Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Pone.0044668 1.6
Early Vascular Alterations in SLE and RA Patients—A Steptowards Understanding the Associated CardiovascularRisk
Maria Jose´ Santos1,2*, Diana Carmona-Fernandes1, Helena Canha˜o1,3, Jose´ Canas da Silva2, Joa˜o
1 Rheumatology Research Unit, Instituto de Medicina Molecular da Faculdade de Medicina de Lisboa, Lisbon, Portugal, 2 Rheumatology Department, Hospital Garcia de
Orta, Almada, Portugal, 3 Rheumatology and Metabolic Bone Diseases Department, Hospital de Santa Maria, Lisbon, Portugal, 4 Cardiology Department, Hospital
Accelerated atherosclerosis represents a major problem in both systemic lupus erythematosus (SLE) and rheumatoidarthritis (RA) patients, and endothelial damage is a key feature of atherogenesis. We aimed to assess early endothelialchanges in SLE and RA female patients (127 SLE and 107 RA) without previous CV events. Biomarkers of endothelial cellactivation (intercellular adhesion molecule-1 (sICAM-1), vascular cell adhesion molecule-1 (sVCAM-1), thrombomodulin (TM),and tissue factor (TF)) were measured and endothelial function was assessed using peripheral artery tonometry. Reactivehyperemia index (RHI), an indicator of microvascular reactivity, and augmentation index (AIx), a measure of arterial stiffness,were obtained. In addition, traditional CV risk factors, disease activity and medication were determined. Women with SLEdisplayed higher sICAM-1 and TM and lower TF levels than women with RA (p = 0.001, p,0.001 and p,0.001, respectively). These differences remained significant after controlling for CV risk factors and medication. Serum levels of vascularbiomarkers were increased in active disease and a moderate correlation was observed between sVCAM-1 levels and lupusdisease activity (rho = 0.246) and between TF levels and RA disease activity (rho = 0.301). Although RHI was similar across thegroups, AIx was higher in lupus as compared to RA (p = 0.04). Also in active SLE, a trend towards poorer vasodilation wasobserved (p = 0.06). In conclusion, women with SLE and RA present with distinct patterns of endothelial cell activationbiomarkers not explained by differences in traditional CV risk factors. Early vascular alterations are more pronounced in SLEwhich is in line with the higher CV risk of these patients.
Citation: Santos MJ, Carmona-Fernandes D, Canha˜o H, Canas da Silva J, Fonseca JE, et al. (2012) Early Vascular Alterations in SLE and RA Patients—A Step towardsUnderstanding the Associated Cardiovascular Risk. PLoS ONE 7(9): e44668. doi:10.1371/journal.pone.0044668
Editor: Songtao Shi, University of Southern California, United States of America
Received May 28, 2012; Accepted August 6, 2012; Published September 4, 2012
Copyright: ß 2012 Santos et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: This study was supported by a grant from Fundac¸a˜o para a Cieˆncia e a Tecnologia, Portugal (PIC/IC/82920/2007). The funders had no role in studydesign, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing Interests: The authors have declared that no competing interests exist.
in regulating vascular tonus and permeability. Under basalconditions ECs express molecules such as thrombomodulin
Chronic systemic inflammation predisposes to accelerated
(TM), which prevent platelet aggregation and the activation of
atherosclerosis, a risk that is well known in systemic lupus
the clotting cascade. Further platelet inhibition is achieved as a
erythematosus (SLE) and in rheumatoid arthritis (RA) patients
result of nitric oxide (NO) synthesis, a major vascular relaxant with
[1]. Subclinical vascular lesions develop long before atherosclerosis
anti-inflammatory and anti-proliferative properties. During the
becomes clinically evident, and they progress more rapidly in SLE
inflammatory process, ECs undergo changes characterized by
[2] and RA [3] than in the general population. Traditional
enhanced expression of adhesion molecules, increased transen-
cardiovascular (CV) risk factors do not fully explain this enhanced
dothelial permeability, and loss of antithrombotic properties [11].
risk, and the disease itself is considered an independent CV risk
Pro-inflammatory cytokines suppress TM expression and promote
factor [1]. In addition, the potential contribution of genetic
its cleavage and release into circulation [12]. In addition, they
variants to the development of atherosclerosis in RA patients has
induce the expression of tissue factor (TF), a procoagulant
been recently highlighted [4,5]. However, the reported magnitude
molecule absent from the surface of the intact ECs [13], shifting
of the CV risk is several times higher in SLE than in RA [6–9],
the balance towards a prothrombotic state. Furthermore, damaged
and the reason for this divergence is still incompletely understood.
endothelium loses its ability to produce vasodilators, thus adding to
Endothelial damage is considered the first step in the
the vascular injury. Endothelial dysfunction is potentially a
pathogenesis of atherosclerosis. It correlates with disease progres-
reversible disorder. Indeed, in patients with active RA, the
sion and predicts CV events in the general population [10]. The
infusion of infliximab, a chimeric antibody against TNF, has been
importance of endothelial cells (ECs) for vascular health is
found to improve biomarkers of endothelial activation [14] and
highlighted by its crucial role in maintaining blood fluidity and
transiently ameliorate endothelial function[15].
September 2012 | Volume 7 | Issue 9 | e44668
In vivo, vascular function can be examined non-invasively by
Quantification of soluble vascular biomarkers and
quantifying biomarkers of endothelial activation/damage, by
measuring the ability of endothelium to release NO in response
Measurements were performed using commercial enzyme-
to various stimuli or by assessing arterial wall stiffness [16].
linked immunosorbent assay (ELISA) based methods according
Previous data indicate impaired endothelial function both in SLE
to the manufacturers’ instructions. The Human sICAM-1
[17] and in RA patients [18] when compared to non-inflammatory
FlowCytomix Simplex Kit and the Human sVCAM-1 FlowCyto-
controls. Nevertheless it is unclear whether the magnitude of early
mix Simplex Kit (Bender MedSystems GmbH, Vienna, Austria)
vascular changes is similar in these two diseases.
were used for quantification of adhesion molecules, both using the
Given the clinical and pathophysiological particularities of SLE
FlowCytomix TM Technology. Serum levels of TM were measured
and RA, we hypothesize that endothelial function is differently
using the Human Thrombomodulin ELISA Kit (Cell Sciences H,
disturbed in these two patient groups, which could explain the
Canton, MA, USA) and serum levels of TF were quantified using
different CV risk. Thus, the major aim of our study was to
the AssayMax Human Tissue Factor ELISA kit (Assaypro, St
compare endothelial cell function between SLE and RA as
assessed by the measurement of soluble vascular biomarkers andby endothelial function testing, taking into account the presence of
traditional CV risk factors and systemic inflammation.
Endothelial function was assessed by peripheral artery tonom-
etry (PAT). PAT is a noninvasive operator-independent method
that evaluates changes in pulse wave amplitude before and after
reactive hyperemia. The inter-day variability of this technique inour department is 11% (data not published). The exam was
Consecutive SLE and RA women fulfilling the ACR classifica-
performed using the EndoPAT 2000 device (Itamar Medical Ltd,
tion criteria and free of clinically manifest CV disease were
Cesarea, Israel) as described elsewhere [22] and by assessors
recruited from the rheumatology clinics of Hospital Garcia de
blinded to the clinical diagnosis. Briefly, patients were placed in a
Orta, Almada, and Hospital de Santa Maria, Lisbon, between
quiet room, in supine position, with a specially designed finger
April 2009 and October 2010. A control group of women without
probe on the index finger of each hand, and a pressure cuff placed
systemic inflammatory diseases was also recruited from the local
on one arm. Patients were recommended to refrain from smoking
community and evaluated in the same period. Participants were
and drinking coffee or tea during the previous 24 hours and not to
excluded if they were pregnant, breastfeeding, had impaired renal
eat for at least 6 hours preceding the exam. PAT was continuously
function (defined as serum creatinine .1.5 mg/dl), or had
measured during a 10-minute baseline period, for 5 minutes after
documented ischemic heart disease (previous infarction, revascu-
the pressure cuff was inflated to suprasystolic pressure and for 10
larization surgery, angina, or heart failure), cerebrovascular
additional minutes following the release of upper arm occlusion.
disease (stroke or transient ischemic attack) or symptomatic
Pressure changes reflecting pulse amplitude were transmitted to a
peripheral artery disease. The study was approved by the Ethics
computer and reactive hyperemia index (RHI) was calculated as
Committee of both hospitals and was conducted in accordance
the ratio of PAT signal amplitude after cuff deflation divided by
with the principles stated in the Declaration of Helsinki. All
the amplitude of baseline signal, adjusted for fluctuations in the
participants gave written informed consent.
magnitude of the signal in the contralateral finger [22]. Augmentation index (AIx) was calculated from the mean PAT
waveform of the baseline period dividing the amplitude of the
Demographic data, disease characteristics, current medication,
second systolic peak by the difference between the second and the
and CV risk profile including blood pressure, serum lipids, fasting
glycemia, smoking habits, and body mass index (BMI) wereobtained. Patients were diagnosed with hypertension if the
measured blood pressure was repeatedly $140/90 mm/Hg or if
Continuous variables are expressed as means with standard
they used antihypertensive medication. The diagnosis of diabetes
deviations and categorical variables as the number of affected
was made if fasting glucose level was $126 mg/dl, or if patients
individuals and proportion of the total. Bivariate comparisons of
were under pharmacological treatment. Participants were classi-
SLE and RA patients were made using Student T-tests, Mann-
fied as obese if BMI was $30 Kg/m2. Disease activity was
Whitney, Kruskal-Wallis or x2 tests, as appropriate.
evaluated using the SLE Disease Activity Index 2000 (SLEDAI
The levels of vascular biomarkers, as well as RHI and AIx, were
2K), [19] and in RA patients 28 joints were examined for
compared between SLE and RA patients first as crude means
tenderness and swelling, and the 4 variable disease activity score
using the Mann Whitney test, followed by analysis of covariance
(DAS28) was calculated using erythrocyte sedimentation rate [20].
(ANCOVA) to adjust for significant and clinically relevant baseline
Disease activity was stratified according to the cutoffs of each
covariates. Likewise, in order to assess the effect of disease activity
instrument [20,21]: remission (SLEDAI 2K = 0 for SLE or
on vascular biomarkers, RHI and AIx, comparisons between
DAS28,2.6 for RA patients), low disease activity ($1 SLEDAI
remission and active disease were performed.
2K,4, in the case of SLE, or $2.6 DAS28#3.2, in the case of
Correlation between disease activity and endothelial cell
RA), and active disease (SLEDAI 2K$4 or DAS28.3.2, for SLE
function was studied separately in SLE and RA using Spearman
correlation coefficient and partial correlations to control for age,
Fasting blood samples were obtained before any other
disease duration, cardiovascular risk factors and medication.
procedures for measurement of glucose, uric acid, lipids (total
Statistical analysis was performed assuming a 5% significance
cholesterol, high density lipoprotein (HDL) cholesterol, low density
level and using SPSS 17 for Windows.
lipoprotein (LDL) cholesterol, and triglycerides), inflammatorymediators (C-reactive protein (CRP) and fibrinogen) and solublevascular biomarkers (sICAM-1, sVCAM-1, TM, and TF).
September 2012 | Volume 7 | Issue 9 | e44668
compared to RA (16% vs 11%; p = 0.04), indicating increasedarterial wall stiffness in these patients. This increase remained
In total 127 women with SLE and 107 with RA, were included
statistically significant after controlling for differences in baseline
in the study. A control group of 124 women, mean age
46.9613.7 years, 98% Caucasian, and 52% postmenopausal wasalso evaluated as reference. Demographic and clinical character-
Disease activity and endothelial function
istics of SLE and RA patients are shown in Table 1. SLE women
Patients presented a broad range of disease activity. The mean
were younger and had shorter disease duration (8.466.5 years)
SLEDAI 2K was 3.4664.5 (range 0 to 21) and the mean DAS28
compared to women with RA (10.767.3 years, p = 0.01). All lupus
was 4.1961.4 (range 1.70 to 7.54). Disease was in remission in
patients were ANA positive and 89% of RA patients were positive
41% of SLE and in 17% of RA cases. 39% of SLE patients
either for IgM RF or for anti-citrullinated protein antibodies. The
presented moderate/high active disease defined as a SLEDAI
use of antimalarials and aspirin was more common in lupus, while
2K$4, and 72% of RA had moderate/high active disease
more RA patients received methotrexate. Serum concentration of
according to the DAS28 definition. Except for prednisolone
fibrinogen was higher in SLE (SLE 3266147 mg/dl vs RA
dosage, which was significantly higher in active SLE and active
2766101 mg/dl; p = 0.01), but CRP levels were similar in both
RA than in remission, demographic characteristics, CV risk profile
groups (SLE 1.1663.2 mg/dl vs 1.0662.5 mg/dl; p = 0.75).
and medication was comparable in quiescent and active disease.
Overall, serum levels of vascular biomarkers were elevated
Vascular biomarkers and endothelial function as assessed
when disease was active, being statistically significant the
differences in sICAM-1, TM and TF levels between active and
A distinct pattern of soluble ECs biomarkers was identified in
quiescent SLE and in sICAM-1 and TF levels between active RA
SLE and in RA. While sICAM-1 and TM levels were significantly
higher, TF was lower in lupus than in RA patients (Figure 1).
sVCAM-1 showed a significant Spearman and partial correla-
Differences in sICAM-1, TM and TF remained significant after
tion with lupus disease activity measured by the SLEDAI (rho
adjustment for covariates (Table 2).
0.246 and 0.361; p = 0.007 and p,0.001 respectively) and TM
Reactive hyperemia was similar in SLE (RHI = 2.13560.686),
levels correlated with DAS28 (rho 0.301 and 0.250; p = 0.002 and
in RA (RHI = 2.19460.810) and in the control population
p = 0.005). In SLE patients there was also a significant correlation
(2.09060.579), while AIx was significantly higher in SLE as
between sVCAM-1, TM, TF and ESR (rho 0.246, 0.323 and0.263; p = 0.01, p = 0.001 and p = 0.01, respectively) and betweenserum TM levels and CRP (rho 0.315; p = 0.001). No significant
Table 1. Demographic and clinical characteristics of SLE and
correlation was found in RA patients between ESR or CRP and
A trend toward lower RHI was observed in active SLE
(1.80660.16) as compared with remission (2.24960.13; p = 0.06),
but no significant correlation was observed between RHI, AIx andSLEDAI or DAS28.
In this comparative study we found distinct patterns of soluble
vascular biomarkers in SLE and in RA female patients free from
clinically evident CV disease. Lupus patients presented higher
serum sICAM-1 and TM levels, while TF was elevated in RA
patients. These findings are relevant for understanding the
pathophysiology of the increased CV risk in SLE and RA patients,
as cell adhesion molecules may represent a link between
inflammation and atherosclerosis. In fact, not only are VCAM-1and ICAM-1 highly expressed on the endothelium overlaying
atherosclerotic lesions [23,24], but an increased serum concentra-
tion of these molecules is also related to CV risk factors [25] and
incident myocardial infarction [26]. In particular, high serum
levels of ICAM-1 represent an independent risk factor for
atherosclerosis and a predictor of future CV events [26,27]. Inaddition, we observed significantly increased levels of vascular
biomarkers in active disease. These observations are in line with
previous studies demonstrating that inflammatory mediators,
including TNF, IL-6, interferon-gamma (INFc) [28], IL-18 [29],
but also MCP-1 and MIF [30], upregulate endothelial cell
adhesion molecule expression. The fact that SLE patients exhibit
higher sICAM-1 and also higher fibrinogen concentrations may berelevant in the initiation and progression of atherosclerosis.
Results are presented as means (SD) or number of affected individuals and (%).
Indeed, ICAM-1 serves as a binding site for fibrinogen and
SLE – systemic lupus erythematosus; RA – rheumatoid arthritis; CV-
promotes adhesion and transendothelial migration of leukocytes
cardiovascular; HDL – high density lipoprotein; LDL – low density lipoprotein, ns
[31], an important early step in inflammatory vascular disease. We
– non significant. doi:10.1371/journal.pone.0044668.t001
did not find any difference in VCAM-1 serum levels among the
September 2012 | Volume 7 | Issue 9 | e44668
Figure 1. Serum concentrations of vascular biomarkers in SLE and RA patients and non-inflammatory controls. sICAM-1– solubleintercellular adhesion molecule; sVCAM-1 – soluble vascular cell adhesion molecule; RHI–reactive hyperemia index; Aix – augmentation index; SLE –systemic lupus erythematosus; RA – rheumatoid arthritis. doi:10.1371/journal.pone.0044668.g001
studied groups. In animal models, VCAM-1 expression is
the control population and the relationship to atherosclerosis is
considered a major early event in the atherosclerotic process
uncertain [34,35]. Nevertheless, very recently sVCAM-1 was
[32], and increased sVCAM-1 levels have been reported in lupus
identified as an independent predictor of overall and cardiovas-
nephritis [33]. However, in RA and SLE patients without renal or
vascular disease, serum concentrations of VCAM-1 are similar to
Table 2. Vascular biomarkers and results of PAT assessment in SLE and RA, after controlling for baseline covariates.
Adjusted for CV risk factors, disease duration and
Results are presented as estimated marginal means (SE). *Adjusted for the following covariates: age, disease duration, total cholesterol, HDL, LDL, triglycerides, aspirin, hydroxychloroquine, methotrexate use, and prednisolonedose. 1RHI and AIx results refer to 87 women with SLE and 75 with RA. sICAM-1 – soluble intercellular adhesion molecule; sVCAM-1 – soluble vascular cell adhesion molecule; TM – thrombomodulin; TF – tissue factor; RHI – reactivehyperemia index; AIx – augmentation index. doi:10.1371/journal.pone.0044668.t002
September 2012 | Volume 7 | Issue 9 | e44668
diseases remains uncertain [44–46]. Similarly, the improvement
Table 3. Vascular biomarkers and endothelial function in
following anti-rheumatic medication is not universally supported
by the available literature [18]. Using PAT, we did not find anysignificant differences in RHI neither between patients and
controls, nor between SLE and RA. RHI quantifies changes inpulse wave amplitude in response to reactive hyperemia, a
measure of microvascular function. In the general population
RHI is an independent predictor of adverse cardiac events [47],
but its predictive value in rheumatic diseases has not beenestablished. The fact that we have included only females without
previous CV events and normal renal function (relatively low risk
population) may in part account for the comparable RHI found in
patients and controls. In fact, only in more active SLE cases did
RHI show a reduction. The follow up of these patients will allowus to ascertain the predictive value of RHI measured by PAT for
Results are expressed as estimated marginal means (SE) adjusted for
the development of CV event in SLE and RA patients.
prednisolone dose. *RHI and AIx results refer to 87 women with SLE and 75 with RA.
Lupus patients presented higher AIx than RA patients and this
SLE – systemic lupus erythematosus; RA – rheumatoid arthritis; sICAM-1 –
difference remained significant after controlling for covariates. In
soluble inter-cellular adhesion molecule; sVCAM-1 – soluble vascular cell
apparently healthy subjects arterial stiffness is an independent
adhesion molecule; TM – thrombomodulin; TF – tissue factor; RHI – reactive
predictor of coronary heart disease and stroke [48], but the
hyperemia index; AIx – augmentation index. doi:10.1371/journal.pone.0044668.t003
predictive value of AIx in rheumatic diseases is unknown. Cardiovascular risk factors and disease related features contribute
There is growing evidence supporting the relationship between
to arterial stiffening in SLE [49] and RA [50]. Shang et al found a
inflammation and thrombotic complications of atherosclerosis
correlation between carotid AIx and SLEDAI [51]. Increased
(atherothrombosis). Interestingly, TM expression, a molecule with
arterial stiffness was also associated with RA disease activity in
anti-coagulant properties, is reduced during the inflammatory
some, but not all, studies [18]. Increased AIx in SLE women
process [12], and increased soluble TM levels probably indicate
probably indicates a worse vascular condition.
EC injury. Together with increased TF, which is an initiator of the
Taken together, our observations add to the evidence that the
extrinsic coagulation cascade, this environment may raise the
pathogenesis of atherosclerosis associated with inflammation may
thrombogenic activity of plasma and contribute to cardiovascular
differ in SLE and RA. Additionally, we found more pronounced
events. Higher levels of TF in RA patients as compared to SLE
early vascular changes in lupus patients, and when the disease is
patients might be explained by the contribution of TNF to its
active, which is in line with the higher risk for CV events
expression [37]. Nevertheless, serum levels of adhesion molecules,
TM, and TF may not accurately translate endothelial functionalexpression of these molecules, which is a limitation of our work.
A further effect of proinflammatory cytokines on EC is the
inhibition of NO synthesis leading to endothelial dysfunction. In
We would like to thank Mrs Ce´lia Monteiro for her help with PAT
the general population, impaired endothelial function is a critical
early step in the development of atherosclerosis [38] and predictsthe progression of structural arterial disease independently of
conventional CV risk factors [39,40]. However, studies of
Conceived and designed the experiments: MJS HC JEF VG. Performed
endothelial function in inflammatory rheumatic diseases depicted
the experiments: MJS DC-F. Analyzed the data: MJS HC JEF JCS VG.
contradictory results [41–43], and the relevance of endothelial
Contributed reagents/materials/analysis tools: MJS DC-F VG. Wrote the
dysfunction for the progression of atherosclerosis in rheumatic
1. Symmons DP, Gabriel SE (2011) Epidemiology of CVD in rheumatic disease,
systemic lupus erythematosus: comparison with the Framingham Study.
with a focus on RA and SLE. Nat Rev Rheumatol 7: 399–408.
2. Thompson T, Sutton-Tyrrell K, Wildman RP, Kao A, Fitzgerald SG, et al.
8. Meune C, Touze E, Trinquart L, Allanore Y (2010) High risk of clinical
(2008) Progression of carotid intima-media thickness and plaque in women with
cardiovascular events in rheumatoid arthritis: Levels of associations of
systemic lupus erythematosus. Arthritis Rheum 58: 835–842.
myocardial infarction and stroke through a systematic review and meta-analysis.
3. Sodergren A, Karp K, Boman K, Eriksson C, Lundstrom E, et al. (2010)
Atherosclerosis in early rheumatoid arthritis: very early endothelial activation
9. Zoller B, Li X, Sundquist J, Sundquist K (2012) Risk of subsequent coronary
and rapid progression of intima media thickness. Arthritis Res Ther 12: R158.
heart disease in patients hospitalized for immune-mediated diseases: a
4. Lopez-Mejias R, Gonzalez-Juanatey C, Garcia-Bermudez M, Castaneda S,
nationwide follow-up study from Sweden. PLoS One 7: e33442.
Miranda-Filloy J, et al. (2012) The lp13.3 genomic region -rs599839- is
10. Vita JA (2011) Endothelial function. Circulation 124: e906–912.
associated with endothelial dysfunction in patients with rheumatoid arthritis.
11. Pober JS, Sessa WC (2007) Evolving functions of endothelial cells in
inflammation. Nat Rev Immunol 7: 803–815.
5. Rodriguez-Rodriguez L, Gonzalez-Juanatey C, Garcia-Bermudez M, Vazquez-
12. Boehme MW, Deng Y, Raeth U, Bierhaus A, Ziegler R, et al. (1996) Release of
Rodriguez TR, Miranda-Filloy JA, et al. (2011) CCR5Delta32 variant and
thrombomodulin from endothelial cells by concerted action of TNF-alpha and
cardiovascular disease in patients with rheumatoid arthritis: a cohort study.
neutrophils: in vivo and in vitro studies. Immunology 87: 134–140.
13. Drake TA, Cheng J, Chang A, Taylor FB Jr. (1993) Expression of tissue factor,
6. Fischer LM, Schlienger RG, Matter C, Jick H, Meier CR (2004) Effect of
thrombomodulin, and E-selectin in baboons with lethal Escherichia coli sepsis.
rheumatoid arthritis or systemic lupus erythematosus on the risk of first-time
acute myocardial infarction. Am J Cardiol 93: 198–200.
14. Gonzalez-Gay MA, Garcia-Unzueta MT, De Matias JM, Gonzalez-Juanatey C,
7. Manzi S, Meilahn EN, Rairie JE, Conte CG, Medsger TA Jr., et al. (1997) Age-
Garcia-Porrua C, et al. (2006) Influence of anti-TNF-alpha infliximab therapy
specific incidence rates of myocardial infarction and angina in women with
on adhesion molecules associated with atherogenesis in patients with rheumatoidarthritis. Clin Exp Rheumatol 24: 373–379.
September 2012 | Volume 7 | Issue 9 | e44668
15. Gonzalez-Juanatey C, Testa A, Garcia-Castelo A, Garcia-Porrua C, Llorca J, et
34. Rho YH, Chung CP, Oeser A, Solus J, Asanuma Y, et al. (2009) Inflammatory
al. (2004) Active but transient improvement of endothelial function in
mediators and premature coronary atherosclerosis in rheumatoid arthritis.
rheumatoid arthritis patients undergoing long-term treatment with anti-tumor
necrosis factor alpha antibody. Arthritis Rheum 51: 447–450.
35. Rho YH, Chung CP, Oeser A, Solus J, Raggi P, et al. (2008) Novel
16. Lane HA, Smith JC, Davies JS (2006) Noninvasive assessment of preclinical
cardiovascular risk factors in premature coronary atherosclerosis associated
atherosclerosis. Vasc Health Risk Manag 2: 19–30.
with systemic lupus erythematosus. J Rheumatol 35: 1789–1794.
17. Mak A, Liu Y, Chun-Man Ho R (2011) Endothelium-dependent But Not
36. Gustafsson J, Simard JF, Gunnarsson I, Elvin K, Lundberg IE, et al. (2012) Risk
Endothelium-independent Flow-mediated Dilation Is Significantly Reduced in
factors for cardiovascular mortality in patients with systemic lupus erythema-
Patients with Systemic Lupus Erythematosus without Vascular Events: A
tosus, a prospective cohort study. Arthritis Res Ther 14: R46.
Metaanalysis and Metaregression. J Rheumatol 38: 1296–1303.
37. Kirchhofer D, Tschopp TB, Hadvary P, Baumgartner HR (1994) Endothelial
18. Sandoo A, Veldhuijzen van Zanten JJ, Metsios GS, Carroll D, Kitas GD (2011)
cells stimulated with tumor necrosis factor-alpha express varying amounts of
Vascular function and morphology in rheumatoid arthritis: a systematic review.
tissue factor resulting in inhomogenous fibrin deposition in a native blood flow
Rheumatology (Oxford) 50: 2125–2139.
system. Effects of thrombin inhibitors. J Clin Invest 93: 2073–2083.
19. Gladman DD, Ibanez D, Urowitz MB (2002) Systemic lupus erythematosus
38. Kozera L, Andrews J, Morgan AW (2011) Cardiovascular risk and rheumatoid
disease activity index 2000. J Rheumatol 29: 288–291.
arthritis–the next step: differentiating true soluble biomarkers of cardiovascular
20. Prevoo ML, van ’t Hof MA, Kuper HH, van Leeuwen MA, van de Putte LB, et
risk from surrogate measures of inflammation. Rheumatology (Oxford) 50:
al. (1995) Modified disease activity scores that include twenty-eight-joint counts.
Development and validation in a prospective longitudinal study of patients with
39. Bonetti PO, Lerman LO, Lerman A (2003) Endothelial dysfunction: a marker of
rheumatoid arthritis. Arthritis Rheum 38: 44–48.
21. Yee CS, Farewell VT, Isenberg DA, Griffiths B, Teh LS, et al. (2011) The use of
atherosclerotic risk. Arterioscler Thromb Vasc Biol 23: 168–175.
Systemic Lupus Erythematosus Disease Activity Index-2000 to define active
40. Halcox JP, Donald AE, Ellins E, Witte DR, Shipley MJ, et al. (2009) Endothelial
disease and minimal clinically meaningful change based on data from a large
function predicts progression of carotid intima-media thickness. Circulation 119:
cohort of systemic lupus erythematosus patients. Rheumatology (Oxford) 50:
41. Hansel S, Lassig G, Pistrosch F, Passauer J (2003) Endothelial dysfunction in
22. Bonetti PO, Barsness GW, Keelan PC, Schnell TI, Pumper GM, et al. (2003)
young patients with long-term rheumatoid arthritis and low disease activity.
Enhanced external counterpulsation improves endothelial function in patients
with symptomatic coronary artery disease. J Am Coll Cardiol 41: 1761–1768.
42. Foster W, Carruthers D, Lip GY, Blann AD (2010) Inflammation and
23. Davies MJ, Gordon JL, Gearing AJ, Pigott R, Woolf N, et al. (1993) The
microvascular and macrovascular endothelial dysfunction in rheumatoid
expression of the adhesion molecules ICAM-1, VCAM-1, PECAM, and E-
arthritis: effect of treatment. J Rheumatol 37: 711–716.
selectin in human atherosclerosis. J Pathol 171: 223–229.
43. Aizer J, Karlson EW, Chibnik LB, Costenbader KH, Post D, et al. (2009) A
24. Wood KM, Cadogan MD, Ramshaw AL, Parums DV (1993) The distribution of
controlled comparison of brachial artery flow mediated dilation (FMD) and
adhesion molecules in human atherosclerosis. Histopathology 22: 437–444.
digital pulse amplitude tonometry (PAT) in the assessment of endothelial
25. Demerath E, Towne B, Blangero J, Siervogel RM (2001) The relationship of
function in systemic lupus erythematosus. Lupus 18: 235–242.
soluble ICAM-1, VCAM-1, P-selectin and E-selectin to cardiovascular disease
44. Gonzalez-Juanatey C, Llorca J, Gonzalez-Gay MA (2011) Correlation between
risk factors in healthy men and women. Ann Hum Biol 28: 664–678.
endothelial function and carotid atherosclerosis in rheumatoid arthritis patients
26. Hwang SJ, Ballantyne CM, Sharrett AR, Smith LC, Davis CE, et al. (1997)
with long-standing disease. Arthritis Res Ther 13: R101.
Circulating adhesion molecules VCAM-1, ICAM-1, and E-selectin in carotid
45. Gustafsson J, Gunnarsson I, Borjesson O, Pettersson S, Moller S, et al. (2009)
atherosclerosis and incident coronary heart disease cases: the Atherosclerosis
Predictors of the first cardiovascular event in patients with systemic lupus
Risk In Communities (ARIC) study. Circulation 96: 4219–4225.
erythematosus – a prospective cohort study. Arthritis Res Ther 11: R186.
27. Luc G, Arveiler D, Evans A, Amouyel P, Ferrieres J, et al. (2003) Circulating
46. Gonzalez-Gay MA, Gonzalez-Juanatey C, Miranda-Filloy JA, Garcia-Unzueta
soluble adhesion molecules ICAM-1 and VCAM-1 and incident coronary heart
MT, Llorca J (2012) Lack of association between carotid intimamedia wall
disease: the PRIME Study. Atherosclerosis 170: 169–176.
thickness and carotid plaques and markers of endothelial cell activation in
28. Zhang J, Alcaide P, Liu L, Sun J, He A, et al. (2011) Regulation of endothelial
rheumatoid arthritis patients undergoing anti.TNF therapy. Acta Reumatol Port
cell adhesion molecule expression by mast cells, macrophages, and neutrophils.
47. Rubinshtein R, Kuvin JT, Soffler M, Lennon RJ, Lavi S, et al. (2010)
29. Morel JC, Park CC, Woods JM, Koch AE (2001) A novel role for interleukin-18
Assessment of endothelial function by non-invasive peripheral arterial tonometry
in adhesion molecule induction through NF kappa B and phosphatidylinositol
predicts late cardiovascular adverse events. Eur Heart J 31: 1142–1148.
(PI) 3-kinase-dependent signal transduction pathways. J Biol Chem 276: 37069–
48. Mattace-Raso FUS, van der Cammen TJM, Hofman A, van Popele NM, Bos
ML, et al. (2006) Arterial Stiffness and Risk of Coronary Heart Disease and
30. Amin MA, Haas CS, Zhu K, Mansfield PJ, Kim MJ, et al. (2006) Migration
inhibitory factor up-regulates vascular cell adhesion molecule-1 and intercellularadhesion molecule-1 via Src, PI3 kinase, and NFkappaB. Blood 107: 2252–2261.
49. Selzer F, Sutton-Tyrrell K, Fitzgerald S, Tracy R, Kuller L, et al. (2001)
31. Languino LR, Duperray A, Joganic KJ, Fornaro M, Thornton GB, et al. (1995)
Vascular stiffness in women with systemic lupus erythematosus. Hypertension
Regulation of leukocyte-endothelium interaction and leukocyte transendothelial
migration by intercellular adhesion molecule 1-fibrinogen recognition. Proc Natl
50. Provan SA, Angel K, Semb AG, Mowinckel P, Agewall S, et al. (2011) Early
prediction of increased arterial stiffness in patients with chronic inflammation: a
32. Nakashima Y, Raines EW, Plump AS, Breslow JL, Ross R (1998) Upregulation
15-year followup study of 108 patients with rheumatoid arthritis. J Rheumatol
of VCAM-1 and ICAM-1 at atherosclerosis-prone sites on the endothelium in
the ApoE-deficient mouse. Arterioscler Thromb Vasc Biol 18: 842–851.
51. Shang Q, Tam LS, Li EK, Yip GW, Yu CM (2008) Increased arterial stiffness
33. Yao GH, Liu ZH, Zhang X, Zheng CX, Chen HP, et al. (2008) Circulating
correlated with disease activity in systemic lupus erythematosus. Lupus 17:
thrombomodulin and vascular cell adhesion molecule-1 and renal vascular lesion
in patients with lupus nephritis. Lupus 17: 720–726.
September 2012 | Volume 7 | Issue 9 | e44668
Name (print): _________________________________________________________________ Medications & Parent/Guardian Permission PLEASE CAREFULLY READ THE FOLLOWING: If you disagree with any statements here, please cross out that section and initial it. Explain your wishes in the comment space provided. This medical form is correct so far as I know, and the person names in Section A has permission t
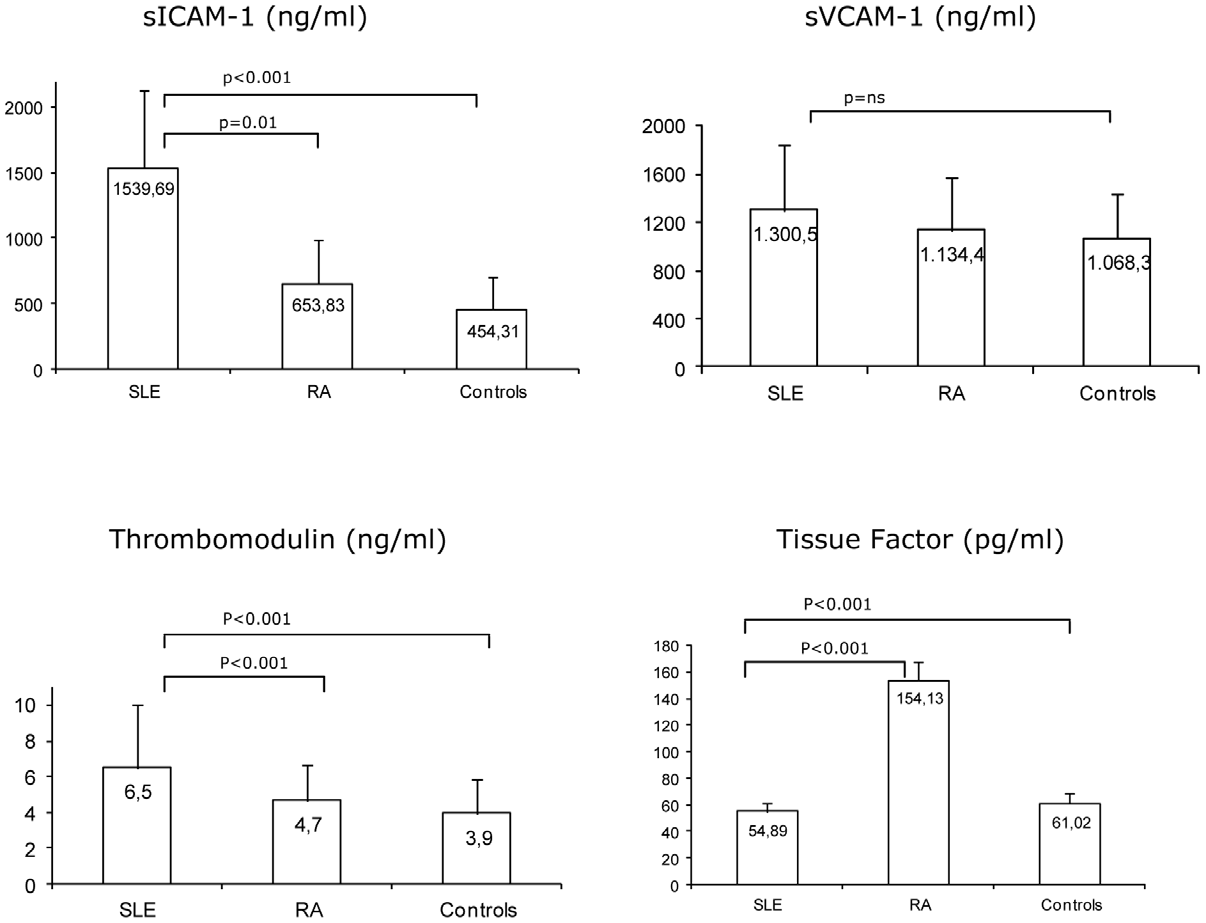 Figure 1. Serum concentrations of vascular biomarkers in SLE and RA patients and non-inflammatory controls. sICAM-1– solubleintercellular adhesion molecule; sVCAM-1 – soluble vascular cell adhesion molecule; RHI–reactive hyperemia index; Aix – augmentation index; SLE –systemic lupus erythematosus; RA – rheumatoid arthritis.
Figure 1. Serum concentrations of vascular biomarkers in SLE and RA patients and non-inflammatory controls. sICAM-1– solubleintercellular adhesion molecule; sVCAM-1 – soluble vascular cell adhesion molecule; RHI–reactive hyperemia index; Aix – augmentation index; SLE –systemic lupus erythematosus; RA – rheumatoid arthritis.