Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Untitled
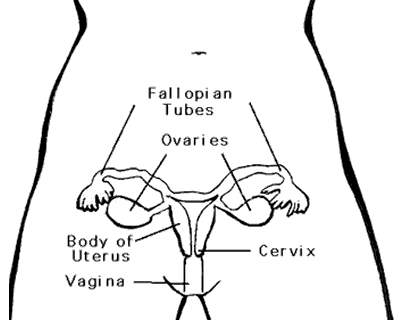
Q: What is endometrial cancer? A: Endometrial cancer is a cancer that starts in the inner lining of the womb (uterus). This lining is called the endometrium. The pictures below show where the uterus is found.
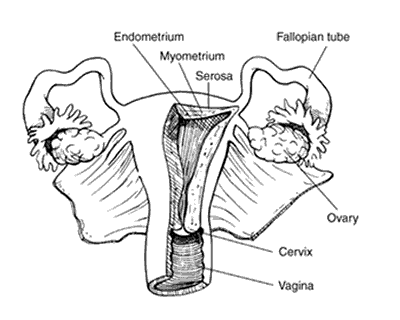
The picture below shows the uterus and its adjacent structures.
The uterus is a hollow organ, about the size and shape of a medium-sized pear. It has 2 main parts. The lower part, which extends into the vagina, is called the cervix. The upper part is the body of the uterus, also known as the corpus. The body of the uterus has three layers. The innermost layer is called the endometrium. During a woman's menstrual cycle the endometrium changes. In the early part of the cycle, it gets thicker in case the woman becomes pregnant. If she does not become pregnant, the tissue is shed from the uterus and becomes the menstrual flow. This cycle repeats throughout a woman's life until the time of menopause. Nearly all cancers of the uterus start in the endometrium. They are called endometrial carcinomas. Most carcinomas are cancers that start in the cells that form glands in the lining of the uterus. They are called adenocarcinomas. The
most common type of endometrial cancer is called endometrioid adenocarcinoma. Other rare types include squamous cell and undifferentiated. About 80% of endometrial cancers are typical adenocarcinomas, also known as endometrioid. These cancers are made up of cells in glands that look much like the normal uterine lining (endometrium). Some of them contain squamous cells (squamous cells are flat, thin cells that can be found on the outer surface of the cervix), as well as glandular cells. A cancer with both types of cells is called an adenocarcinoma with squamous differentiation. There are other types of endometrioid cancers, such as secretory carcinoma, ciliated carcinoma, and mucinous adenocarcinoma. The grade of an endometrioid cancer is based on how much the cancer forms glands that look similar to the glands found in normal, healthy endometrium.
Grade 1 tumors have 95% or more of the cancerous tissue forming glands. Grade 2 tumors have between 50% and 94% of the cancerous tissue forming Grade 3 tumors have less than half of the cancerous tissue forming glands.
They are called "high-grade", tend to be aggressive, and have a poorer prognosis than low grade cancers (grades 1 and 2). Some less common forms of endometrial adenocarcinoma are clear-cell carcinoma, serous carcinoma (also called papillary serous carcinoma), and poorly differentiated carcinoma. These cancers are more aggressive than most endometrial cancers. They tend to grow quickly and usually have spread outside the uterus at the time of diagnosis. Endometrial carcinomas may be classified into 2 types based on their prognosis and underlying causes. "Type 1" cancers are thought to be secondary to an excess estrogen. They are usually not very aggressive and are slow to spread to other tissues. Grades 1 and 2 endometrioid cancers belong to this type. A small number of endometrial cancers are "Type 2." The exact cause of these cancers is still unknown, although they have not been associated with unopposed estrogen. Serous carcinoma, clear-cell carcinoma, poorly differentiated carcinoma, and grade 3 endometrioid carcinoma are all type 2 cancers. They appear differently from a normal endometrium and thus are called "poorly differentiated" or "high-grade". They are more likely to grow and spread outside of the uterus and are thus associated with poorer prognosis (than type 1 cancers). Q: What are the key statistics about endometrial cancer? A: In the United States, cancer of the endometrium is the most common cancer of the female reproductive organs. The American Cancer Society estimates there will be 40,100 new cases of cancer of the body of the uterus (uterine corpus) diagnosed in the United States during 2008. Most of these occur in the
endometrium. The American Cancer Society also estimates that about 7,470 women in the United States will die from cancers of the uterine body during 2008. In the Philippines, cancer of the corpus uteri has been identified as the 9th leading site of cancer among Filipino women, with an incidence of 3.2%. There is an estimated 4.3 new cancer cases per 100,000 women in 2005. About 546 Filipino women afflicted with this disease died in 2005. This cancer is rare in women under the age of 45. Most cases are found in women who are 55 years old and over, with more than half of all endometrial cancer cases diagnosed in the 55 to 74 age group. The average chance of a woman being diagnosed with this cancer during her lifetime is about one in 41. There are over 500,000 women who are survivors of this cancer. This cancer is more common in white women, but black women are more likely to die from it. The 5-year relative survival rate from endometrial cancer is about 88%. Majority of these cancers are found at an early stage, with a 5-year survival rate of more than 95%. However, the prognosis for any single woman depends on the stage of her cancer as well as several other factors. Q: What are the risk factors for endometrial cancer? A: The cause of most cases of endometrial cancer is still unknown. However, there are certain risk factors that are linked to the development of this disease. A risk factor is anything that increases a person's chance of getting a disease such as cancer. Different cancers have different risk factors. A person can have several risk factors and still not get the disease. On the other hand, not having any risk factor does not mean that a woman will never have the disease. The following have been identified as risk factors for the development of endometrial cancer: Hormone levels – A woman's hormonal balance plays a part in most endometrial cancers. Many of the risk factors for endometrial cancer affect estrogen levels. Before menopause, the ovaries are the main source of the 2 main types of female hormones – estrogen and progesterone. The balance between these two hormones changes during a woman's menstrual cycle each month. A shift in the balance of these 2 hormones toward more estrogen increases a woman's risk for getting endometrial cancer. After menopause, the ovaries cease producing these hormones, but a small amount of estrogen is still made naturally in fat tissue. This estrogen has a bigger impact after menopause than it does before menopause. Female hormones are also available as birth control pills to prevent pregnancy, and hormone therapy to treat menopausal symptoms. Estrogen therapy – Using estrogen to treat symptoms of menopause is known as estrogen replacement therapy or hormone replacement therapy. Estrogen is available in various forms, such as pills, skin patches, creams, and vaginal rings.
It can reduce hot flashes, improve vaginal dryness, and help prevent the weakening of bones (osteoporosis) that can occur with menopause. Using estrogen alone (without progesterone) had been associated with the development of endometrial cancer. Progesterone-like drugs must be given along with estrogen in order to avoid this increased risk. This approach is called combination hormone therapy. Total number of menstrual cycles (periods) – Having more periods during a woman's lifetime raises her risk for endometrial cancer. Starting menstrual period (menarche) before age 12, or going through menopause late, raises the risk. Starting periods early is less a risk factor for women with early menopause. Likewise, late menopause may not lead to a higher risk in women whose periods began later in their teens. Pregnancy – During pregnancy, the hormonal balance shifts toward more progesterone. Therefore, having several pregnancies reduces endometrial cancer risk. Women who have never been pregnant (nulliparity) have a higher risk, especially if they were also infertile (unable to become pregnant). Obesity – Most of a woman's estrogen is produced by the ovaries, but fat tissue can change some other hormones into estrogens. Having more fat tissue thus can increase a woman's estrogen levels and, as a result, increase her endometrial cancer risk. In comparison with women who maintain a healthy weight, endometrial cancer is twice as common in overweight women, and more than three times as common in women who are obese. Tamoxifen – Tamoxifen is a drug that is used to treat women with breast cancer. It is also used to reduce the risk in women who are at high risk of getting breast cancer. The drug, unfortunately, acts like estrogen in the uterus. It can cause the uterine lining to grow thereby increasing the risk of endometrial cancer in women taking this drug. The risk of getting endometrial cancer in women taking tamoxifen is very small (about 1 in 500). It must be balanced against the benefit obtained from taking the drug in treating breast cancer and reducing the chances of the woman getting cancer in the other breast. Ovarian tumors – A certain type of ovarian tumor, the granulosa-theca cell tumor, often produces estrogen. However, the control mechanism by which estrogen is released by one of these tumors is different from that produced by the ovaries, which can sometimes lead to high estrogen levels. This may result to hormone imbalance which can stimulate the endometrium and may lead to endometrial cancer. In fact, sometimes vaginal bleeding from endometrial cancer is the first symptom of one of these tumors. Polycystic ovarian syndrome – Women with polycystic ovarian syndrome (PCOS) have hormonal imbalance such as higher estrogen levels and lower
levels of progesterone. The increase in estrogen compared to progesterone can increase a woman's chance of getting endometrial cancer. Age – The risk of endometrial cancer increases as a woman gets older. Diabetes – Diabetes occurs more commonly among people who are overweight. This could be the reason why diabetes is a risk factor for endometrial cancer. Endometrial cancer may be as much as four times more common in women with diabetes. Although diabetes is more common in people who are overweight, even diabetics with normal body weight have a higher risk of developing endometrial cancer. Some studies suggest that diabetes by itself could also be a risk factor. Family history – Endometrial cancer tends to run in some families with an inherited tendency to develop colon cancer, a disorder called hereditary nonpolyposis colon cancer (HNPCC), or Lynch syndrome. In most cases, this disorder is secondary to a defect in either the gene MLH1 or the gene MSH2. At least 5 other genes can cause HNPCC, namely MLH3, MSH6, TGBR2, PMS1, and PMS2. An abnormal copy of any one of these genes reduces the body's ability to repair any damage to its DNA, resulting in a very high risk of colon cancer, as well as a high risk of endometrial cancer. Women with this syndrome have a 40% to 60% risk of developing endometrial cancer some time during their lives. The risk of ovarian cancer is also increased. A person who has a family history of colon cancer or endometrial cancer may opt to have genetic counseling and testing for HNPCC to determine whether the individual is at high risk for the development of endometrial cancer. The American Cancer Society guidelines recommend that women with known or suspected (based on family history) HNPCC consider beginning endometrial sampling at age 35, and that their physicians offer this test and explain its benefits, risks, and limitations. Another option for a woman who has (or may have) HNPCC is to have the uterus removed (prophylactic hysterectomy) once childbearing has been completed. Breast or ovarian cancer – Women who have had breast cancer or ovarian cancer may have a higher risk of getting endometrial cancer. Some of the risk factors for breast and ovarian cancer also increase endometrial cancer risk. Endometrial hyperplasia – Endometrial hyperplasia is an increased growth of the endometrium. Mild or simple hyperplasia, the most common type, has a very small risk of becoming cancerous. It may spontaneously resolve without treatment, or may need hormone therapy. If the hyperplasia is called "atypical", it has a higher chance of becoming cancer. Simple atypical hyperplasia develops into cancer in about 8% of cases if not treated. Complex atypical hyperplasia, on the other hand, has a risk of becoming cancerous in up to 29% of cases in the absence of treatment. Q: What causes endometrial cancer? A: The exact cause of most cases of endometrial cancer is still unknown. A great deal of research is currently ongoing in order to learn more about the disease. Most endometrial cancer cells contain estrogen and/or progesterone receptors on their surfaces. Somehow, interaction of these receptors with their hormones leads to increased growth of the endometrium, particularly if hormonal imbalance occurs. This can mark the beginning of the development of cancer. Q: Can endometrial cancer be prevented? A: Most cases of endometrial cancer cannot be prevented. However, there are several ways to lower one’s risk of developing this disease. One is to change the risk factors whenever possible. Weight loss may reduce the risk of this type of cancer in women who are obese. A healthy diet and regular exercise can also lower endometrial cancer risk. Women who exercise on a daily basis can decrease their risk into half compared to women who do not exercise.
Controlling diabetes, if present, may also help reduce the risk. Estrogen is available in many different forms to treat the symptoms of menopause, such as pills, skin patches, creams, and vaginal rings. Prior to using this hormone for menopausal symptoms, one should consult her physician first to discuss how this will affect one’s risk of endometrial cancer. Although the additional use of progestins can reduce the risk of endometrial cancer in women taking estrogen therapy, this combination had been found to case an increase in the risk of breast cancer. Also, obtaining prompt treatment for pre-cancerous disorders of the endometrium is another way to lower the risk of endometrial cancer. Most endometrial cancers develop over a period of years. Many are known to follow and possibly start from less serious abnormalities of the endometrium called endometrial hyperplasia. Some cases of hyperplasia will resolve spontaneously without treatment. Other types will require treatment with hormones or even surgery. Treatment with progestins and a dilation and curettage (D & C) or hysterectomy can prevent hyperplasia from becoming cancerous. Abnormal vaginal bleeding is the most common symptom of endometrial pre-cancers and cancers, and it needs to be reported and evaluated right away. Q: Can endometrial cancer be detected early? A: In most cases, being alert to any signs and symptoms of endometrial cancer, such as abnormal vaginal bleeding or discharge, and seeking immediate consult allows the disease to be diagnosed at an early stage. Early detection improves the chances of successful treatment. However, some endometrial cancers may reach an advanced stage before signs and symptoms are evident. Women at average endometrial cancer risk – At present, there are no tests or exams that can detect endometrial cancer early in women who are at average risk and have no symptoms. The American Cancer Society recommends that, at the time of menopause, all women should be informed of the risks and symptoms
of endometrial cancer and strongly encouraged to report any vaginal bleeding or spotting to their physician. Women should talk to their physicians about having regular pelvic exams. Although the pelvic exam can find some cancers, including some advanced uterine cancers, it is not very effective in finding early endometrial cancers. Although the Pap test can find some early endometrial cancers, it is not a good test for this type of cancer. Women at increased endometrial cancer risk – The American Cancer Society recommends that most women at increased risk should be informed of their risk and advised to see their physician whenever there is any abnormal vaginal bleeding. This includes women whose risk of endometrial cancer is increased due to increasing age, late menopause, never giving birth (nulliparous), infertility, obesity, diabetes, hypertension, estrogen treatment, or tamoxifen therapy.
Women who have (or may have) hereditary nonpolyposis colon cancer (HNPCC) have a very high risk of endometrial cancer. These women should be offered yearly testing for endometrial cancer with endometrial biopsy beginning at the age of 35. This includes women known to carry HNPCC-linked gene mutations, women who are likely to carry such a mutation (those with a mutation known to be present in the family), and women from families with a tendency to get colon cancer where genetic testing has not been done. Another option for a woman who has (or may have) HNPCC is to have a hysterectomy once childbearing has been completed. One study found that none of 61 women who had prophylactic hysterectomies developed endometrial cancer, while 1/3 of the women who did not undergo surgery eventually had endometrial cancer. Q: How is endometrial cancer diagnosed? A: There is no screening test that has been recommended in order to detect this cancer before symptoms develop (except for women at high risk). Routine pelvic exams rarely discover this disease. Most women are diagnosed once they have symptoms. Signs and symptoms of endometrial cancer
Unusual bleeding, spotting, or other discharge – A menopausal woman should seek immediate consultation for any unusual vaginal bleeding, spotting, or discharge. About 90% of patients diagnosed with endometrial cancer have abnormal vaginal bleeding such as bleeding between periods (intermenstrual bleeding) or after menopause. Non-bloody vaginal discharge may also be a sign of endometrial cancer, which can be found in about 10% of cases. Pelvic pain and/or mass and weight loss – These symptoms are more common in the advanced stages of the disease. Still, any delay in seeking medical help may allow the disease to progress even further, thus lowering the chances for successful treatment. Seeing a specialist
If the physician is highly considering the presence of endometrial cancer, the woman must be examined by a gynecologist, a doctor qualified to diagnose and treat diseases of the female reproductive system. Specialists in treating cancers of the endometrium and other female reproductive organs are called gynecologic oncologists. Sampling endometrial tissue
To find out whether endometrial hyperplasia or endometrial cancer is present, the doctor must remove some tissue so that these can be examined under a microscope. Endometrial tissue can be obtained through either an endometrial biopsy, or by dilation and curettage (D & C). Endometrial biopsy – An endometrial biopsy is the most commonly performed test for endometrial cancer. It can be done in the office or clinic without any form of anesthesia. A very thin flexible tube is inserted into the uterus through the cervix. Using suction, a small amount of endometrium is removed through the tube. Others use a rigid instrument to scrape a little amount of the endometrial lining. The discomfort is similar to menstrual cramps and can be diminished with intake of a nonsteroidal anti-inflammatory drug such as ibuprofen before the procedure. Dilation and curettage (D & C) – If the endometrial biopsy sample does not provide enough tissue, or if the biopsy suggests cancer but the results are uncertain, a D & C must be performed. This procedure requires general anesthesia or conscious sedation, performed in an outpatient surgery area of a clinic or hospital. The opening of the cervix is enlarged (dilated) and a special instrument is inserted into the uterine cavity to scrape tissue from the endometrial lining. Most women have little discomfort after this procedure. Testing of endometrial tissue Endometrial tissue samples removed by biopsy or D & C are examined under the microscope. Endometrial cancer is graded based on how much it looks like a normal endometrium. It is called grade 1 if 95% or more of the cancer forms glands similar to those of normal endometrial tissue. Grade 2 tumors have between 50% and 94% gland formations. Cancers with less than half of the tissue forming glands are given a grade of 3. Women with lower grade cancers are less likely to have advanced disease or recurrences. Tests for endometrial cancer Transvaginal ultrasound – Ultrasound uses sound waves to obtain images of parts of the body. For a transvaginal ultrasound, a probe that gives off sound
waves is inserted into the vagina, creating images of the uterus and other pelvic organs. These images often help demonstrate the character and thickness of the endometrial lining, whether a tumor is present, or whether it is growing into the muscle layer of the uterus (myometrium), or adjacent structures. Cystoscopy and proctoscopy – If a woman experiences symptoms that suggest the cancer has spread to the bladder or rectum, the lining of these organs can be visualized through a lighted tube. In cystoscopy, the tube is placed into the bladder through the urethra. In proctoscopy, the tube is inserted into the rectum. Small tissue samples can also be obtained during these procedures for pathologic (microscopic) testing if suspicious or abnormal areas are noted. Computed tomography (CT) – The CT scan is an x-ray procedure that creates detailed, cross-sectional images of the body. It is not used to diagnose endometrial cancer, but may be used to delineate spread of the disease to other organs. It can also be utilized in detecting tumor recurrence after treatment. A CT scan can also be used to precisely guide a biopsy needle into a suspected area of cancer spread. Magnetic resonance imaging (MRI) – MRI scans use radio waves and strong magnets instead of x-rays. The energy from the radio waves is absorbed and then released in a pattern formed by the type of tissue and by certain diseases. A computer translates the pattern of radio waves given off by the tissues into a very detailed image of parts of the body, creating cross sectional slices of the body like a CT scanner. It also produces slices that are parallel with the length of the body. This procedure is particularly helpful in detecting tumors within the brain, spinal cord, and other soft tissue structures such as lymph nodes. Positron emission tomography (PET) – In this test, radioactive glucose (sugar) is administered to the patient to look for cancer cells. Because cancers use glucose (sugar) at a higher rate than normal tissues, the radioactivity will tend to concentrate in the tumor. A scanner is used to spot the radioactive deposits. This test can be helpful for locating small foci of cancer cells. However, PET scans are not routinely ordered, and their role in endometrial cancer is still under investigation. Chest x-ray – This test can show whether the cancer has spread to the lungs. It may also be used to look for serious lung or heart problems, particularly prior to surgery. Intravenous pyelogram (IVP) – This is an x-ray of the urinary system taken after injecting a special dye into a vein. This dye is removed from the bloodstream by the kidneys and passes through the ureters into the bladder (the ureters are the tubes that connect the kidneys to the bladder). It is useful in detecting abnormalities of the urinary tract, such as changes caused by spread of
cancer to the pelvic lymph nodes, which may compress or block a ureter. IVP is rarely used in the initial evaluation of patients with endometrial cancer. CA 125 blood test – CA 125 is a substance released into the blood stream by many, but not all, endometrial and ovarian cancers. An elevated CA 125 level suggests that an endometrial cancer has probably spread beyond the uterus. Some physicians will utilize this in deciding whether surgery should be done by a gynecologic oncologist. Furthermore, if levels are elevated prior to surgery, serial measurements can be obtained post-operatively and during adjuvant treatment in order to determine how well the treatment is working (levels will drop after surgery if treatment is effective). Follow-up measurements can also be requested after completion of treatment to detect early tumor recurrences. Q: How is endometrial cancer staged? A:Staging is a universal system used to describe how far the cancer has spread. The stage of an endometrial cancer is the most important factor in choosing a treatment plan. The main system used to stage endometrial cancer is called the FIGO (International Federation of Gynecology and Obstetrics) system. This is a surgical staging system, and is based on examination of the tissues removed during the operation. Although several tests may be requested prior to the surgery (ultrasound, MRI, CT scan) to detect spread of the tumor to distant sites, this information can be helpful in planning surgery and other treatment and cannot be used for staging the disease. The staging system looks at how far the cancer has spread. It can spread locally to other parts of the uterus. It can also spread regionally to nearby lymph nodes found in the pelvis and along the aorta. Finally, the cancer can spread (metastasize) to distant lymph nodes or organs such as lung, liver, bone, brain, and other organs. Below is the 1988 FIGO surgical staging system for endometrial cancers:
Tumor confined to the body of the uterus
Tumor invades up to less than half of myometrium
Tumor invades to more than one half of myometrium
Tumor invades the cervix but does not extend beyond uterus
Local and/or regional spread as specified in IIIA, B, C
Tumor involves serosa and/or adnexa (direct extension or metastasis) and/or cancer cells in ascites or peritoneal washings
Vaginal involvement (direct extension or metastasis)
Metastasis to pelvic and/ or para-aortic lymph nodes
Tumor has spread to the bladder and/or bowel mucosa or to
Tumor invasion of bladder and/ or bowel mucosa
Distant metastasis (excluding metastasis to vagina, pelvic serosa, or adnexa, including metastasis to intra-abdominal lymph nodes other than para-aortic and/or inguinal nodes)
Survival by stage
The 5-year survival rate refers to the percentage of patients who live at least 5 years after a diagnosis of malignancy has been made. These rates are used to create a standard way of discussing prognosis. However, many of these patients live much longer than 5 years from the time of diagnosis. Improvements in treatment may result in a better treatment outcome for recently diagnosed patients. Relative 5-year survival rates by stage for endometrial adenocarcinoma are as follows:
Q: How is endometrial cancer treated? A: The choice of treatment depends largely on the type of cancer and stage of the disease at the time of diagnosis. Other factors that are taken into consideration in choosing the best treatment plan include the patient’s age, overall state of health, plans for future childbearing, and other personal considerations. There are four basic types of treatment for women with endometrial cancer: surgery, radiation therapy, chemotherapy and hormonal therapy. Surgery is the main treatment for most women afflicted with this disease. In certain situations, however, a combination of these treatments may be used. SURGERY Hysterectomy – The main treatment for endometrial cancer is an operation to remove the uterus and cervix (called a hysterectomy). When the uterus is removed through an incision in the abdomen, it is called a simple or total abdominal hysterectomy (TAH). If the uterus is removed through the vagina, it is known as a vaginal hysterectomy. A radical hysterectomy is done when endometrial cancer has spread to the cervix or the area around the cervix (the parametrium). In this type of operation, the entire uterus, the tissues adjacent to the uterus (parametrium and uterosacral ligaments), and the upper part of the vagina (next to the cervix) are all removed. Bilateral salpingo-oophorectomy – This operation removes both fallopian tubes and both ovaries. This procedure is usually done at the same time the uterus is removed (either by simple hysterectomy or radical hysterectomy) to treat endometrial cancers. Removal of both ovaries will lead to menopause if the patient has not done so already. Lymph node surgery Pelvic and para-aortic lymph node dissection – This operation removes lymph nodes from the pelvis and the area adjacent to the aorta to detect cancer cells that have spread from the endometrial tumor. This procedure is usually done at the same time as the operation to remove the uterus. If the patient is having an abdominal hysterectomy, the lymph nodes can be removed through the same incision. In women who have had a vaginal hysterectomy, these lymph nodes may be removed by laparoscopic surgery. In a lymph node dissection, most or all of the lymph nodes in a certain area are removed. When only a few of the lymph nodes in an area are removed, it is called lymph node sampling. Laparoscopic lymph node sampling – Laparoscopy is a technique that allows the surgeon to inspect the abdominopelvic cavity through tubes inserted into very small incisions. Small surgical instruments can be controlled through the tubes, allowing the surgeon to remove lymph nodes. This approach avoids the need for a large incision in the abdomen, and so can shorten the time needed for recovery from surgery. This procedure is done when hysterectomy is accomplished via the vaginal route. Studies are in progress to determine whether sampling lymph nodes by laparoscopy is comparable with the usual operations for endometrial cancer. Meanwhile, many oncologists feel that laparoscopic lymph node sampling is as effective, and are offering this procedure as an option to their patients. In early studies with short-term follow-up, women who underwent laparoscopic surgery have had the same cure rate as those who had abdominal surgery, with reduced side effects and complications from the operation.
Pelvic washings – In this procedure, the surgeon "washes" the abdominal and pelvic cavities with salt water (saline) and sends the fluid to the laboratory to determine if it contains cancer cells. Other procedures that may be used for staging Omentectomy – The omentum is a layer of fatty tissue that covers the abdominal contents like an apron. When this tissue is removed, it is called an omentectomy. This procedure is sometimes performed to determine tumor spread into the omentum. In cases where the endometrial cancer has metastasized to the adnexa, omentectomy may also be done. Peritoneal biopsies – The tissue lining the pelvis and abdomen is called the peritoneum. Peritoneal biopsies involve removing small pieces of this lining to check for cancer cells. Tumor debulking – If cancer has spread throughout the abdomen, the surgeon may attempt to remove as much of the tumor as possible. This is called debulking. Debulking a cancer can facilitate a more efficient delivery of other treatments, like radiation or chemotherapy. Recovery after surgery For an abdominal hysterectomy, the hospital stay is usually from 3 to 7 days. The average hospital stay after a radical hysterectomy is about 5 to 7 days. Complete recovery can take about 4 to 6 weeks. A laparoscopic procedure and vaginal hysterectomy usually require a hospital stay of 1 to 2 days and 2 to 3 weeks for recovery. Complications are unusual but could include excessive bleeding, wound infection, and damage to the urinary or intestinal systems. Side effects Any hysterectomy causes infertility. For those who were premenopausal before surgery, removing the ovaries will lead to early menopause. This can cause the appearance of symptoms such as hot flashes, night sweats, and vaginal dryness. RADIATION THERAPY Radiation therapy is the use of high-energy radiation (such as x-rays) to kill cancer cells. It may be administered by placing radioactive materials inside the body near the tumor, called internal radiation therapy or brachytherapy. Another option is to deliver radiation from a machine outside the body in a procedure that is much like having an x-ray, called external beam radiation therapy. In some cases, both brachytherapy and external beam radiation therapy are given. The stage and grade of the cancer help determine what areas need to be exposed to radiation therapy and which methods are used. Brachytherapy – For vaginal brachytherapy, a cylinder containing a source of radiation is inserted into the vagina about 4 to 6 weeks after hysterectomy. With this method, the radiation mainly affects the area in contact with the cylinder, such as the vaginal cuff (the upper third of the vagina). Nearby structures such as the bladder and rectum receive less radiation exposure than the area in contact with the cylinder. There are 2 types of brachytherapy used for endometrial cancer, low-dose rate (LDR) and high-dose rate (HDR). In LDR brachytherapy, the pellets are usually left in place for about 3 days. The patient needs to stay immobile to keep the pellets from moving during treatment, and so she is usually kept in the hospital during the treatment.
In HDR brachytherapy, the radiation is more intense. Each dose takes a very short period of time (usually less than an hour), and the patient can return home the same day. For endometrial cancer, HDR brachytherapy is often given weekly or even daily for at least 3 doses. External beam radiation therapy – In this type of treatment, the radiation is delivered from a source outside of the body. This is often given 5-days-a-week for 4 to 6 weeks. The skin covering the treatment area is carefully marked with permanent ink or injected dye similar to a tattoo. A special mold of the pelvis and lower back is custom made to ensure that the woman is placed in the exact same position for each treatment. Each treatment takes less than a half-hour. Side effects of radiation therapy Common side effects of radiation therapy include tiredness, upset stomach, or loose bowels. Serious fatigue, which may not occur until about 2 weeks after treatment begins, is a common side effect. Diarrhea is likewise common, but can usually be controlled with over-the-counter medicines. Nausea and vomiting may also occur, but can be treated with medication. Side effects tend to be worse when chemotherapy is administered concurrent with the radiation. Skin changes are also common, with the skin in the treated area looking and feeling sunburned. As the radiation passes through the skin to the cancer, it may damage the skin cells, thus causing irritation ranging from mild temporary redness to permanent discoloration. The skin may also release fluid, which can subsequently lead to infection. Radiation can irritate the bladder, and problems with urination may occur. This is called radiation cystitis, and can result in discomfort and an urge to urinate often. Radiotherapy can also lead to low blood counts, causing anemia (low red blood cells) and leukopenia (low white blood cells). The blood counts usually return to normal once radiation is discontinued. Pelvic radiation therapy may cause scar tissue to form in the vagina. This scar tissue can make the vagina shorter or more narrow (called vaginal stenosis), which can make sexual intercourse painful. A woman can help prevent this problem by stretching the walls of her vagina several times a week through frequent intercourse 3 to 4 times per week, or by using a vaginal dilator (a plastic or rubber tube used to stretch out the vagina). Still, vaginal dryness and pain with intercourse can be long-term side effects from radiation. Pelvic radiation can damage the ovaries, resulting in premature menopause. However, this is not an issue for most women who are being treated for endometrial cancer, since majority are already postmenopausal, either naturally or as a result of surgery to treat the cancer (hysterectomy and removal of the ovaries).
Radiation to the pelvis can also weaken the bones, leading to fractures of the hips or pelvic bones. CHEMOTHERAPY Chemotherapy is the use of cancer-fighting drugs administered into a vein or taken by mouth. These drugs enter the bloodstream and reach all areas of the body, making this treatment potentially useful for cancer that has spread beyond the endometrium. If this treatment is chosen, a combination of drugs is usually given. Combination chemotherapy sometimes works better than a single drug alone in the treatment of cancer. Drugs used in treating endometrial cancer may include doxorubicin, cisplatin, carboplatin, and paclitaxel. Most often, 2 or more drugs are combined for treatment. The most common combinations include cisplatin and doxorubicin, paclitaxel and doxorubicin, and cisplatin/paclitaxel/doxorubicin. These drugs kill cancer cells but can also damage some normal cells, which in turn can cause side effects. Side effects of chemotherapy depend on the specific drugs, the amount taken, and the length of time of treatment. Common side effects include nausea and vomiting, loss of appetite, mouth and vaginal sores, and hair loss. Also, most chemotherapy drugs can damage the blood-producing cells of the bone marrow, resulting in low blood cell counts, such as low white blood cells (leukopenia) which increases the risk of infection, low platelet counts which can cause bleeding or bruising after minor cuts or injuries, and low red blood cells (anemia) which can cause problems like fatigue and shortness of breath. Most of the side effects of chemotherapy stop when the treatment is over, but some can last a long time. Different drugs can cause different side effects. For example, the drug doxorubicin can damage the heart muscle over time. The chance of heart damage increases as the total cumulative dose of the drug increases, such that there is only a limit or maximum dose of doxorubicin that a patient can receive. Cisplatin can cause kidney damage. Giving large amounts of fluid before and after chemotherapy can help protect the kidneys. Both cisplatin and paclitaxel can cause nerve damage (called neuropathy), leading to numbness, tingling, or even pain in the hands and feet. HORMONE THERAPY Progestins – The main hormone treatment for endometrial cancer uses progesterone-like drugs called progestins. The 2 most commonly used progestins are medroxyprogesterone acetate (Provera – injection or pill) and megestrol acetate (Megace – a pill). These act by slowing the growth of endometrial cancer cells. Side effects can include increased blood sugar levels in patients with diabetes. Hot flashes, night sweats, and weight gain (from fluid
retention and an increased appetite) can also occur. Rarely, serious blood clots are seen in patients on progestins. Tamoxifen – Tamoxifen, an anti-estrogen drug often used to treat breast cancer, may also be used to treat advanced or recurrent endometrial cancer. The goal of tamoxifen therapy is to prevent any estrogens circulating in the woman's body from stimulating growth of the cancer cells. Even though tamoxifen may prevent estrogen from nourishing the cancer cells, it acts like a weak estrogen in other areas of the body. It does not cause bone loss, but can cause hot flashes and vaginal dryness. People taking tamoxifen also have an increased risk of serious blood clots in the leg. Gonadotropin-releasing hormone agonists – Gonadotropin-releasing hormone (GNRH) agonists are another way to lower estrogen levels. These drugs switch off estrogen production by the ovaries in women who are premenopausal. Examples include goserelin (Zoladex) and leuprolide (Lupron). They are injected every 1 to 3 months. Side effects include any of the symptoms of menopause, such as hot flashes and vaginal dryness. If they are taken for a long time (years), these drugs can weaken the bones and lead to osteoporosis. Aromatase inhibitors – Even if the ovaries are removed (or are not functioning), estrogen can still be produced in fat tissue. Drugs called aromatase inhibitors can halt estrogen production by this mechanism and lower estrogen levels even further. Examples of aromatase inhibitors include letrozole (Femara), anastrozole (Arimidex), and exemestane (Aromasin). These drugs are most often used to treat breast cancer, but may be helpful in the treatment of endometrial cancer. Side effects can include hot flashes and muscle pain. If they are taken for a long time (years), they can weaken the bones and lead to osteoporosis. These drugs are still being studied, and their role in endometrial cancer treatment is not yet clear. Q: What are the treatment options for endometrial cancer? A: The following are some options that oncologists may suggest in the management of endometrial cancer after initial biopsy: STAGE I
An endometrial cancer is stage I if the cancer is limited to the body of the uterus and has not spread to lymph nodes or distant sites. If the tumor is endometrioid, standard treatment includes surgery to remove the tumor and stage the disease. Treatment after surgery depends upon the surgicopathologic stage. Treatment after complete staging
Stage IA endometrioid cancers are limited to the endometrium only and have not infiltrated into the myometrium. These cancers most often do not need any further treatment after surgery. If the tumor is grade 3, the oncologist may recommend vaginal brachytherapy. Pelvic radiation may be given as well in rare circumstances. In Stage IB, the cancer has invaded less than halfway into the myometrium. Many of these can be observed without further treatment after surgery. For high grade tumors, oncologists are more likely to recommend radiation after surgery, in the form of either vaginal brachytherapy or pelvic radiation. In stage IC, the cancer has infiltrated more than halfway through the myometrium. After surgery, the patient is usually offered pelvic radiotherapy. Patients not staged with surgery If endometrial cancer was an incidental finding after hysterectomy for a benign disease, and the procedure performed was a THBSO, further adjuvant treatment will depend on the stage and grade of tumor. For stage IA and IB well- or moderately-differentiated endometrial cancer, no further treatment is necessary. High-grade tumors, on the other hand, will require either vaginal brachytherapy (for stage IA tumors), or pelvic radiation (for stage IB tumors). However, if the tumor has invaded more than half of the myometrium (stage IC), pelvic radiotherapy is usually administered post-operatively, regardless of tumor differentiation. If lymphovascular space invasion (LVSI) was noted on the hysterectomy specimen, an option of re-exploration and lymphadenectomy may be entertained. Otherwise, adjuvant therapy may be instituted. On the other hand, if the patient underwent hysterectomy (TH) alone, and the tumor is either stage IA or IB, well- or moderately-differentiated, with no LVSI, the oncologist may opt to do re-exploration to remove the adnexa and perform complete surgical staging. Close observation with no further adjuvant treatment is also an option. If the disease is either stage IC, or poorly differentiated, with no evidence of LVSI or metastases, pelvic radiotherapy is usually administered. In the presence of LVSI or distant metastasis, however, re-operation may be the best option to allow adnexal removal and the performance of a comprehensive surgical staging so that further adjuvant treatment may be tailored accordingly. Conservative therapy in the form of high dose progestins may be used to treat early stage endometrial cancer in women younger than 40, who are still desirous of pregnancy. Medical treatment may only be offered to patients in whom the cancer is well-differentiated and of favorable histologic type (endometrioid). Lymphovascular space invasion must be absent on comprehensive microscopic examination. Imaging with contrast-enhanced MRI must demonstrate no or minimal invasion into the myometrium, and the absence of cervical or extrauterine spread. Serum CA 125 levels must be within normal limits. Furthermore, the couple must have no other concomitant problems that would
lead to infertility. Most importantly, the patient must be able to comply with the treatment and should have good follow-up with her oncologist. Patients are initially managed with a fractional curettage, followed by 3 months of high dose progestins. Repeat curettage is performed after treatment to document tumor regression, persistence or progression. If the lesion persists or progresses, then medical treatment is considered a failure, and surgery should be performed. However, patients need to understand that this is not a standard treatment and may increase risk of spread or progression of the disease. STAGE II When a cancer is stage II, it has spread to the cervix but has not grown outside of the uterus. Cervical involvement could either be occult/microscopic (endocervical curettage shows the presence of tumor cells with histologic continuity to normal endocervical tissue) or gross. Options of surgical treatment for occult/microscopic cervical involvement include either an extrafascial or a radical hysterectomy with a complete surgical staging procedure. The advantage of performing a radical hysterectomy is that it will obviate the need for adjuvant radiotherapy for surgical stage II disease since more parametrial tissues have been resected. This surgical approach is preferred in areas with no facilities for radiation. On the other hand, patients who underwent extrafascial hysterectomy will require postoperative pelvic radiotherapy. For patients whose cervix is grossly infiltrated by tumor, radical hysterectomy with surgical staging is also the recommended procedure. However, for poor surgical risk patients, pre-operative complete radiotherapy (pelvic radiation followed by vaginal brachytherapy) followed by extrafascial hysterectomy and lymph node assessment is an acceptable alternative. These latter patients are staged according to the 1971 FIGO clinical staging of endometrial cancer. STAGE III Stage III cancers have spread outside of the uterus, but the tumor is still confined within the pelvis. Standard treatment even for advanced disease is still hysterectomy and comprehensive surgical staging. In the presence of adnexal involvement, the omentum is removed as well. Any remaining tumor is removed during surgery to achieve optimal debulking. Stage IIIA: If the cancer is confined to the uterus, but pelvic washings obtained during laparotomy demonstrate the presence of cancer cells, the disease is stage IIIA. In the absence of other poor prognostic factors (unfavorable histologic type, poorly differentiated tumor, presence of LVSI, deep myometrial invasion), no other treatment may be needed after surgery. On the other hand, if any of the abovementioned prognostic factors is present, chemotherapy followed by pelvic radiation is usually administered.
A cancer is also considered stage IIIA when it has spread to other tissues in the pelvis like the fallopian tubes and the ovaries. When this occurs, treatment after surgery may include a combination of chemotherapy followed by radiation. Stage IIIB: In this stage, the cancer has spread to the vagina. After surgery, stage IIIB patients may be treated with combination chemotherapy, pelvic radiation, and vaginal brachytherapy. Stage IIIC: When the cancer has spread to the lymph nodes in the pelvis or around the aorta, it is stage IIIC. Treatment includes surgery, followed by combination chemotherapy, extended field radiation (includes pelvic and para- aortic fields) and vaginal brachytherapy. STAGE IV These cancers have grown into the bladder or bowel (stage IVA), or spread to distant sites like liver, lungs, etc. or to lymph nodes outside of the pelvis or para- aortic area (stage IVB). The patient may have the best chance if all grossly visible tumor seen during laparotomy can be removed and biopsies of the abdomen do not show cancer cells. This may be possible if the cancer has spread to lymph nodes in the abdomen and pelvis only. However, in most cases of stage IV endometrial cancer, the extensive spread of the disease makes a surgical cure nearly impossible. Nevertheless, a hysterectomy and bilateral salpingo-oophorectomy may still be performed in order to prevent excessive bleeding. This is followed by chemotherapy and complete radiotherapy (extended field radiotherapy followed by brachytherapy). When the cancer has spread to other parts of the body, hormone therapy such as progestins and tamoxifen, may be given as well. Combinations of chemotherapy drugs may help for a time in some women with advanced endometrial cancer. The drugs used most often are doxorubicin, paclitaxel, and either cisplatin or carboplatin. These drugs are often used together in combination. Women with stage IV endometrial cancer should consider taking part in clinical trials of chemotherapy or other new treatments. POOR HISTOLOGIC TYPES Tumors of poor histologic types, such as papillary serous carcinoma or clear cell carcinoma, are more likely to have spread outside of the uterus at the time of diagnosis, and thus have poorer prognosis. The surgery may be more extensive such that in addition to the TH/BSO and the pelvic and para-aortic lymph node dissections, the omentum is often removed and peritoneal biopsies are obtained. After surgery, both chemotherapy and radiation therapy are often given to help keep the cancer from recurring. The chemotherapy usually includes the drugs cisplatin and doxorubicin. Paclitaxel may be given as well. RECURRENT ENDOMETRIAL CANCER When a cancer has gone away with treatment, but then comes back later, it is called recurrent. Treatment depends on the size of the lesion, and location of the tumor. If the recurrent cancer is only in the pelvis, radiation therapy may provide a cure. Women with more extensive recurrences are treated like those with stage IV endometrial cancer. Either hormone therapy or chemotherapy is recommended. Low-grade cancers containing progesterone receptors are more likely to respond well to hormone therapy. Higher-grade cancers and those without detectable receptors are less likely to shrink during hormone therapy, but may respond to chemotherapy. Clinical trials of new treatments are another option. Q: What will happen after treatment for endometrial cancer? A: An important part of the treatment plan is a specific schedule of follow-up visits after surgery, chemotherapy, or radiation therapy. During the first 2 years after treatment, follow-up visits are usually scheduled for every 3 to 4 months. About 75% of endometrial cancer recurrences are found within the first 2 years of follow-up. Later on, recurrence is less likely and follow-up visits are scheduled less often, usually twice yearly. During each follow-up visit, it is important to report any symptom (vaginal spotting, vaginal discharge, abdominal pain, weight loss, anorexia, etc) that might suggest a tumor recurrence, as well as any side effect of treatment. A pelvic exam is performed to detect any abdominal or vaginal mass, or look for any enlarged lymph nodes in the groin area. A Pap test may also be done to look for cancer cells in the vagina vault. If symptoms or physical exam suggest a possible recurrence, imaging tests (CT scans, ultrasound studies), a CA 125 blood test, and/or biopsies may be done. Studies of patients with endometrial cancer show that in the absence of symptoms or abnormal physical exam findings, routine blood tests and imaging tests are not necessary. Hormone therapy may be given to symptomatic women who have been treated for endometrial cancer. Studies have shown that the absolute recurrence rate after hormone replacement therapy for early stage (stage I and II) endometrial cancers is only 2.1%, and the incidence of development of a new malignancy is very low. It is also helpful to adopt lifestyle modification during or after treatment. One of the best things that can be done is to put healthy eating habits into place, like increasing the variety of healthy foods. Eat five or more servings of vegetables and fruits each day. Choose whole grain foods instead of white flour and sugars. Limit meats that are high in fat. Cut back on processed meats like hot dogs, bologna, and bacon. Limit alcohol intake. Adopt a regular exercise plan. Studies have shown that patients who follow an exercise program tailored to their personal needs feel physically and emotionally improved and can cope better.
Exercise can improve physical and emotional health by improving cardiovascular (heart and circulation) fitness, strengthening the muscles, reducing fatigue, and lowering anxiety and depression. The American Cancer Society, in its guidelines on physical activity for cancer prevention, recommends that adults take part in at least one physical activity for 30 minutes or more on 5 days or more of the week. Children and teens are encouraged to try for at least 60 minutes a day of energetic physical activity on at least five days a week. Q: What happens if treatment is no longer working? A: If cancer continues to grow after one kind of treatment, or if it returns, it is often possible to try another treatment plan that might still cure the cancer, or at least shrink the tumors enough to help the patient live longer and feel better. On the other hand, when a woman has received several different medical treatments and the cancer has not been cured, over time the cancer tends to become resistant to all treatment. At this time it is important to weigh the possible limited benefit of a new treatment against the possible disadvantages, including continued doctor visits and treatment side effects. Everyone has a different way of looking at a situation like this. Some patients may want to focus on remaining comfortable during their limited time left, especially if continuing treatment will not likely improve health or change the prognosis or survival. In such cases, most oncologists recommend treatment directed to any symptom that the patient might have, particularly pain. This type of treatment is called "palliative" treatment. Palliative treatment helps relieve these symptoms, but is not expected to cure the disease. It is primarily given to improve a patient’s quality of life. Sometimes, the treatment to control symptoms is similar to the treatments used to treat cancer. For example, radiation therapy might be given to help relieve bone pain from bone metastasis. Or chemotherapy might be given to help shrink a tumor and keep it from causing a bowel obstruction. However, this is not the same as receiving treatment to try to cure the cancer. Q: What’s new in endometrial cancer research and treatment? A: Molecular pathology Recent research has improved our understanding of how changes in certain molecules can cause normal endometrial cells to become cancerous. It has been known for several years that damaged or defective DNA (called mutations) can alter important genes that regulate cell growth. If these genes are damaged, out-of-control growth may result in cancer.
Some endometrial cancer and colon cancer cases may seem to "run in a family" who have an inherited defect in certain genes that normally help repair damage to DNA. If these repair enzymes are not working properly, damage to DNA is more likely to persist and cause cancer. Similar DNA repair defects have also been found in endometrial cancer cells from some patients without an inherited tendency to develop this disease. One of the normal genes responsible for suppressing tumor growth, called PTEN, is often abnormal in endometrial cancers. Tests for this and other DNA changes may some day help detect endometrial cancers early. Endometrial cancers without other tumor suppressor genes (or with inactive ones), such as the retinoblastoma (Rb) gene and the p53 gene, tend to be more likely to recur after initial treatment. Tests for these and other DNA changes may some day be used to help predict how aggressive the cancer might be and to select the best treatment for each patient with this disease. The long-range goal of this field of research is gene therapy that can correct the DNA abnormalities that caused the endometrial cells to become malignant. Tumor markers Molecules released by cancer cells to the circulation can help detect recurrence of some types of cancer. For example, CA 125 is a useful marker in finding recurrent ovarian cancer. Recent studies demonstrate that blood tests for CA 125 may also be helpful in finding recurrent endometrial cancer, before tumor deposits are visible by CT or MRI scans. Measuring CA 125 levels in some patients before surgery may also be helpful if it appears the cancer may have spread. New treatments Researchers are examining new drugs, combinations of drugs and "targeted therapies" in patients with advanced endometrial cancer. The use of adjuvant chemotherapy, with or without radiation is also under investigation.
Arantza MENDIZABAL GOROSTIAGA TERRORISMO: Un desafío para la democracia ANTECEDENTES En España después de la muerte del dictador se inició un proceso de transición a la democracia ejemplar. Un proceso de recuperación de las libertades y de construcción de un país plural y tolerante. Los rescoldos del franquismo fueron desapareciendo, sólo quedaba ETA. El grupo terrorista
Welcome-So very glad to be here! It’s hard to believe that it has been almost a year since I have been with you all! I miss my daily visits to the City working with Sherry and our monthly coalition meetings together. Do know, I think of you all often and I am always ready to answer any questions Brooke or Natalie may have! My family looks back on our time with SCHEC with great memories. I will U
 Q: What is endometrial cancer?
Q: What is endometrial cancer?