Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
3 cols.qxd
4_Learning points.qxp 29/11/2007 14:32 Page 264
Learning points
Diagnosing and managing hypertension can help minimise the risk of cardiovascular disease
In the last article of the year in our Learning points series Candy Norris refreshes our knowledge on the
As a major modifiable contributory factor
in cardiovascular disease, the management
of high blood pressure is an important way
minimise this risk. However, to best achieve
pressure targets in different patient groups
not do regular exercise because of pressure
Latanoprost 1 drop both eyes at night.
through participation and to this endquestions have been included throughout
this article that will help you think about
to spironolactone, metformin, co-codamol,
reading through the case study andassociated questions — which you are
In view of his renal impairment and raised
microalbuminuria/creatinine ratio of 7,what would be a target blood pressure for
˿ understand the different blood pressure
this patient and what guidance is this based
in their Clinical Guideline H (October
2002)1 for people with diabetes is <140/80
guidance is taken from the Chronic kidneydisease in adults: UK guidelines (March
above: Although patients might not feel anxious
pharmacist-led hypertension clinic held in
about having their blood pressure measured, somepatients do experience a significant rise in blood
albuminuria or proteinuria and for those with
intensive control of his hypertension. He
pressure simply because they are attending a
total proteinuria of >1g per day the target
clinic. This ‘white coat’ hypertension is sometimesincorrectly interpreted as genuine hypertension.
mended for this patient is <130/80mmHg.
NOVEMBER/DECEMBER 2007 PHARMACY IN PRACTICE
4_Learning points.qxp 29/11/2007 14:32 Page 266
Learning points
thought to have raised blood pressure. This
that dependence on drug therapy alone will
result in prolonged drug therapy for a large
could suggest the possibility of coarctation
This patient needs to address his obesity
cardiological procedures, such as cardiac
problem and lack of exercise. Unfortunately,
these two lifestyle factors often go hand-in-
hand, and because he is also taking insulin,
starting a weight loss programme couldseem to be an uphill struggle.
Why would this patient be at risk of ‘white
highlighted as a key factor in hypertension,4
The patient could be at risk of white coat
istockphoto be that there are some gentle exercises that
secondary care clinic and, therefore, visiting
outpatients at hospital. Although patients
smoker but does drink some alcohol, which
above: Blood pressure readings should be made in both arms with the patient seated at the initialassessment. This is important to check whetherthere are any differences that might suggest co-
having ‘hypertension’ using conventional
existing disease or anatomical variation. The
ions of two or more lifestyle modifications
blood pressure readings should then be repeated
could achieve even better results. However,
have ‘white coat hypertension’ and may not
with the patient in the standing position to check
in practice it still seems that many patients
find the theory easier to get to grips withthan the application of it, and this is one
systolic or diastolic differences described,
blood pressure reading should be used for
in the sitting position, at the initial visit
is the most effective method of determining
standing position. This is so that any degree
result of ‘white coat hypertension’ or
of postural drop can be assessed and taken
into consideration in the drug managementof the patients.
At the initial visit where should his blood
What additional lifestyle measures should
above: This patient is overweight, does little exercise and does drink some alcohol. Helping him to consider lifestyle factors, such as his diet,drinking habits and exercise, might therefore,
lifestyle advice.4 The guidelines point out
make a significant impact on his blood pressure.
NOVEMBER/DECEMBER 2007 PHARMACY IN PRACTICE
4_Learning points.qxp 29/11/2007 14:33 Page 267
Learning points
In relation to current guidelines how well
ideations and should not be used unless the
microalbuminuria is ramipril.1 Unfortunat-
with ramipril if appropriate. However, he is
agent (Irbesartan) — and is taking this
second line drug at the maximum evidence-
based dose for this group of patients.
recent large clinical outcome trials hadprovided new information.8 A major change
is that of beta-blockers being no longer a
is taking atenolol, which is an appropriate
preferred initial treatment for hypertension.
second line drug. The dose is 25mg daily,
However, unless there are good reasons for
and so it may be possible to increase this
already stabilised, it is not recommended
precludes the use of bendroflumethiazide.5
He is not taking a calcium channel blocker,
above: Weighing patients regularly may help them to address their obesity problem and adhere to a healthy diet to keep their weight down.Candy Norris, clinical pharmacy manager,
Harrogate and District Foundation Trust, UK
As discussed above, the next step would be
References
1. National Institute for Health and Clinical Excellence. Clinical
Guideline H. Management of type 2 diabetes. Management of
added at 5mg daily for four weeks and then
blood pressure and blood lipids. National Institute for Healthand Clinical Excellence, London, 2002. Available at: http://
increased to the maximum of 10 mg daily.
www.nice.org.uk/nicemedia/pdf/NICE_INHERITEd_Hv8.pdf.
2. Joint Specialty Committee on Renal Medicine of the Royal
College of Physicians of London and the Renal Association. Chronic kidney disease in adults UK guidelines foridentification, management and referral. London: Royal
patient, there are often problems with the
side-effect of swollen ankles in females. In
3 .Ramsey L, Williams B, Johnston G, MacGregor G, Poston L,
Potter J, Poulter N, Russell G. Guidelines for management of
hypertension: report of the third working party of the British
studies evaluating rimonabant 20mg versus
Hypertension Society, 1999-BHS 111. J Hum Hypertens 1999; 13: 569–92.
placebo in addition to a hypocalorific diet.7
4. Williams B, Poulter NR, Brown MJ et al. British Hypertension
Society Guidelines. Guidelines for management of
Is it appropriate to consider rimonabant for
hypertension: report of the fourth working party of the
British Hypertension Society, 2004-BHS1V. J Hum Hypertens 2004; 18: 139–85.
5. British National Formulary 54 September 2007 Appendix 3
cholesterol, triglyceride levels and systolic
6. British National Formulary 54 September 2007 Section 4.5.2
diet and exercise for the treatment of obese
Centrally acting appetite suppressants.
underlines the appropriateness of this drug
7.Curioni C. Rimonabant for overweight or obesity. CochraneDatabase and Systematic Reviews 2006; Issue 4.
patients (BMI>27kg/m2) with associated
8. National Institute for Health and Clinical Excellence. Management of hypertension in adults in primary care:pharmacological update of Clinical Guideline 18, 2006.
NOVEMBER/DECEMBER 2007 PHARMACY IN PRACTICE
Quincy Area EMS System STUDY GUIDE ECRNs and Paramedics 2008 Version QAEMS Policy & Procedure Manuel . blessinghealthsystem.org Click “ Community Resources ” Click “ Emergency Medical Services ” in the drop down menu, then Click “ Download PDF version of QAEMS Policy & Procedure Manual ” (located in the column under the apple sitting on the d
Carbon Monoxidee Poisoning By: Capt Nina M. Griffin NREMT‐P Boulder Mountain Fire Protection District Carbon Monoxide Facts Carbon monoxide, or CO, is an odorless, colorless gas that can cause sudden Known as the “Silent Killer” Carbon Monoxide is the byproduct of incomplete combustion, with one Carbon monoxide is dangerous to the body beca
 4_Learning points.qxp 29/11/2007 14:32 Page 264
Learning points
4_Learning points.qxp 29/11/2007 14:32 Page 264
Learning points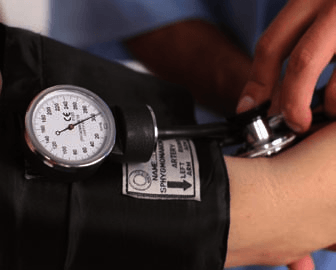
 4_Learning points.qxp 29/11/2007 14:32 Page 266
Learning points
4_Learning points.qxp 29/11/2007 14:32 Page 266
Learning points 4_Learning points.qxp 29/11/2007 14:33 Page 267
Learning points
4_Learning points.qxp 29/11/2007 14:33 Page 267
Learning points