Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
The effect of fluid intake on renal length measurement in adults
The Effect of Fluid Intake on Renal LengthMeasurement in Adults
Fatih Kantarci, MD,1 Ismail Mihmanli, MD,1 Ibrahim Adaletli, MD,1 Harun Ozer, MD,1Fatih Gulsen, MD,1 Alev Kadioglu, MD,2 Ayca Altug, MD,1 Omer Uysal, MSc3
1 Department of Radiology, Istanbul University, Cerrahpasa Medical Faculty, 34300 Istanbul, Turkey2 ALKA Medical Imaging Center, Istanbul, Turkey3 Department of Biostatistics, Istanbul University, Cerrahpasa Medical Faculty, 34300 Istanbul, Turkey
Received 24 May 2005; accepted 3 November 2005
ABSTRACT: Purpose. To evaluate whether oral fluidintake has an effect on renal length as determined
Unilateral or bilateral reduction or increase in
kidney size is an important sign of many re-
nal diseases. Thus, knowledge of normal sono-
Methods. We studied 524 adult patients who were re-
graphic size is important when evaluating patients
ferred to our ultrasound unit with complaints other than
with renal diseases. Estimation of renal size via
urinary tract symptoms. The mean age of the patientswas 44 years (range 17–76). All of the measurements
sonography can be performed by measuring renal
were performed with the patient in the prone position.
length, renal volume, or cortical volume or thick-
The renal length of each kidney was measured by the
ness.1–5 Renal length and cortical thickness are
same observer before and after oral fluid intake. Stu-
routine measurements in the diagnosis and
dent’s t-test was applied for the statistical significance
follow-up of most disease conditions involving the
of renal length measurements before and after hydra-
tion. Analysis of variance was performed for the effect
In most institutions, sonographic evaluation of
of age and sex on the renal length measurements.
the genitourinary tract includes examination of
Results. The mean renal length on the right side
the kidneys, ureter (if possible), and urinary blad-
was 106.2 6 5.5 mm and 107.5 6 5.7 mm on the left
der. Therefore, measurements regarding the kid-
side before hydration. There was no statistically sig-
neys, such as renal length, can be performed in a
nificant difference between right and left side renallength measurements. After hydration, the mean re-
hydrated or nonhydrated state. Adequate hydra-
nal length was 113.5 6 6.1 mm on the right side and
tion may be provided intravenously or via oral fluid
114.6 6 6.6 mm on the left side. The mean increase in
intake,10,11 and is used primarily for accurate sono-
renal length after hydration was statistically signifi-
graphic evaluation of the bladder. The diagnosis of
cant (P < 0.001) and was 6.8% on the right side and
various disease conditions of the urinary tract—
6.6% on the left side. Sex and age did not affect the
such as obstruction or differentiation between a
parapelvic cyst and hydronephrosis—requires ad-
Conclusions. Oral fluid intake causes a statistically
equate hydration.10–12 The effects of hydration on
significant increase in renal length. This observation
the renal pelvis have been widely studied10,12–14;
should be taken into consideration when renal length
however, the effect on renal length by means of so-
measurements are clinicallly important. V
Periodicals, Inc. J Clin Ultrasound 34:128–133, 2006;
nography has not been established. The aim of our
Published online in Wiley InterScience (www.inter-
study was to evaluate whether oral fluid intake
science.wiley.com). DOI: 10.1002/jcu.20225
has an effect on renal length measurement.
Keywords: ultrasonography; kidneys; hydration; renallength; measurement
From October 2003 to September 2005, we pro-spectively measured kidney size in adult patients
who were attending our ultrasound unit for rea-
sons other than renal examinations. The inclu-
JOURNAL OF CLINICAL ULTRASOUND—DOI 10.1002/jcu
sion criterion for the study was normal appear-
amination), the patients were asked to empty their
ance of the kidneys on sonographic examination.
bladder just before the sonographic examination.
Exclusion criteria were chronic renal failure, hyper-
For the second part, the patients were subdivided
tension, diabetes mellitus, chronic heart failure,
into 2 groups. Group 1 patients (n ¼ 50) consumed
history of hemodialysis or peritoneal dialysis, uni-
1.5 l of water within 1 hour, while group 2 patients
lateral or partial nephrectomy, renal transplanta-
(n ¼ 50) remained dehydrated. The second exami-
tion, any congenital anomaly in 1 or both of the
nation for group 1 patients (hydrated group) was
kidneys, presence of a unilateral kidney, hydro-
performed when the patient noted bladder filling
nephrosis, renal cysts and/or neoplasms, renal cal-
but no urgency. The second examination for group
culi, and abnormal parenchymal echo appearance
2 patients (dehydrated group) was performed ap-
on initial examination. Written informed consent
proximately 1.5 to 3 hours after the baseline exam-
was obtained from all patients. The study was per-
ination. The timing was determined by an assist-
formed according to the guidelines of the Helsinki
ant who was blinded to the renal length measure-
ments but not the hydration status. The physician
The study included 524 patients (group A, 291
who performed the examination was blinded to
male, 233 female) in which the examiner was not
both the hydration status of the patients and the
blinded to the hydration status or the renal
renal length measurements. Measurements were
length measurements. The mean age of the patients
noted by an assistant who was also blinded to the
was 44 6 12.3 years (range 17–76). An additional
100 patients (group B, 52 male, 48 female) were
SPSS software for Windows (version 7.5; SPSS
studied in which the examiner was both blinded to
Inc., Chicago, IL) was used for statistical analy-
the hydration status and the renal length mea-
sis. The patients in group A were subgrouped
surements. The mean age of these patients was
based on side (right and left), gender (male and
female), or age differences. Grouping based on
The examination was performed in a quite,
age was made according to decades. Patients in
temperature-controlled room (228C) between 9
subgroup 1 were less than 30 years old, subgroup
and 12 A.M. Real-time gray-scale sonography was
2 between 30 and 39 years, subgroup 3 between
performed with a 2–5-MHz convex transducer
40 and 49 years, subgroup 4 between 50 and
connected to a Sonoline Elegra scanner (Siemens
59 years, subgroup 5 between 60 and 69 years,
Medical Solutions, Issaquah, WA). All the exami-
and subgroup 6 older than 69 years. Statistical
nations were performed by a single experienced
analysis included the overall comparison of the
radiologist. Renal length measurements were
renal length measurements on each side (right and
performed for each kidney while patients were in
left) before and after hydration via paired-sample
the prone position. All measurements were per-
t-test. The comparison between gender groups and
formed in deep inspiration. Both renal poles were
age groups was performed via independent-sample
identified and the measurements were performed.
t-test. The changes among gender groups, side-to-
At least 3 consecutive measurements were taken
side differences, and age groups between pre-
in the prone position for each kidney, and the
hydration and posthydration measurements were
mean of these measurements was calculated foreach kidney.
Patients in group A were all hydrated, and the
examinations were performed before and afterhydration. All patients fasted the night beforethe examination and oral fluid intake was re-stricted for a minimum of 6 hours before the ex-amination. For the first part of the study (base-line examination), the patients were asked toempty their bladder just before the sonographicexamination. For the second part, the patientsingested 1.5 l of water within 1 hour. The secondpart of the examination was performed when thepatients noted bladder filling but no urgency.
All patients in group B fasted the night before
the examination, and oral fluid intake was re-stricted for a minimum of 6 hours before the exam-ination. For the first part of the study (baseline ex-
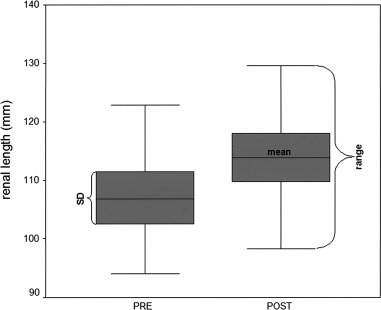
FIGURE 1. Change in renal length (mm) before and after hydration.
VOL. 34, NO. 3, MARCH/APRIL 2006—DOI 10.1002/jcu
FIGURE 2. Difference in millimeters between the prehydration and posthydration renal length measurements.
Mean Renal Length Measurements among Male and Female Subjects Before and After Hydration and the Percent
studied via analysis of variance. The patients in
were statistically significant (P < 0.001) (Fig-
group B were assessed via paired-sample t-test for
ures 1, 2). The renal length measurements were
comparison of the baseline renal length measure-
not statistically significant before or after hydra-
ments on each side (right and left) with the second
tion among males and females or among different
measurements for group 1 and group 2 patients.
age groups (Tables 1, 2). Analysis of variance
The amount of change (percent) was calculated for
revealed no significant effect of age, side, or gen-
both group 1 and group 2. A P value of less than
der on renal length measurements (P > 0.05).
0.05 was considered statistically significant.
In group B, the mean renal length at baseline
examination was 101.7 6 7.5 mm (right side,range 90.5–118.9 mm) and 102.3 6 6.9 mm (left
side, range 91.2–119.7 mm) for the patients who
In group A, the mean renal length before hydra-
were hydrated (group 1), and 102.6 6 9.5 mm (right
tion was 106.3 6 5.6 mm on the right side and
side, range 90.4–119.2 mm) and 103.1 6 9.8 mm
107.5 6 5.8 mm on the left side. Before hydration,
(left side, range 90.1–121.1 mm) for patients who
there were no statistically significant differences
remained dehydrated (group 2). The mean renal
between the right and left side renal length
length after hydration was 107.4 6 8.1 mm (right
measurements (P > 0.05). After hydration, the
side, range 91.1–123.4 mm) and 108.2 6 7.2 mm
mean renal lengths were 113.5 6 6.1 mm and
(left side, range 95.1–122.8 mm) for patients in
114.6 6 6.6 mm on the right and left sides,
group 1. The second examination for group 2 re-
respectively. The mean increase in renal length
vealed a mean renal length of 102.8 6 9.7 mm
was 6.8% and 6.6% on the right and left sides,
(right side, range 90.6–120.6 mm) and 103.2 6
respectively. After hydration, the comparison
9.7 mm (left side, range 90–120.7 mm). The sta-
between the right and left renal length measure-
tistical analysis revealed a significant change in
ments was not statistically significant (P > 0.05).
group 1 (P < 0.001), while there was no statisti-
The renal length measurements before and after
cally significant change in group 2 (P ¼ 0.164 for
hydration on the right and left sides separately
right side, P ¼ 0.251 for left side). The mean re-
JOURNAL OF CLINICAL ULTRASOUND—DOI 10.1002/jcu
Mean Renal Length Measurements among Different Age Groups Before and After Hydration and the Percent Increase
nal length increased 5.6% (right side) and 5.8%
glomerular filtration rate (GFR) and increases the
(left side) in group 1. The change was 0.1% (right
natriuresis.17 Increase in natriuresis after oral
and left sides) increase for group 2.
fluid intake may manifest as mild or moderatehydronephrosis, a common observation duringroutine sonographic examination of the kidneys.17We cannot directly examine the histopathological
changes in the kidneys after fluid intake, and we
Sonographic evaluation of the kidney is generally
do not know what changes occur in the glomerulus
a part of the urinary tract examination, in which
and collecting tubules in this situation. On the
the kidneys, ureter, and bladder are evaluated.15
other hand, the gross morphological changes may
The kidneys may be well identified in a nonfast-
be studied with imaging modalities such as sono-
ing patient; however, fasting may be desired to
graphy, CT, or MRI.1–5,18 We hypothesized that
limit bowel gas.15 When the kidneys are part of
the increased amount of urine production caused
a full urinary tract examination (ie, kidneys,
by oral fluid intake probably distended the col-
ureter, and bladder), high fluid intake is com-
lecting ducts, and this in turn may manifest as
monly used to accelerate urine production.10 The
an increase in the dimension of the kidneys.
examination is performed by filling the bladder
The position of the patient is probably one of
with a moderate amount of urine. Therefore, it is
the most important aspects of sonographic exami-
essential to know the effects of fluid intake on re-
nation of the kidneys. The kidneys are ovoid on
nal physiology and the morphological changes
cross-section, with the largest dimension proceed-
associated with it. The hydration status of the
ing anteromedially to posteromedially. Therefore,
patients by way of oral fluid intake varies from
longitudinal views of the kidney will demonstrate
patient to patient. Assessing the hydration status
a different shape depending on how the view was
is a complex issue and can be accomplished by
obtained.19,20 For this reason, we examined patients
measuring body weight, hemoglobin and hemato-
in the prone position. A posterior approach allows
crit levels, serum osmolality, sodium concentra-
the transducer to be closer to the kidneys, and the
tion, and urine-specific gravity and osmolality and
measurement technique is more standardized.
via bioelectrical impedence analysis.16 In our study,
There is little information available regarding
although the patients consumed 1.5 l of water, a
the accuracy of sonography in the evaluation of re-
standardized hydration status was not achieved
nal size.21 Renal volume measurements calculated
and should be noted as a limitation of the study.
with the ellipsoid formula applied to sonographic
Therefore, we attributed changes in renal length
images can result in a considerable systematic un-
on sonographic examination to changes in fluid
derestimation of renal volume and have large intra-
intake and excretion on the part of the patient.
observer and interobserver variations.1,5 On the
Although the renal effects of hydration are not
other hand, it has been suggested that renal length
well defined, it is said that hydration lowers the
measurements are more reliable than volume
VOL. 34, NO. 3, MARCH/APRIL 2006—DOI 10.1002/jcu
measurements. Ablett et al22 studied interobserver
In conclusion, it is essential to understand that
and intraobserver variations in renal length mea-
renal length measurements may change after
surements and found that the magnitude of varia-
oral fluid intake. This fact should be kept in mind
tion is similar whether the left or right kidney is
for disease processes in which renal length meas-
measured and whether measurements are made
urements are clinically important and are used
by 1 or multiple sonographers. They reported that
the SDs ranged between 4.8 and 7.2 mm. Ema-mian et al1 found a relative SD of 4%–5% for renallength in adults. In our study, in which the exam-
iner was blinded to both the hydration status and
1. Emamian SA, Nielsen MB, Pedersen JF. Intra-
renal length measurements, no statistically signif-
observer and interobserver variations in sono-
icant change in renal length measurements were
graphic measurements of kidney size in adult vol-
found in patients who were not hydrated. On the
unteers. A comparsion of linear measurements and
other hand, an approximately 6% increase was
volumetric estimates. Acta Radiol 1995;36:399.
seen in patients who were hydrated in the blinded
2. Brandt TD, Neiman HL, Dragowski MJ, et al.
study group. In the nonblinded group in which all
Ultrasound assessment of normal renal dimen-
the patients were hydrated, the change was ap-
proximately 7%. However, in the studies by Ablett
3. Spiegl G, Jeanty P, Kittel F, et al. Ultrasonic mea-
et al22 and Emamian et al,1 the hydration status
sure of the normal kidney. J Belge Radiol 1982;
of the patients was not standardized. The great
4. Emamian SA, Nielsen MB, Pedersen JF, et al.
interobserver and intraobserver difference may
Kidney dimensions at sonography: corrrelation
be due to the hydration status of the patients.
with age, sex, and habitus in 665 adult volunteers.
For practical reasons, it was not possible at the
beginning of our study to create a blinded study
5. Bakker J, Olree M, Kaatee R, et al. Renal volume
design. Therefore, we conducted a satellite-
measurements: accuracy and repeatability of US
blinded study design in a new but smaller group
compared with that of MR imaging. Radiology
of patients due to the significant bias introduced
by a nonblinded study. Our results in the blinded
6. Banholzer P, Haslbeck M, Edelmann E, et al. Sono-
study group confirmed the change in renal
graphic changes in the size of the kidneys in type I
length measurements (6% for the blinded group,
diabetes as a method of early detection of diabeticnephropathy. Ultraschall Med 1988;9:255.
7% for the nonblinded group), which was pro-
7. Sustic A, Mavric Z, Fuckar Z, et al. Kidney length
bably caused by the hydration of the patients.
in postoperative acute renal failure. J Clin Ultra-
A reduction in renal length is considered an in-
dicator of chronic renal disease, with a value of
8. McRae CU, Shannon FT, Utley WLF. Effect on re-
9 cm or less indicating irreversible disease.23 It
nal growth of reimplantation of refluxing ureters.
may also be used in follow-up for the progression
of a disease process affecting the kidneys; there-
9. Troell S, Berg U, Johansson B, et al. Ultrasono-
fore, accurate renal length measurements are
graphic renal parenchymal volume related to kid-
important.6–9 In our study, we found an approxi-
ney function and renal parenchymal area in chil-
mately 7% increase in renal length measurements
dren with recurrent urinary tract infections andasymptomatic bacteriuria. Acta Radiol 1984;25:411.
after oral fluid intake. Based on our results, one
10. Morin ME, Baker DA. The influence of hydration
may estimate that renal length measurements are
and bladder distension on the sonographic diagnosis
prone to variability depending on the fluid intake
of hydronephrosis. J Clin Ultrasound 1979;7:192.
of the patient. An important aspect of renal sono-
11. Shokeir AA, Provoost AP, el-Azab M, et al. Renal
graphic examination is sequential imaging change
Doppler ultrasound in children with normal upper
in which the enlargement or reduction of the kidney
urinary tracts: effect of fasting, hydration with
is associated with a disease pattern. We believe
normal saline, and furosemide administration.
that in such a situation, the patients are their
own control with the awareness that the same
12. Nicolau C, Vilana R, Del Amo M, et al. Accuracy of
level of fluid intake should be present when se-
sonography with a hydration test in differentiatingbetween excretory renal obstruction and renal
quential sonograms are obtained. Our study in-
sinus cysts. J Clin Ultrasound 2002;30:532.
cluded patients without renal complaints and
13. Hasch E. Changes in renal pelvic size in children
sonographically normal kidneys; however, the
after fluid intake demonstrated by ultrasound.
effect of hydration on renal length in abnormal or
diseased kidneys is not known. This issue should
14. Meola M, Giuliano G, Morelli E, et al. Ultrasound
diagnosis of suspected urinary tract obstruction
JOURNAL OF CLINICAL ULTRASOUND—DOI 10.1002/jcu
using a stimulated diuresis test. Nephron 1995;
19. Middleton WD, Kurtz AB, Hertzberg BS. Kidney.
In: Ultarsound: the prerequisites. 2nd edition.
15. Thurston W, Wilson SR. The urinary tract. In:
Rumack CM, Wilson SR, Charboneau JW, editors.
20. Michel SC, Forster I, Seiferet B, et al. Renal dimen-
Diagnostic ultrasound. 2nd edition. St. Louis: Mosby;
sions measured by ultrasonography in children:
variations as a function of the imaging plane and
16. Kavouras SA. Assessing hydration status. Curr
patient position. Eur Radiol 2004;14:1508.
Opin Clin Nutr Metab Care 2002;5:519.
21. Hricak H, Lieto RP. Sonographic determination of
17. Anastasio P, Cirillo M, Spitali L, et al. Level of
renal volume. Radiology 1983;148:311.
hydration and renal function in healthy humans.
22. Ablett MJ, Coulthard A, Lee RE, et al. How reli-
able are ultrasound measurements of renal length
18. Tublin ME, Tessler FN, McCauley TR, et al. Effect
in adults? Br J Radiol 1995;68:1087.
of hydration status on renal medulla attenuation
23. Rodriquez-de-Velasquez A, Yoder IC, Velasquez P,
on unenhanced CT scans. AJR Am J Roentgenol
et al. Imaging the effects of diabetes on the genito-
urinary system. Radiographics 1995;15:1051.
VOL. 34, NO. 3, MARCH/APRIL 2006—DOI 10.1002/jcu
Top 50 Tips for Navigating Bologna: Travel, travel, travel. Travel as much as possible. You will ALWAYS feel too busy and too stressed to leave town. but if you don't do it, you'll look back on the year and realize that your grades would not have slipped even if you'd gone somewhere. .more specifically, travel within Italy. There are a lot of really great small towns just a train
BLAZE TECHNOLOGY PTE LTD Features • Measures UV intensity up to 20W/cm2 (Standard Range) • Totally self-contained, battery-powered Applications • Monitor UV spot curing system performance • Measure individual UV lamp performance • Determine proper UV intensity required for curing any Operation Introduction The portable, EIT SpotCure is simple to use. Its
 sion criterion for the study was normal appear-
amination), the patients were asked to empty their
ance of the kidneys on sonographic examination.
sion criterion for the study was normal appear-
amination), the patients were asked to empty their
ance of the kidneys on sonographic examination.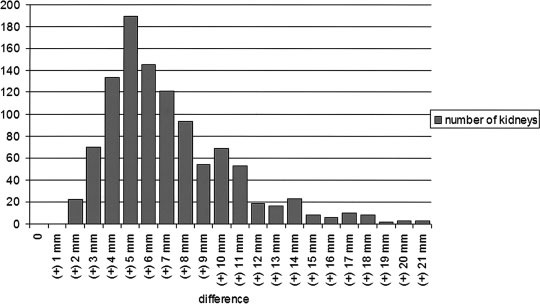 FIGURE 2. Difference in millimeters between the prehydration and posthydration renal length measurements.
FIGURE 2. Difference in millimeters between the prehydration and posthydration renal length measurements.