previous antimalarial therapy in patients diagnosed with lupus nephritis: Influence on outcomes and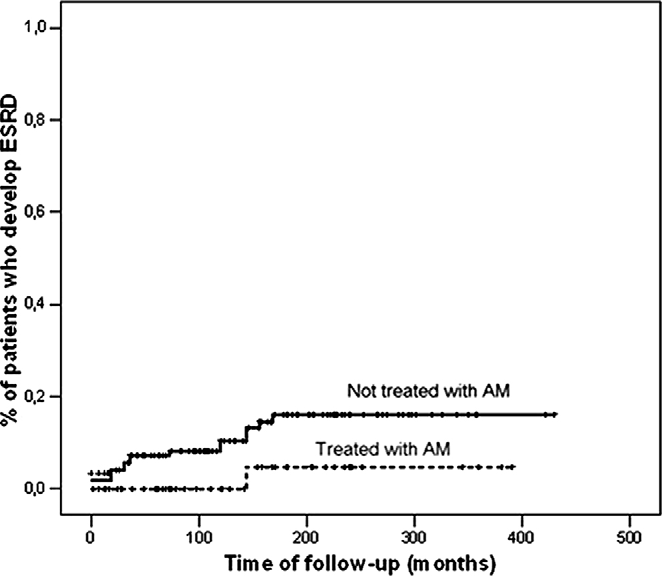
 Antimalarials and outcomes of lupus nephritisA Sisó, et al.
Antimalarials and outcomes of lupus nephritisA Sisó, et al.