Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Microsoft word - patient information - english2007.doc
Bone & Joint Center, P.C./ACES PATIENT INFORMATION QUESTIONNAIRE Name: _______________________________________________________________________________ Address: _____________________________________________________________________________ Street address City State Zip code Height: ____feet ____inches Please check one: I am right-handed or I am left-handed What kind of work do you do? (Please check one)
Construction Desk job Driver Teacher Executive/Professional Factory Homemaker Retired Sales Student Other _____________________________
If you are not working now, when did you last work? ____/____/____ Does/did it require lifting? Yes No How often? Rarely Frequently Constantly How much? 10 Lbs. or less 10-50 Lbs. 50-100 Lbs. More than 100 Lbs. As part of your work, do you commonly? (Please check all those that apply)
Squat Push Pull Lift overhead Climb ladders/stairs Reach Bend Stoop
Is this a Workman’s Compensation case? Yes No Company name: ______________________________________ Tel: ( ) ________________________ Company address: _____________________________________________________________________ Street City State Zip code Is this a legal or third person liability case? Yes No Lawyer’s name: ______________________________________ Tel: ( ) ________________________ Lawyer’s address: _____________________________________________________________________ Street City State Zip code Which joint (s) are you having trouble with? (Please check all those that apply) Right side: Shoulder Elbow Wrist Hand Fingers Hip Knee Ankle Foot Toes Left side: Shoulder Elbow Wrist Hand Fingers Hip Knee Ankle Foot Toes
Back Neck Other (please specify) __________________________________________________
Please circle your one major complaint and please check any other complaints.
Difficulty with: Lifting Putting on clothes/shoes Climbing/descending stairs
Please list any other complaints: __________________________________________________________ Onset of the problem: Suddenly without known injury on ____/____/____ ____ Days ago ____ Weeks ago ____ Months ago ____ Years ago Gradually since ____/____/____ I do not know when it started An injury on ____/____/____ At work Other (specify location) _______________________ ____ Days ago ____ Weeks ago ____ Months ago ____ Years ago Overall, since it started, is your problem getting worse or Staying the same? Have you missed work or practice because of your injury? Yes No Injured while: (Please check all those that apply)
Other (please specify): __________________________________________________________
Injured during: (Please check all those that apply)
Other (please specify): __________________________________________________________
If this injury was on the job, please fill out this section.
Was any equipment, machinery, and/or object involved in the accident? Yes No
If yes, please explain: _______________________________________________________
_________________________________________________________________________
Was the accident reported to your supervisor and/or employer at the time of the injury? Yes No If this was a motor vehicle accident, please fill out this section.
Were you (please check)? Driver Passenger Pedestrian
Were you wearing a seatbelt? Yes No Did you strike your head or lose consciousness? Yes No If you were a passenger, what was your position in the vehicle? _____________________ What kind of vehicle (s) was/were involved in the accident (Please circle your type of vehicle and check off the other) Truck Van Car Motorcycle Other: ____________________
Type of collision: Rear-ended Head-on T-type Sideswipe Struck on the left
Struck on the right Multiple vehicles “Daisy chain” Other: ___________________________________________________
Was your vehicle moving when it was struck? Yes No How fast was it going? _____mph. Did your vehicle strike another vehicle or object? Yes No Describe: __________________________ _____________________________________________________________________________________ Was the accident reported to the police? Yes No Were traffic tickets issued? Yes No If yes, who received the tickets?__________________________ How was the weather? __________________________________________________________________ Other: _______________________________________________________________________________ _____________________________________________________________________________________ If you are experiencing PAIN, please answer this section. If not, please circle NO PAIN and skip to the next page. Location of the pain: (Please check all those that apply)
The pain goes to: (Please check all those that apply)
Where did your pain start? _______________________________________________________________ Where did your pain spread to? (if anywhere) ________________________________________________ Do you have any abnormal sensation? (Please check all those that apply)
________________________________________________________________________
Do you have weakness in the arms or legs? Yes No Where? ______________________________________________________________________________
Do you have any problems controlling your bowels or bladder? Yes No Frequency of pain: (Please check all those that apply)
_________________________________________________________________________
Time of day when the pain occurs? (Please check all those that apply)
Other: _______________________________________________________________________
The pain is:
_________________________________________________________________________
Do you have stiffness in the back/neck? (Please check all those that apply)
_________________________________________________________________________
Have you had back or neck pain before?
Yes No When? _______________________________
What is the MAXIMUM amount of time you could sit in one place?
Less than 15 minutes 15-30 minutes 30-60 minutes 1-2 hours Unlimited
What is the MAXIMUMamount of time you could stand in one place?
Less than 15 minutes 15-30 minutes 30-60 minutes 1-2 hours Unlimited
What is the MAXIMUM distance you could walk?
Which of the following aids for walking are you currently using?
No aids necessary Brace Cane Crutches Walker Wheelchair
Could you go as far if you couldn’t use an aid such as a cane or crutches? Yes No What is the MAXIMUM number of stairs that you can climb?
None A few steps ½ Flight 1 Flight 2 or more flights
PLEASE CIRCLE THE NUMBER THAT CORRELATES BEST WITH HOW FAR YOU ARE FROM NORMAL TOWARD THE WORST POSSIBLE SITUATION YOU CAN IMAGINE OR HAVE SUFFERED. 0 = No pain or limitation at all.
10 = The worst possible pain or limitation that you could imagine
How bad is the pain at the worst it’s ever been?
How bad is the pain at the best it’s ever been?
Does the pain interfere with your lifestyle?
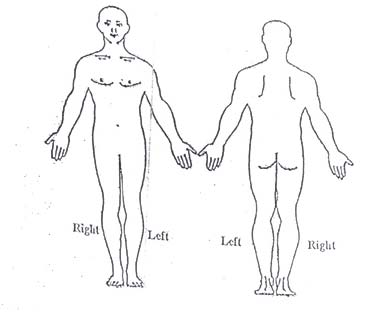
Where is your pain? (Please mark on the drawings where you feel the specific type of pain or sensation) Use the following symbols to indicate your specific type of pain or sensation: Burning: XXXX Throbbing: ++++ Sharp: //// Aching: •••• Numbness: **** What activities or positions make the pain worse? (Please check all those that apply)
Sitting (Driving, airplane, theater, etc.)
Carrying things (laundry, groceries, etc.)
_________________________________________________________________________
What activities or positions make the pain better? (Please check all those that apply)
_________________________________________________________________________
Have you taken any medication for the pain? Yes No (If so, please check all those that apply) Pain medications Anti-inflammatories Muscle relaxants
Does the medication help? Yes No Only a little bit Activities you CANNOTperform because of the injury? (Please check all those that apply)
Sitting (driving, airplane, theater, etc.)
Carrying things (groceries, laundry, etc.)
Continued
Other: ____________________________________________________________________________
I have had to quit some nonsporting recreational activities that I enjoy (Please list) __________________ _____________________________________________________________________________________ How often do you wake up at night or have difficulty going to sleep?
I can sleep but only when I take medicine
I can’t sleep even when I take medicine
Which sports do you (or would like to) participate in but are limited in them? __________________ _____________________________________________________________________________________ Have you or do you participate in competitive sports and at what level? _______________________ _____________________________________________________________________________________ Has your injury ever been treated by your family physician? Yes No Physician’s name: ________________________________When? _______________________________ Diagnosis: ______________________________________ Treatment? ___________________________ Has your injury ever been treated by an orthopedic or neurosurgeon? Yes No Physician’s name: ________________________________When? _______________________________ Diagnosis: ______________________________________ Treatment? ___________________________ Has your injury ever been treated by a chiropractor or naprapath? Yes No Physician’s name: ________________________________When? _______________________________ Diagnosis: ______________________________________ Treatment? ___________________________ Were you ever treated for your injury in an emergency room? Yes No Hospital: _______________________________________ When? _______________________________ Diagnosis: ______________________________________ Treatment? ___________________________ Have you ever been admitted to a hospital for your injury? Yes No Hospital: _______________________________________ When? _______________________________ Diagnosis: ______________________________________ Treatment? ___________________________
Have you ever had physical therapy (PT), a brace, or a corset? Yes No When: _________________________________________ Where? ______________________________ Results: _____________________________________________________________________________ Have you ever had x-rays of your injury taken? Yes No When: _________________________________________ Where? ______________________________ Results: _____________________________________________________________________________ Have you ever had a myelogram (dye test) done? Yes No When: _________________________________________ Where? ______________________________ Results: _____________________________________________________________________________ Have you ever had a CAT scan or an MRI of your injury done? Yes No When: _________________________________________ Where? ______________________________ Results: _____________________________________________________________________________ Have you ever had an EMG/NCVS (electromyelogram/nerve conduction velocity) done? Yes No When: _________________________________________ Where? ______________________________ Results: _________________________________________Ordering Doctor: ______________________ Have you ever had a chymopapain injection (meat tenderizer)? Yes No When: _________________________________________ Where? ______________________________ Results: _________________________________________Ordering Doctor: ______________________ Have you ever had spine surgery (laminectomy or spinal fusion) Yes No When: _________________________________________ Where? ______________________________ Results: _________________________________________Ordering Doctor: ______________________
THANK YOU FOR YOUR PATIENCE IN FILLING OUT THIS FORM!
HIGHLY INDUCIBLE TET-ON VECTOR SYSTEM Summary of the Offer developed. The original tetR do not contain Public Health System (SSPA) has developed a TetR(Tetracycline repressor)-based al -in-allow the design of a less-toxic Tet-inducible Description of the Offer expression cassette that maintain the endogenous characteristics of the regulated- Inducible gene expression systems b
Ref. CoP13 Prop. 37 Inclusion of Hoodia spp. in Appendix II, designating all parts and derivatives except those bearing the label ‘Produced from Hoodia spp. material obtained through controlled harvesting and production in collaboration with the CITES Management Authorities of Botswana, Namibia and South Africa under agreement no. BW/NA/ZA xxxx’ . Proponents: Botswana, Nami
 PLEASE CIRCLE THE NUMBER THAT CORRELATES BEST WITH HOW FAR YOU ARE
PLEASE CIRCLE THE NUMBER THAT CORRELATES BEST WITH HOW FAR YOU ARE