Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Patient forms
WELCOME TO OUR OFFICE
Name: ____________________________________________________________ Date of Birth: ______________________________________ Address: __________________________________________________________ City: ______________________ State: ________ Zip Code: ________ Phone Number: ____________________________________________________ Social Security Number: ______________________________ Sex: [ ] M [ ] F
Occupation: _____________________________________________________
Employer: __________________________________________________
Work Phone Number: ___________________________ Extension: ________
Cell Phone Number: __________________________________________
Primary Care Physician: ______________________________________________ Phone #: __________________________________________ Primary Care Physician’s Address: ______________________________________ City: ____________________ State: _________ Zip Code: ________ Referring Physician: _________________________________________________ Phone #: ___________________________________________ Referring Physician’s Address: _________________________________________ City: ____________________ State: _________ Zip Code: _______ EMERGENCY CONTACT
Name: ___________________________________________________________ Home Phone #: ______________________________________________ Relationship: ______________________________________________________ Work Phone#: _______________________________________________ PHARMACY INFORMATION
Pharmacy Name: ____________________________________________________ Pharmacy Phone #: __________________________________ Pharmacy Address: __________________________________________________ City: ______________________ State: __________ Zip Code: ________ IF THIS IS RELATED TO A MOTOR VEHICLE ACCIDENT OR WORKER’S COMPENSATION PLEASE FILL OUT THIS SECTION
[ ] MVA Related
Adjuster: _______________________________________________________
Phone Number: __________________________ Extension: _________
Billing Address: __________________________________________________
City: ________________________ State: __________ Zip Code:______
Claim Number: ___________________________________________________ Date of Incident: ____________________________________ PRIMARY INSURANCE
Insurance Company: _________________________________________________ Subscriber’s Name: __________________________________________ Subscriber’s Date of Birth: ____________________________________________ Subscriber’s Social Security #:__________________________________ Relationship: [ ] Self [ ] Husband/Wife [ ] Father/Mother [ ] Other ___________________________ SECONDARY INSURANCE
Insurance Company: _________________________________________________ Subscriber’s Name: __________________________________________ Subscriber’s Date of Birth: ____________________________________________ Subscriber’s Social Security #:__________________________________ Relationship: [ ] Self [ ] Husband/Wife [ ] Father/Mother [ ] Other ___________________________ RELEASE OF INFORMATION/ASSIGNMENT OF BENEFITS:
Authorization is hereby granted to release information as may be necessary to process and complete my claims. I hereby authorize payment of medical benefits to be paid directly to the attending physician for services rendered. _______________________________________________________________
___________________________________________________________
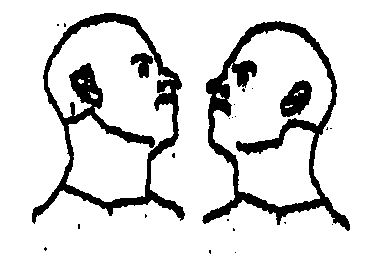
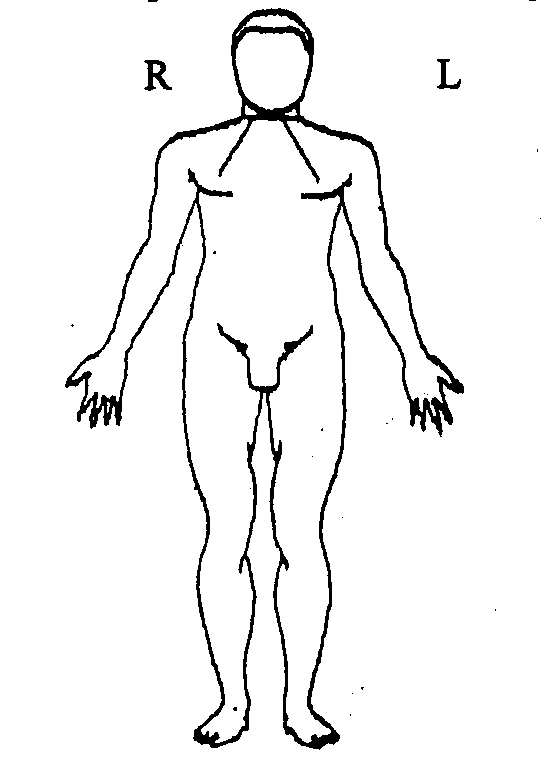
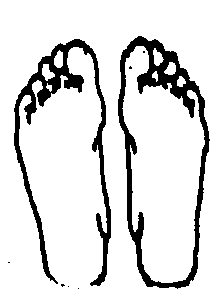
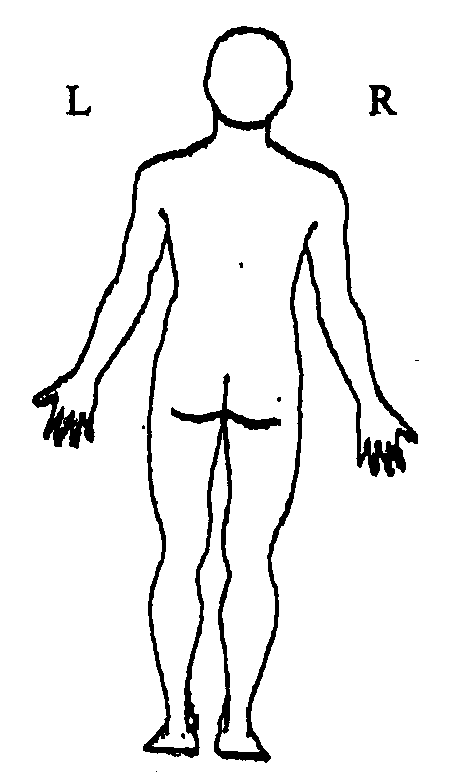
Center for Pain Management and Rehabilitation 635 East Main Street, Bridgewater NJ 08807 Phone: (908) 231-1131 Fax: (908) 231-1132 Shade in painful areas in the diagram below. (Please circle the most painful area)
FOR PHYSICIAN’S USE ONLY—DO NOT WRITE BELOW THIS LINE
Allergy: Intensity: 1 2 3 4 5 6 7 8 9 10 out of 10 Current Description of Pain: Location: Aggravating: Alleviating: Weakness/Numbness: Bowel/Bladder: Current Medications: Physical Exam: BP:
ROM: Neurological Exam: Impression: Plan:
Center for Pain Management and Rehabilitation 635 East Main Street, Bridgewater NJ 08807 Phone: (908) 231-1131 Fax (908) 231-1132 Previous Medications (Check appropriate boxes below if you have used these types of medications for your current pain problem and circle the medications that you have used)
[ ] Narcotics (i.e., Demerol, Morphine, Dilaudid, MS Contin, Methadone, Darvon, Percocet, Talwin, Vicodin, Codeine,
[ ] NSAIDS (i.e., Aspirin, Motrin, Ibuprophen, Dolobid, Toradol, Advil, Naprosyn, Relafen, Orudis)
[ ] Sedatives / Relaxants (i.e., Ativan, Xanax, Valium, Librium, Flexeril, Parafon Forte)
[ ] Antidepressants (i.e., Elavil, Pamelor, Desipramine, Effexor, Desyrel, Prozac, Zoloft, Paxil, Serzone, Remeron)
[ ] Anticonvulsants (i.e., Neuronton, Klonipin, Tegretol, Dilantin)
[ ] Neuropathic Pain Medications (i.e., Baclofen, Mexitil, Phenoybenzamine, Ultram, Prazocin) Previous Treatments (Please circle all that apply)
Other (specify) ________________________
Duration of Physical Therapy: ____________________________________
Review of Symptoms (Please circle all that apply) Past Medical History (Please circle all that apply)
This page reviewed by attending physician.
Center for Pain Management and Rehabilitation 635 East Main Street, Bridgewater NJ 08807 Phone: (908) 231-1131 Fax: (908) 231-1132 Past Surgical History (Please indicate date, type of surgery and physician’s name)
_________________________________________
_________________________________________
_________________________________________
_________________________________________
_________________________________________
_________________________________________
_________________________________________
_________________________________________
_________________________________________
_________________________________________
_________________________________________
_________________________________________
Medications (Please fill out all medications that you are using at this time) How many times/day Date Started 1.______________________________ ____________________ ____________________ __________________ 2.______________________________ ____________________ ____________________ __________________ 3.______________________________ ____________________ ____________________ __________________ 4.______________________________ ____________________ ____________________ __________________ 5.______________________________ ____________________ ____________________ __________________ 6.______________________________ ____________________ ____________________ __________________ 7.______________________________ ____________________ ____________________ __________________ 8.______________________________ ____________________ ____________________ __________________ 9.______________________________ ____________________ ____________________ __________________ 10______________________________ ____________________ ____________________ __________________ This page reviewed by attending physician.
Center for Pain Management and Rehabilitation 635 East Main Street, Bridgewater NJ 08807 Phone: (908) 231-1131 Fax: (908) 231-1132 Social History (Please complete information below)
[ ]Remarried [ ] Divorced [ ] Separated [ ] Widowed
Litigation history: is there any litigation in progress in regard to your pain condition? [ ] Yes
Family History FOR PHYSICIAN’S USE ONLY—DO NOT WRITE BELOW THIS LINE.
Miscellaneous __________________________________________________________________________________________ ____________________________________________________________________________________________________________ ____________________________________________________________________________________________________________ ____________________________________________________________________________________________________________
This page reviewed by attending physician.
Film4 and UK Film Council Present in association with The Wales Creative IP Fund and The Film Agency for Wales in association with Optimum Releasing and Protagonist Pictures in association with Red Hour Films Warp Films Production SUBMARINE A FILM BY RICHARD AYOADE DIRECTED & WRITTEN BY RICHARD AYOADE BASED ON A NOVEL BY JOE DUNTHORNE STARRING CRA
PATIENT AGREEMENT 1. I have read the attached MEDICATION GUIDE for using Mifeprex and misoprostol to end mypregnancy. 2. I discussed the information with my health care provider (provider). 3. My provider answered all my questions and told me about the risks and benefits of using Mifeprex andmisoprostol to end my pregnancy. 4. I believe I am no more than 49 days (7 weeks) pregnant. 5. I underst
 Center for Pain Management and Rehabilitation
Center for Pain Management and Rehabilitation