Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Ncpneph_2005_105.indd
Fatal hyponatremia in a young woman after ecstasy ingestion Kamyar Kalantar-Zadeh*, Minhtri K Nguyen, Roger Chang and Ira Kurtz
This article offers the opportunity to earn one Category 1 credit toward the AMA Physician’s
Background A 20-year old, otherwise healthy, female college student presented in an unresponsive state with respiratory distress after ingesting ecstasy (3,4-methylenedioxymethamphetamine). She had initial plasma sodium concentration of 117mmol/l.
In 2002, a 20-year-old, Asian American woman
Investigations Physical examination, blood chemistry panel, urinary
was brought to the emergency room at Harbor-
osmolality and electrolytes, arterial blood gas, chest X-ray, and CT scan of the brain.
multiple tablets of ecstasy (3,4-methylene-
Diagnosis Hyponatremia associated with noncardiogenic pulmonary edema and cerebral edema.
quantities of water while dancing and drinking excessively during a party the night before. She
Management Administration of a total of 6.8l of isotonic saline and 0.245l
did not report any symptoms upon returning
of 3% hypertonic saline with sporadic administration of intravenous
home after the party. In the morning, however,
furosemide. The patient died approximately 12h after admission.
she was found unresponsive and foaming at the
KEYWORDS ecstasy, estrogen, hyponatremic encephalopathy, MDMA, noncardiogenic pulmonary edema
mouth although no seizures were reported. She had rapid and shallow breathing, a weak pulse
and did not respond to painful stimuli. The patient was otherwise healthy, with no medical or surgical history or significant family history. She was not taking any medications and was a college student of good standing.
In the emergency room the patient was found to
be in respiratory distress (respiratory rate 30–35 breaths per minute), hypothermic (temperature 34.7 °C), tachycardic (pulse 123 beats per minute), hypotensive (blood pressure 88/49 mmHg), hypoxemic (oxygen saturation 80% on a non rebreather mask), and nonedematous. Her pupils were symmetrically dilated and minimally reactive to light. No jugular venous distention was
K Kalantar-Zadeh is an Associate Professor of Medicine and Pediatrics and
noted. Chest auscultation revealed diffuse crackles
Director of the Dialysis Expansion Program and Epidemiology at Harbor-UCLA
bilaterally. The patient was intubated. Division of Nephrology and Hypertension, MK Nguyen (co-primary author)
Table 1 shows results of initial plasma electro-
is an Assistant Professor of Medicine and Director of Consultative Nephrology
lyte measurements and arterial blood gas analy ses
in the Division of Nephrology, and I Kurtz is Chief of Nephrology, Professor of
and how these results changed over time with
Medicine, Factor Chair in Molecular Nephrology, and Director of the Molecular Physiology and Biophysics Transport Laboratory at UCLA, Torrance, CA.
treatment. Initial laboratory examination also
R Chang is a hospitalist at St Joseph’s Hospital in Orange, CA, USA.
revealed a blood urea nitrogen (BUN) level of 6.4 mmol/l, a serum glucose level of 5.75 mmol/l,
Correspondence
and a serum calcium level of 1.95 mmol/l.
*Harbor-UCLA Medical Center, UCLA David Geffen School of Medicine, 1124 W Carson St, C-1 Annex, Box 406, Torrance, CA 90502-2064, USA
The patient had an initial serum osmolality of
245 mOsm/kg, urine specific gravity of 1.015, a white blood cell count of 18,300 cells/mm3,
Received 1 July 2005 Accepted 20 February 2006
a hemoglobin concentration of 133 g/l, and a
www.nature.com/clinicalpracticedoi:10.1038/ncpneph0167
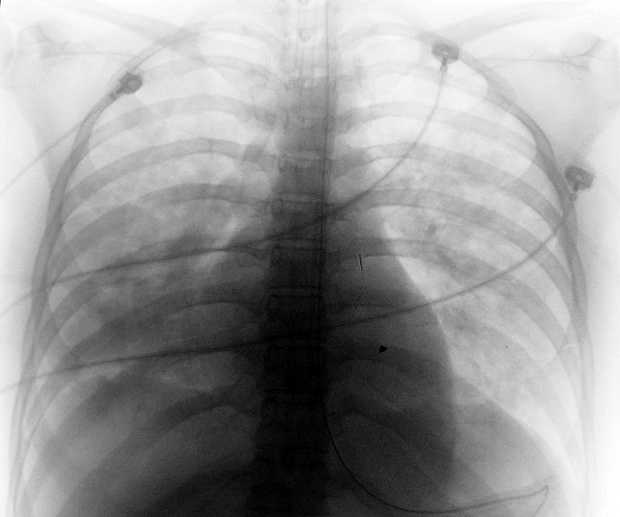
platelet count of 310,000 cells/mm3. The chest
2006 Nature Publishing Group Table 1 Chronologic course of events in the patient after ecstasy (3,4-methylenedioxymethamphetamine) ingestion. Chemistry panel Arterial blood gas Events and intravenous Na (mmol/l; Cl (mmol/l; Creatinine pO (mmHg; (mmol/l; (μmol/l; range: 135– range: 95– range: 80– 145mmol/l) 105mmol/l) range: 22– range: 50– 7.35–7.45) range: 38– 100mmHg) 26mmol/l) 120μmol/l)
Approximately 1 l normal saline in the ambulance
normal saline upon arrival in emergency room
20 ml 3% hypertonic saline in intensive care unit
saline plus furosemide following nephrology consultation
pressure increased to 23 cm, intravenous fluids discontinued
GLOSSARY
X-ray showed severe pulmonary edema (Figure 1).
concentration [Na+] increased to 129 mmol/l
NONCARDIOGENIC
A CT scan of the head showed evidence of
after 10 h of hospitalization, but the patient’s
PULMONARY EDEMA
hemodynamic status remained unstable; 12 h
A status of pulmonary vascular congestion and/or
The patient was given a total of 6.8 l of isotonic
after admission, she was found to have wide-
saline and 0.245 l of 3% hypertonic saline with
complex tachycardia, which was followed by
intermittent administration of furosemide and
pulseless electrical activity. Resuscitation efforts
60 g of mannitol (Table 1). Plasma sodium
were unsuccessful, and the patient expired.
KALANTAR-ZADEH ET AL. MAY 2006 VOL 2 NO 5
2006 Nature Publishing Group DISCUSSION OF DIAGNOSIS Hyponatremia can lead to increased intracranial pressure, which might trigger the development of neurogenic pulmonary capillary leak and result in noncardiogenic pulmonary edema. Cardiogenic pulmonary edema is highly unlikely in a young woman with no medical history of cardiovascular, pulmonary or renal disease. Encephalopathy is thought to result from brain edema caused by movement of water into the brain cells. Hyponatremic encephalopathy can also manifest as hypercapnic respiratory failure.1 Even in chronic symptomatic hyponatremia, hypoxia can play a crucial role in morbidity and mortality.2 The encephalopathic patient with hyponatremia usually presents with head- ache, nausea, vomiting, abdominal pain, confu- sion, and seizures, which can lead to permanent neurologic sequelae and imminent death due to brain edema and subsequent herniation.
Several factors that might contribute to
Figure 1 Chest X-ray of 20-year-old woman with a plasma sodium concentration
in Box 1. Profuse sweating at a ‘rave party’ can
of 117 mmol/l after ecstasy (3,4-methylenedioxy methamphetamine) ingestion.
lead to excessive water intake, which ultimately
Note the cephalization of pulmonary vasculature consistent with pulmonary
results in a decreased concentration of sodium
edema, which is noncardiogenic in this case.
in the blood.3 Up to 2 l of perspiration can be lost per hour in a hot environment, especially during intense physical activity such as dancing.4
Box 1 Factors that might contribute to fatal hyponatremia following ecstasy
If MDMA in some way also inhibits perspira-
(3,4-methylenedioxymethamphetamine [MDMA]) ingestion.
tion, hyponatremia is more likely to occur. A
Excessive fluid intake in response to central polydipsia (effect of MDMA on
the central nervous system) or polydipsia as a result of perspiration during
also stimulate thirst and cause primary poly-
rigorous physical activity (e.g. dancing)
dipsia independent of perspiration or ambient
Fluid third-spacing in the GI tract (ileus) with subsequent abrupt water
temperature.5 Moreover, partygoers are usually
encouraged to drink large volumes of water to avoid dehydration.4
As in marathon runners, excess antidiuretic
Overproduction and/or release of antidiuretic hormone either in response to,
hormone (ADH, also known as vasopressin)
or independent of, rigorous physical activity
release can result from rigorous physical activity
Administration of hypotonic or isotonic intravenous fluids
such as dancing. MDMA can trigger inappro-priate secretion of ADH independent of the
degree of physical activity. In a study of eight
healthy drug-free male volunteers Fallon et al.
Estrogenic hormones (in menstruating women)
showed that concentrations of plasma argi-nine vasopressin increase significantly after
Higher intracellular brain volume (relative to older women) or absence of
In MDMA users, gastrointestinal motility can
decrease, resulting in a large static volume of electrolyte-free water in the lumen of the gastro-intestinal tract.4,7 An ileus with a 2-cm radius would lead to a 7-l water intake and its retention
of physical activity (e.g. at the end of a dance
in the lumen of the stomach and small intestine.4
This retained water might be absorbed abruptly
through the gastrointestinal tract upon cessation
hyponatremia have been reported;8–12 most of
MAY 2006 VOL 2 NO 5 KALANTAR-ZADEH ET AL.
2006 Nature Publishing Group Table 2 Comparison of clinical and laboratory findings, course of events, and management and outcome of three hyponatremic patients. MDMA user Marathon runner Post-surgical patient
preoperatively and postoperatively to avoid hypoglycemia
no jugular venous distention, bilateral basilar crackles on chest auscultation
discontinued, 40 mg intravenous furosemide administered
in 6 h) with no sequelae, discharged after 1 day
MDMA, 3,4-methylenedioxymethamphetamine; [Na+], sodium concentration; SG, urine specific gravity; UOsm, urine osmolality.
these cases were premenopausal women.8–12
reported to be 30 times greater for women than
This finding is consistent with the findings of
for men, and 25 times greater for menstruant
‘Ayus–Arieff syndrome’, in which women of
females than for postmenopausal females.13 The
this age develop noncardiogenic pulmonary
higher morbidity and mortality rates among
edema, hypoxemia and brain edema.13,14 The
relative risk of death or permanent neurological
to the effects of estrogenic hormones, via
damage from hyponatremic encephalopathy is
two possible mechanisms: (1) inhibition of
KALANTAR-ZADEH ET AL. MAY 2006 VOL 2 NO 5
2006 Nature Publishing Group
cerebral Na+/K+-ATPase activity, which impairs
Are there signs and symptoms of pulmonary edema
the ability of brain cells to extrude sodium
(dyspnea, hypoxemia, congestion) or cerebral edema (headache)?
in the initial defense of cell volume; and (2) increased vasoconstriction of cerebral blood vessels by vasopressin, which leads to decreased brain perfusion.15,16
The gender discrepancy could also be due
to the fact that women have less muscle mass than men. As half of total body water is located in skeletal muscle cells, an individual with low muscle mass is at high risk for development
of severe hyponatremia when a given volume
of electrolyte-free water is retained.4 Individuals
Figure 2 Algorithm for treatment of premenopausal women with hyponatremia.
with muscle atrophy resulting from illness or a nutritional problem (e.g. anorexia nervosa) are also at risk. In addition, differences in brain adaptation could account for part of the gender
Box 2 The Nguyen-Kurtz equation can predict post-intervention plasma
discrepancy—women are less able to adapt to
sodium concentration based on pre-intervention plasma sodium
concentration, total body water and other factors including the type and
amount of administered fluid, urine output and urinary electrolytes.17,18
natremia-associated morbidity. Young patients
seem to be affected to a greater degree than
older patients, possibly because of the absence of
age-related brain cell atrophy and the resulting
higher intracellular brain volume. If acute hypo-natremia develops, a larger intracellular brain
EMB = (Na+ + K+)input–output = mass balance of Na+ + K+ in a chosen duration of time.
volume could result in a greater increase in cell
= [E]IVF × VIVF + [E]oral × Voral + [E]tube feed × Vtube feed + [E]TPN × VTPN
volume within the confined space of the skull.
− [E]urine × Vurine − [E]GI × VGI − [E]sweat × Vsweat
DISCUSSION OF TREATMENT OPTIONS
VMB = Vinput – Voutput = mass balance of H2O in a chosen duration of time.
In edematous patients with otherwise asympto-
= VIVF + Voral + Vtube feed + VTPN + Voxidation − Vurine − VGI
matic hyponatremia, combined water restric-
tion and loop diuretics or vasopressin-receptor antagonists are appropriate treatment options.
y = 23.8 + (1.6/100)([G] − 120) where [G] = plasma glucose concentration.
In patients with acute or symptomatic hypo-
In patients with euglycemia, y1 = y2 = 23.8 for the sake of simplification.
natremia, however, the administration of a loop
, [Na+ + K+] in the administered total parenteral nutrition; [Na+]
diuretic plus intravenous saline is often neces-
, post-intervention plasma sodium concentration;
sary to achieve a higher rate of correction of the
water produced as a result of oxidation; V
Table 2 outlines two nonfatal cases of hypo-
natremia in premenopausal women who had signs and symptoms similar to those of our patient but had favorable outcomes. These
to proceed with hypertonic fluid treatment was
patients were treated primarily with hypertonic
reached after the team reviewed relevant litera-
saline or with the diuretic furosemide, and their
ture.10 In the setting of non cardiogenic pulmo-
symptoms resolved within 48 h. The decision to
nary edema and cerebral edema, treatment
administer hypertonic saline (plus furosemide
of the hyponatremia should be aimed at both
therapy) to patients with pulmonary and cerebral
correcting dysnatremia and achieving negative
edema is counterintuitive and might be ques-
tioned by many physicians. Indeed, in the case
In the fatal case presented here, the patient’s
presented here, the recommendation of hyper-
tonic fluid made by the consulting nephrolo-
gist was questioned by the emergency room
after administra tion of intravenous fluids. The
physicians and by the intensivist. Agreement
relative contributions of isotonic saline and
MAY 2006 VOL 2 NO 5 KALANTAR-ZADEH ET AL.
2006 Nature Publishing Group GLOSSARY
hypertonic saline to correction of this patient’s
References NGUYEN-KURTZ
hyponatremia can be determined quantitatively
1 Ayus JC and Arieff AI (1995) Pulmonary complications
of hyponatremic encephalopathy: noncardiogenic
EQUATION
pulmonary edema and hypercapnic respiratory failure.
An equation for predicting changes in plasma sodium
(Box 2).15 Administration of 6.8 l of isotonic
Chest107: 517–521
saline is predicted to have raised plasma [Na+]
2 Ayus JC and Arieff AI (1999) Chronic hyponatremic
by 3.6 mmol/l, whereas infusion of 0.245 l hyper-
association of therapies with morbidity and mortality.
tonic saline is predicted to have increased plasma
JAMA281: 2299–2304 Acknowledgments
[Na+] by 3.4 mmol/l. For a given urinary output,
et al. (2002) The health effects of ecstasy:
a literature review. Drug Alcohol Rev21: 53–63
the volume of isotonic saline required to raise
4 Cherney DZ et al. (2002) Acute hyponatraemia and
the plasma [Na+] to a target value will be signifi-
‘ecstasy’: insights from a quantitative and integrative
cantly greater than that of hypertonic saline. In
analysis. QJM95: 475–483 et al. (2004) Polydipsia as another
the setting of hyponatremia asso ciated with cere-
mechanism of hyponatremia after ‘ecstasy’ (3,4
bral and pulmonary edema, this additional fluid
methyldioxymethamphetamine) ingestion. Eur J
will worsen volume overload, as was the case
Emerg Med11: 302–304
Rosenthal Foundation, and the Fredrika Taubitz Fund.
with this patient. Administration of hypertonic
et al. (2002) Action of MDMA (ecstasy) and
its metabolites on arginine vasopressin release. Ann
saline and furosemide is therefore preferable to
NY Acad Sci965: 399–409 Competing interests
infusion of isotonic saline and furosemide, as
7 Haldane JS and Priestley JG (1916) The regulation of
The authors declared they have no competing
the former approach facilitates attainment of
excretion of water by the kidneys. J Physiol London 50: 296–303
negative water balance by limiting the amount
of infusate needed to increase the plasma [Na+]
amphetamine (“Ecstasy”) abuse. Am J Med Sci326: 89–93 et al. (2002) Hyponatraemic states
CONCLUSIONS
following 3,4-methylenedioxymethamphetamine
Nephrologists are often consulted on the manage-
(MDMA, ‘ecstasy’) ingestion. QJM95: 431–437
10 Balmelli C et al. (2001) Fatal brain edema after
ment of patients with MDMA-associated hypo-
ingestion of ecstasy and benzylpiperazine. Dtsch Med
natremia. At the dawn of the 21st century, however,
Wochenschr126: 809–811
many nephrologists, as well as emergency room
11 Parr MJ et al. (1997) Hyponatraemia and death after
“ecstasy” ingestion. Med J Aust166: 136–137
physicians, cardiologists and intensivists, might
12 O’Connor A et al. (1999) Death from hyponatraemia-
still be unaware of the potentially fatal outcome
induced cerebral oedema associated with MDMA
and might not feel comfortable recommending
(“Ecstasy”) use. NZ Med J112: 255–256
13 Ayus JC et al. (2000) Hyponatremia, cerebral edema,
administration of hypertonic saline in the pres-
and noncardiogenic pulmonary edema in marathon
ence of noncardiogenic pulmonary edema. This
runners. Ann Intern Med 132: 711–714
counterintuitive measure could, however, save
14 Arieff AI and Ayus JC (1993) Endometrial ablation
complicated by fatal hyponatremic encephalopathy.
lives, as recently indicated.13 Early symptoms
JAMA270: 1230–1232
of hyponatremic encephalopathy (e.g. nausea,
15 Arieff AI et al. (1995) Age, gender, and vasopressin
abdominal pain, headache and mild obtunda-
affect survival and brain adaptation in rats with metabolic encephalopathy. Am J Physiol268:
tion) and signs and symptoms of noncardiogenic
pulmonary edema (e.g. dyspnea, hypoxemia and
16 Ayus JC et al. (1992) Postoperative hyponatremic
pulmonary congestion or edema) in a young
encephalopathy in menstruant women. Ann Intern
woman with mild to moderate hyponatremia,
Med 117: 891–897
17 Kurtz I and Nguyen MK (2003) A simple quantitative
should prompt immediate hospitalization (prefer-
approach to analyzing the generation of the
ably in the intensive care unit) and administra-
dysnatremias. Clin Exp Nephrol7: 138–143
tion of hypertonic, rather than isotonic, saline in
18 Nguyen MK and Kurtz I (2004) New insights into the
pathophysiology of the dysnatremias: a quantitative
analysis. Am J Physiol Renal Physiol287: F172–F180
KALANTAR-ZADEH ET AL. MAY 2006 VOL 2 NO 5
2006 Nature Publishing Group
MEETING HELD ON REGULATORY MANAGEMENT THURSDAY 14 FEBRUARY 2008 COMMITTEE MINUTES of an ordinary meeting of the Regulatory Management Committee, held in the Council Chambers, 175 Rimu Road, Paraparaumu, on Thursday 14 February 2008 commencing at 9.00 am. PRESENT: Cr (Chair, Paraparaumu/Raumati Community Board) The Chair welcomed the members of the Committee, Community Board Chai
TRAUMATIC BRAIN INJURY DEFINITION: Traumatic brain injury (TBI) is injury caused to the head that results in minor to serious brain injury. It is caused by either an open head injury where there is a penetrating lesion or closed head injury (most common) where there is no outward injury. Characterized by permanent brain damage caused by concussion, contusion, or hemorrhages. Studen
 DISCUSSION OF DIAGNOSIS
DISCUSSION OF DIAGNOSIS