Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Microsoft word - gastric ulcers in the adult horse.doc
May 2004 Livestock Technology
INFOSheet
Ministry of Agriculture, Food and Rural Affairs
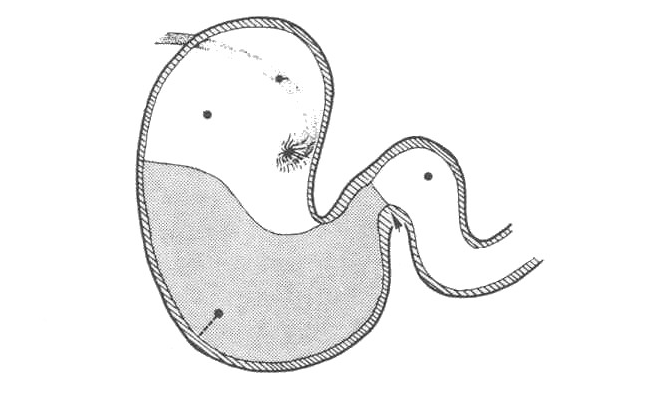
Gastric Ulcers in the Adult Horse The term ‘ulcers’ refers to a break or erosion in the lining of the esophagus, stomach or small intestines. The depth of the erosion determines the severity of the ulcer. Stomach ulcers are more common and occur primarily in the non-glandular (squamous) area of the stomach (See Figure 1). Less commonly, ulcers occur in the glandular area of the stomach. Stomach ulcers occur in horses of
all ages but particularly in foals and horses
and Thoroughbred horses in race training
affected. The clinical signs of ulcers are not
noticeable in most horses. Of those horses
clinically affected, the signs may include
poor athletic performance, weight loss and
colic. Horses may also have an unthrifty
appearance and mild diarrhea. In foals, teeth grinding (a sign of pain) and excessive
Figure 1. Food enters the stomach via the esophagus, leaves
salivation are common. Ulcers also occur in
through the opening called the pylorus and passes into the first
portion of the small intestine (duodenum). The stomach contains
Causes or Etiology Ulcers are caused by a variety of factors, including:
• diet and feeding management - including meal feeding, feeding high levels of concentrates, feed
deprivation and types of feed (timothy versus alfalfa).
• the stress of training and the stress of disease.
• medications such as corticosteroids. • bile acid reflux.
This is quite different than with ulcers in man where the bacterium Helicobacter pylori is now thought to be important in the pathogenesis of 90% of duodenal ulcers and about 70% of gastric ulcers (1). Diet and feeding management may play a major role in inducing ulcers in horses. By nature, horses are grazing animals, spending much of their day feeding. The grazing horse has a constant flow of saliva and passage of grass into the stomach, buffering stomach acid (2). Most horses graze pasture during the year. Bringing the Resources of the World to Rural Ontario Agricultural Information Contact Centre However, there are many horses, e.g., racehorses and high level event horses, that are managed as meal- eaters rather than being allowed to feed or graze continuously. They receive dry hay and concentrates year-round, or for the majority of the year, in a meal rather than eating continuously as in grazing. (Concentrates are mixtures of grain, crushed or whole, along with vitamins and minerals combined in various forms or textures (e.g., sweet-feed, pelletted feed) to compliment the nutrients found in the hay.) The feeding of high volumes of concentrates in itself increases the production of volatile fatty acids. This, combined with meal-feeding, results in sudden drops in gastric pH and damage to cells in the stomach and intestine. Measurements of gastric pH revealed that acidity (< pH 2.0) was greatest in horses deprived of food (3). An alternating regimen of feed deprivation for 24 hours followed by free choice hay for 24 hours resulted in erosions and ulceration of gastric mucosa with as little as 48 hours of cumulative food deprivation (3). This is important to remember; horses that are anorectic (not eating) or partially anorectic because of an underlying medical condition can develop erosions and ulcers in their gastric squamous mucosa within one to two days. When horses were fed timothy grass hay, gastric pH measurements were often greater than pH 6 (3). The feeding of alfalfa hay and grain resulted in a higher gastric pH than feeding grass hay. This may be due to the constituents of alfalfa but further research is needed in the area of the effect of forage type on gastric pH (3).
The stress of training regimen on the animal causes the increased release of corticosteroids and subsequent decrease in blood flow to the stomach lining. This interferes with the natural protective mechanisms and results in more damage from stomach acids. Medications, such as corticosteroids (prednisolone, dexamethasone) or non-steriodal anti-inflammatory medications (NSAIDS) (e.g., phenylbutazone or “Bute”, flunixin meglumine or Banamine), may similarly cause gastric ulceration. Bile acids, which are normally secreted into the duodenum, may reflux into the stomach and also damage the stomach lining. Treatment The treatment of stomach ulcers involves a combination of changes to feeding management, medical therapy, as well as reducing stress on the horse. Turnout onto green grass pasture along with altering the feeding regimen is likely the fastest method to allow the ulcers to heal. If concentrates are to be fed, they should be fed in small amounts at frequent intervals. There are many medications that are available to help heal ulcers. They include: • Antacids (aluminum and magnesium hydroxide) will reduce the acidity of the stomach for a short
period but must be given every two hours to be effective.
• Histamine-receptor antagonists. Cimetidine (Tagamet) and ranitidine (Xantac) are commonly used
in the horse and are considered very effective in the prevention and treatment of ulcers. They reduce both basal gastric acid production and induced acid production (e.g., from food) by competitively inhibiting histamine at the H2 receptors of the parietal cells (4).
• Omeprazole (Gastroguard, Pepsid) is the most potent anti-ulcer medication currently available. As a
proton pump inhibitor, it inhibits gastric acid secretion by interfering with hydrogen ions in the final stage of acid secretion. This medication is given by mouth once daily and, therefore, owner compliance is improved. The raw chemical of omeprazole is available from compounding
Gastric Ulcers in the Adult Horse
pharmacies. This type of product is less expensive than the commercial preparations. However, studies have shown that generic, compounded medications may be less effective. There is no quality control for compounded products. Therefore, the amount of active ingredient available in the compounded product may be very variable.
• Sucralfate (Carafate) is another type of medication that is useful in treating stomach ulcers,
especially in foals. After ingestion, sucralfate reacts with hydrochloric acid in the stomach to form a paste-like complex that will bind to the proteinaceous exudates that are generally found at ulcer sites. This insoluble complex forms a barrier at the site and prevents the ulcer from further damage caused by pepsin, acid and bile (4). Sucralfate will remain adherent to the ulcer crater for more than six hours (1). Because it requires an acidic environment to be effective, sucralfate should be administered at least ½ hour prior to cimetidine or antiacids.
Prognosis Adverse outcomes occasionally happen in horses with stomach ulcers. The ulcers may perforate into the abdominal cavity resulting in infectious peritonitis and rapid death. Scarring of the esophagus, gastric pylorus or duodenum may also occur, resulting in problems swallowing, emptying of the stomach and colic. Prevention and Recommendations Horses should be fed no less than 50% (and preferably >70%) of their dry matter intake as long dry hay or pasture. • If high levels of concentrates are required (greater than 2.5 lbs twice daily), they should be fed more
often and in small amounts, e.g., every 4-6 hours. Since this is labour intensive, and compliance will be variable, use of computerized or mechanical feeding systems may increase compliance.
• Turnout or, better yet, access to pasture on a daily basis is a good way of reducing stress for horses as
well as providing a continuous access to nutrients.
• Horses that are being deprived of food for extended periods of time (greater than 12 hours), e.g., pre
operatively, management of colic or for any other reason, should be carefully monitored for the development of ulcers (3).
References 1) MacAllister CG. A review of medical treatment for peptic ulcer disease. EVJ Suppl. 1999;29: 45-49. 2) Collier DSTJ. Editorial - Gastric Ulceration: Response to an unnatural environment. EVJ Suppl.
3) Murray MJ. Pathophysiology of peptic disorders in foals and horses: a review. EVJ Suppl. 1999;29:
4) Plumb DC. Veterinary Drug Handbook 4th ed. St. Paul: Iowa State Press, 2002. Dr. Dan Kenney, Diplomate, A.C.V.I.M. is a staff veterinarian
Permission is granted to use and reproduce this
with the Ontario Veterinary College, University of Guelph,
article in its entirety provided credit is given as
Guelph, Ontario N1G 2W1, Tel.: (519) 824-4120 ext. 54030,
Dr. Dan Kenney, Ontario Veterinary College, University of Guelph, Guelph,
Dr. Bob Wright is the Lead Veterinarian, Equine and Alternate
Ontario, Canada, and Dr. Bob Wright,
Species with the Animal Health and Welfare Branch of the Ontario
Ontario Ministry of Agriculture, Food and
Ministry of Agriculture, Food and Rural Affairs, Unit 10,
Rural Affairs, Elora, Ontario, Canada
6484 Wellington Road 7, Elora, Ontario N0B 1S0
Material may not be changed without the
Tel.: (519) 846-3412, Fax: (519) 846-8178, E-mail: robert.wright@ontario.ca
Gastric Ulcers in the Adult Horse
Effect of enteral feeding on lipid subfractionsin children with chronic renal failureJameela A. Kari1, Vanessa Shaw1, David T. Vallance2, and Lesley Rees11 Nephrourology Unit, Great Ormond Street NHS Trust, London WC1N 1EH, UK2 Department of Biochemistry, Royal Free Hospital and School of Medicine, Hampstead, London NW3, UKReceived August 19, 1997; received in revised form December 19, 1997;
Verwendung ausschließlich zu privaten Zwecken gestattetAus: Wegweiser Psychopharmaka von Carola Burkhardt-NeumannDieses Buch informiert in allgemeiner Form über Psychiatrie und diedort eingesetzten Medikamente. Die Angaben wurden zwar mit größ-ter Sorgfalt erstellt, im Interesse der Lesbarkeit wurde jedoch keine Voll-ständigkeit angestrebt. Auch sind Fehler naturgemäß nie ganz auszu-sch