Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Bme.sjtu.edu.cn
NIH Public Access Author Manuscript Neurosurgery. Author manuscript; available in PMC 2009 June 1. Neurosurgery. 2008 June ; 62(6): 1340–1350. doi:10.1227/01.neu.0000333306.64683.b5. Evidence for Inflammatory Cell Involvement in Brain Arteriovenous Malformations Yongmei Chen, MD, PhD1, Wei Zhu, MD, PhD1, Andrew W. Bollen, MD, DVM5, Michael T. Lawton, MD2, Nicholas M. Barbaro, MD2, Christopher F. Dowd, MD1,2,4, Tomoki Hashimoto, MD1, Guo-Yuan Yang, MD, PhD1,2, and William L. Young, MD1,2,3 for the UCSF BAVM Study Project
1 Center for Cerebrovascular Research, Department of Anesthesia and Perioperative Care, University ofCalifornia, San Francisco, CA 94110
2 Department of Neurological Surgery, University of California, San Francisco, CA 94110
3 Department of Neurology, University of California, San Francisco, CA 94110
4 Department of Radiology, University of California, San Francisco, CA 94110
5 Department of Pathology, University of California, San Francisco, CA 94110Abstract Objective—Brain arteriovenous malformations (AVM) have high MMP-9, IL-6 and MPO expression, and polymorphic variations in inflammatory genes are associated with increased risk of hemorrhage. In this study, we characterized the presence of inflammatory cells in AVM lesional tissues. Methods—Immunohistochemistry was used to identify and localize neutrophils (MPO as marker), macrophages/microglia (CD68 as marker), T lymphocytes (CD3 as marker), and B lymphocytes (CD20 as marker). Endothelial cell (EC) marker CD31 was used as an index to assess vascular mass (EC mass). Surgical specimens from 20 unruptured, non-embolized AVMs were examined; seven cortical samples from temporal lobectomy were used as controls. Positive signals for inflammatory cell markers were counted and analyzed by normalizing to the area of the tissue section and the amount of endothelial cells (cells/mm2/EC mass pixels). Levels of MPO and MMP-9 were Results—Neutrophils and macrophages are all frequently identified in the vascular wall of AVM tissues. In contrast, T and B lymphocytes are rarely observed in AVM tissues. AVM tissues displayed more neutrophil and macrophage/microglia markers than epilepsy control tissues (MPO: 434 ± 333 vs 5 ± 4, P=0.0001; CD68: 454 ± 404 vs 4 ± 2, P=0.0001; cells/mm2/EC mass pixels). In ex vivo studies, neutrophil quantity, MPO, and MMP-9 levels were all co-linear(R2=0.98–0.99). Conclusion—Our study demonstrates that inflammatory cells are present in AVM tissues. Taken together with prior genetic and cytokine studies, these data are consistent with a novel view that inflammation is associated with AVM disease progression and rupture. Keywords
CD68; inflammation; myeloperoxidase; vascular malformations
Correspondence: William L. Young, M.D., University of California, San Francisco, Department of Anesthesia and Perioperative Care,1001 Potrero Avenue, Rm. 3C-38, San Francisco, CA 94110, Phone: 415-206-8906; Fax: 415-206-8907, Email: ccr@anesthesia.ucsf.edu. Background
Brain arteriovenous malformations (AVM) are complexes of tortuous, tangled vessels
representing fistulous connections between arteries and veins lacking a capillary bed (8,16). These vascular lesions are characterized by a phenotype of excessive angiogenesis and vascularremodeling. The primary clinical implication of AVM is recurrent spontaneous intracranialhemorrhage. The pathophysiology underlying brain AVM is not clearly understood and thereis a presumption, with only circumstantial evidence, that they are primarily congenital, staticlesions (47).
Our general hypothesis is that inflammation is involved in the clinical course of the diseasestate, if not the pathogenesis of the lesion. This view is based on several lines of evidence. Wepreviously found an association between promoter polymorphisms in inflammatory cytokinegenes and AVM intracranial hemorrhage (ICH) risk; TNF-α was associated with increased riskof new ICH in the natural course of AVMs (1), and IL-6 was associated with presenting ICH(37). We have also demonstrated that brain AVM tissues displayed increased inflammatorymarkers compared to control tissues by biochemical methods (6,7). There is a precedent in thatintracranial aneurysms, even if unruptured, have an inflammatory component to the phenotype(10,17).
In order to provide further evidence that inflammation and leukocyte participation is associated
with the phenotype of the disease, we present several lines of additional evidence. We examinedunruptured tissue specimens in patients that had not undergone pre-surgical embolization, twopotential confounders that might increase the level of inflammatory infiltrates in the lesionaltissue. We used immunocytochemistry to characterize leukocyte infiltrates. To further explainour previous observations (6,7), we demonstrate a linear relationship between leukocytequantity and MPO expression. Because intra- or extravascular blood may affect matrixmetallonproteinase 9 (MMP-9) expression (44), we also show that such contamination cannotexplain the large increases in MMP-9 levels we measured in lesional tissue. Materials and Methods
All studies involving patients were IRB-approved and patients gave informed consent. Procedures for the use of laboratory animals were approved by the UCSF Institutional AnimalCare and Use Committee. Subjects
Beginning in June 2000, patients with AVM evaluated at the University of California, San
Francisco (UCSF) were entered into an ongoing prospective registry (18). We analyzed a subsetof this group who underwent microsurgery and had tissue available for analysis. We selectedfrom our tissue bank cases that were unruptured and did not undergo pre-surgical embolization. Control cerebral cortex was obtained from patients undergoing surgical treatment of epilepsyas previously described (20,23). Samples were taken from structurally normal temporal loberemote from the epileptogenic focus. Prior to surgery, Decadron was given to both lobectomypatients and brain AVM patients in the same dose range. Immunohistochemistry
We used immunocytochemistry to characterize leukocyte infiltrates. CD31 antibody wasobtained from DakoCytomation (Denmark) and was used according to the company’sinstruction. This antibody primarily labels endothelial cells, and its specificity has beenreported.(36) MPO, CD68, CD3, and CD20 were purchased from Serotec (Raleigh, NC) andwere used according to the manufacture’s protocol. The specificities of these antibodies have
Neurosurgery. Author manuscript; available in PMC 2009 June 1.
been tested by the manufacture, and have also been reported. (3,4,25,26,29). Brain sections at10 μM were fixed with cold acetone for 20 min at 4°C. Endogenous peroxidase activity was
quenched by incubating slides in 0.3% H2O2 in methanol for 30 minutes. Slides were rinsedin 2 changes of PBS, pH 7.4, and then incubated in PBS with 0.1% Triton X-100 for 30 minutesat room temperature. After blocking, sections were incubated with primary antibodies dilutedin PBS with 0.1% Triton X-100 at the following concentrations: mouse monoclonal anti-human-MPO, 1:2000, mouse monoclonal anti-human-CD68, 1:1000, mouse anti-human CD3,1:200, mouse anti-human CD20, 1:100, and mouse anti-human CD31, 1:100. After incubatingat 4°C overnight and washing in PBS, the sections were incubated with biotinylated goat anti-mouse (Vector Laboratories, Burlingame, CA) diluted 1: 5000 for 1 hour at room temperature,and were treated with the ABC streptavidin detection system (Vector Laboratories) for 1 hourafter washing with PBS. The resulting horseradish peroxidase signal was detected using 3,3′-diaminobenzidene. For dual fluorescent staining, after incubating at 4°C overnight withprimary antibodies, sections were incubated with Alexa Fluor 594-conjugated goat anti-mouseor Alexa Fluor 488-conjugated goat anti-rabbit IgG (Molecular probes, Eugene, OR) at 1:500dilution for 1 hour at room temperature. They were then mounted and photographed withfluorescent microscope. Negative controls were performed by omitting the primary antibodiesduring the immunostaining. Assessing the amount of neutrophil and macrophage in AVM tissue
The area of each tissue section was measured with NIH image J program, and expressed asmm2. To quantitate the amount of leukocytes present in AVM tissue, neurophil positive signal(brown color associated with blue nuclei) present in the vascular lumen (defined asunassociated with endothelial cells), in the vascular wall (defined as associated with endothelialcells, or smooth muscle cells), and in the parachyma of AVM tissue was counted separately. Neutrophil positive signal was also counted in the control epilepsy tissue in the same manner. The number of positive signals was taken as neutrophil count. The count was divided by themeasured area to obtain neutrophil count per unit area. The neutrophil counts from the vascularwall and parenchyma were combined and analyzed because the neutrophils from these twolocations are presumably available to exert a substantial biological effect on tissue.
Because the control tissue had a different amount of vascular tissue than the AVM nidus, wenormalized the area to an index of blood vessel mass, which is represented by the amount ofendothelial cell (EC) marker CD31. Brain AVM tissue and epilepsy tissue were immunostainedwith CD31. The amount of CD31 was assessed by measuring CD31 digitized positive bloodvessels with NIH image J program by computer-aided planimetry. Staining images weredigitized under a 20× objective with a spot camera (Leica, Germany) equipped with NIH imageJ software. To control for the variations during photographing, all images used for cell counting
were acquired under the same magnification, light intensities, and exposure time on slides. Thethresholds were selected with a “set color threshold” feature in the Image J software, whichpermits the user to select pixel regions that were considered positive. After establishing thethreshold, this same parameter was applied to all images during counting. The tissue slides foreach cell marker were processed identically during staining to avoid impact of backgroundcolor on counting. The positive signal displayed dark brown color which is in sharp contrastto the background light brown color, and thus, the counting is not affected by the smallvariations in background color. The amount of CD31 was assessed by measuring the pixels ofCD31 positive particles, and was expressed as pixels. Neutrophil count per unit area per unitEC mass was calculated. The amounts of macrophage were assessed in the same fashion as forneutrophils. Neurosurgery. Author manuscript; available in PMC 2009 June 1. Isolation of neutrophil from peripheral blood of AVM patients
To further explain our previous observations that suggested the correlation between leukocyte
infiltration and inflammatory marker expression (6,7), we correlated leukocyte quantity andMPO expression ex vivo. Neutrophils were isolated from brain AVM patients’ blood by usingHistopaque 1077 (Sigma-Aldrich, St Louis, MO). The isolated cells were resuspended atdifferent density in PBS, and were used for assessing MMP-9 and MPO content by ELISA, asdescribed below. Enzyme-linked immunoadsorbent assays (ELISA)
MPO levels were measured by ELISA according to the protocols provided by the manufacturer(Calbiochem, San Diego, CA). Protein levels of MMP-9 in tissue specimens were measuredusing specific ELISA kits (R&D systems Inc., Minneapolis, MN) according to themanufacturer’s protocol. Animals and blood infusion
Because intra- or extravascular blood in AVM tissue may affect MMP-9 expression (44), wefurther investigated this effect by injecting whole blood in the mouse brain. Adult male, CD-1mice, weight 30 to 35 g, were purchased from Charles River Laboratory (Wilmington, MA). Mice (n= 3 per group) were injected with 20μl of whole blood at various dilations: 100% (no
dilution), 50%, 25% (diluted with normal saline). A control group was injected with normalsaline. The method for whole blood injection was as described by Tejima et al (44). Briefly,after induction of anesthesia with ketamine and xylazine (intraperitoneal), mice were placedin a stereotactic frame (David Kopf Instruments, Tujunga, CA). Hamilton syringe was insertedthrough a burr hole 1 mm lateral to the sagittal suture, 1 mm posterior to bregma, and 3 mmunder the cortex. 20 μl of injectate (whole blood, diluated whole blood, or normal saline asdescribed above) was injected stereotactically into the right caudate putamen. The mice weresacrificed at 3hr after treatment. Tissue sampling is depicted in Figure 8A. Brain tissues wereimmediately frozen in liquid nitrogen and stored at −80°C. For MMP-9 activity assessment,tissue homogenates were centrifuged at 10,000g for 20 min at 4°C, and the supernatants of thehomogenates were used for zymography. Gelatin zymography
Zymography was performed as previously described (24). Briefly, protein sample of 40 μgwas separated under non-reducing conditions in a 10% zymogram gel (Invitrogen, Carlsbad,CA) containing 0.1% gelatin as a substrate. Following electrophoresis, gels were washed, andincubated in developing buffer overnight at 37°C. Then the gels were stained with 0.5%Coomassie Blue R-250 and de-stained. MMP activity can be detected as white bands of lysis
against the Coomassie blue stained gel. Protein bands in zymography were quantified byscanning densitometry using KODAK image analysis software (Eastman Kodak Company). In preliminary experiments, controls with increasing amounts of protein verified thatquantitative band intensities fell within a linear range. Statistical analyses
Data are presented as mean ± SD. For neutrophil and macrophage counts and indices, wedetermined that the distribution of values was skewed and therefore used the non-parametricMann-Whitney test to compare AVM to control tissues. Linear regression was used to comparethe various assayed protein relationships. Results from animal and cell culture studies wereanalyzed using a one-way ANOVA followed by the Scheffé test. A probability value of lessthan 5% was considered to represent statistical significance. Neurosurgery. Author manuscript; available in PMC 2009 June 1.
Table 1 shows the demographic and brain AVM characteristics of the study cohort. The mean
age (years) for AVM patients was 46 ± 15 and 36 ± 13 for control patients (P=0.11). MeanAVM size was 2.2 ± 1.3 cm. Presence of inflammatory cells in AVM tissues
To investigate whether inflammatory leukocytes are present in brain AVM tissue, weperformed immunohistochemistry on sections from frozen AVM tissues using neutrophilmarker MPO, macrophage/microglia marker CD68, T lymphocyte marker CD3, and Blymphocyte marker CD20. We examined unruptured tissue specimens in AVM patients thathad not undergone pre-surgical embolization, two potential confounders that might increasethe level of inflammatory infiltrates in the lesional tissue. Neutrophils were present in thevascular wall as well as in parenchymal tissues of AVM, demonstrating regional infiltrationof neutrophils (Figure 1a, b, c, d,e,f). Although a majority of MPO signals were detected in thevascular wall and the parenchymal tissues, some of MPO signals were observed in the lumenof the vessel of AVM (brown color indicated by arrowheads) (Figure 1a). These are presumedto be neutrophils that remained in the vascular lumen during resection. There were no MPOpositive cells in epilepsy brain samples (Figure 1 g, h).
Macrophages, monocytes, and microglia, identified by CD68 staining, were scatteredthroughout the AVM tissue specimens such as vascular wall and parenchyma (brown colorindicated by arrows, Figure 2a, b, c, d, e and f). Figure 2a, c and e are representatives fromthree brain AVM patients, and g is from an epilepsy patient. Figure 2b, d, f and h arephotographed under higher power from areas from Figure 2a, c, e, g respectively (indicated byrectangle).
To determine whether neutrophil and macrophage were present in the same vascular loci, serialAVM sections (a and e; c and g) were stained with MPO and CD68 markers respectively. Asshown in Figure 3a and 3e, a majority of neutrophils and macrophages were present inproximity in the same vessels. However, in some cases, neutrophils and macrophages werepresent at different locations: neutrophils mainly at the inner wall, and macrophages mainly atthe outer vascular wall (Figure 3c and 3g).
To quantitatively assess leukocyte infilatration in brain AVM tissue, we performed cellcounting on slides immunostained with MPO, CD68, or CD31. Table 2 shows results of MPOand CD68 signal representing neutrophils and macrophage indices, respectively, in the vascularwall, lumen, and adjacent parenchyma tissue. As shown in Figure 4, brain AVM tissues had
more MPO and CD68 than the cortical tissues from epilepsy patients (MPO: 434 ± 333 vs 5 ±4, P=0.0001; CD68: 454 ± 404 vs 4 ± 2, P=0.0001; cells/mm2/EC mass pixels). In addition,the amount of neutrophils and macrophages in brain AVMs was not closely correlated (R2 =0.18, y = 0.515× + 230, n = 20, P = 0.06). We found no association between the amount ofneutrophil or macrophage and avm location, size, or drainage (data not shown).
In contrast to the abundant MPO and CD68 signals present in brain AVM tissues, the signalsfor T cells (CD3) and B cells (CD20) were rare in brain AVM tissues (data not shown). Correlation of neutrophils with MPO and MMP-9 levels
To determine whether neutrophils contribute to MMP-9 production in brain AVM tissue, weperformed double immunofluorescent staining of MPO and MMP-9 on AVM tissue sections. As represented in Figure 5, majority of MMP-9 signal (a, green) and MPO signal (b, red) inbrain AVM tissue co-localized (c, yellow), indicating that a major source of MMP-9 in AVMtissues was from neutrophils. Neurosurgery. Author manuscript; available in PMC 2009 June 1.
To validate the use of MPO as a marker for quantitative assessment of neutrophils, we measuredMPO and MMP levels in neutrophils isolated from patients with brain AVMs. There was a
linear relationship among neutrophil counts and MPO and MMP-9 levels (Figure 6A and 6B). Neutrophil count was linearly correlated with MPO and MMP-9 (R2=0.99, R2=0.98). MPOlevel, in turn, correlated with MMP-9 levels (Figure 6C, R2=0.99). The results indicate thatMPO level could be used as an index for assessing the amount of neutrophils, and imply thatmore neutrophils present in brain avm tissues could be associated with higher MPO and MMP-9levels. Contribution of the blood pool to tissue measurement of MMP-9
We have previously reported that brain AVM tissues displayed higher levels of inflammatorymarkers compared to control epilepsy tissues by ELISA (6). Brain AVM tissues dissected insurgery are heterogeneous, and contain varying amount of blood, both intravascular andextravascular. To assess the amount of blood present in AVM tissues, and the contribution ofblood source MMP-9 on measurements of total MMP-9 levels, we measured the amount ofhemoglobin in brain AVM tissues and used it as an index for the amount of blood and comparedit with MMP-9 tissue levels. MMP-9 level was correlated with Hb (Figure 7). However, theblood pool, as reflected by Hb content, contributed to only 6% of the variation in therelationship (R2 = 0.06, y = 0.048× + 9.79, n = 77, P = 0.04), suggesting that blood-borneMMP-9 only partially accounted for the amount of total measured MMP-9 activity in surgical
To further examine the potential confounding effects of retained blood cells in AVM tissueson MMP-9 tissue levels, we injected blood at varying hematocrits into the mouse brain andmeasured MMP-9 tissue levels. Figure 8A shows the site of blood infusion and tissue sampling. Blood injection increased MMP-9 level by 22% to 37% (100% blood 137 ± 11 vs 50% blood131 ± 1.3 vs 25% blood 122 ± 1.8 vs normal saline 100 ± 10). MMP-2 level increased in aparallel fashion as MMP-9 (Figure 8B and 8C). The results indicate that about 78% to 63%MMP-9 level came from parenchyma tissue, and suggest that even large amounts ofextravascular blood could not account for the large increases in MMP-9 level that we havepreviously described (6). Discussion
This study reports the first quantitative description of neutrophils and macrophages in the nidusof brain AVM tissue removed during microsurgical resection. We found that neutrophils andmacrophages were present in the vascular wall of brain AVM tissues, as well as adjacentparenchyma to a greater degree than control tissue. In contrast, we did not observe a significant
amount of T and B lymphocytes present in brain AVM tissues. Because prior hemorrhage orembolic material might confound interpretation of inflammatory infiltrates in the lesionaltissue, we examined leukocyte infiltrates in brain AVM tissue from unruptured and un-embolized patients. Our current findings are consistent with our prior reports which suggestthat inflammatory response is present in brain AVMs and plays a role in its pathophysiology. (6,7,20) Our gene microarray studies found that several genes involved in inflammation suchas chemokine receptor 1, TGF-β, angiopoitein 2, and integrin α are upregulated in brain AVMs. (20) In addition, our ELISA analysis showed that elevated concentrations of inflammatorybiomarkers in brain AVMs.(6,7) Consistent with our data, Shenkar et al reported that severalinflammatory genes such as NF-kB, IL-8 receptor, and TNF-related receptor were increasedin brain AVMs.(40) The novel finding of this study is the observation of inflammatoryleukocytes in un-ruptured, and non-embolized brain AVM patients. Neurosurgery. Author manuscript; available in PMC 2009 June 1. Inflammatory leukocytes are present in brain AVM tissues
Inflammation has been considered as shared pathological mechanisms in many vascular
disorders including aneurysm (10,21). Inflammatory leukocytes have been implicated aspathological mediators in cardiovascular disease and brain injury (14,30,42). Underphysiological conditions, leukocytes circulate freely and do not interact with the endothelialcells. During inflammatory cascades, leukocytes transmigrate to the cerebral microvasculature,and accumulate at the inflammatory site in response to cytokines, chemokines, as well asproducts of tissue breakdown. They secrete enzymes such as MPO, MMPs, and releasecytokines including IL-6 that contribute to brain injury (5,9,41).
Our immunohistochemical staining demonstrates that neutrophils and macrophages are presentin the vascular wall as well as adjacent tissue of brain AVMs. Our data are consistent with theview that inflammation may play a role in brain AVM pathophysiology. The rarity of T and Bcells in brain AVMs was somewhat surprising. However, their absence does not preclude aneffect of chronic inflammation: macrophages, neutrophils, as well as vascular endothelia aresufficient to produce and release inflammatory mediators.(38) A significant cellular componentof chronic inflammation associated with pathological angiogenesis is the macrophage.(2,11,32,33) We do not have definitive explanation or a precedent why pathways for T & Blymphocyte recruitment in brain AVMs are not as pronounced as those for macrophages andneutrophils. Further studies are needed to elucidate the precise stimulatory mechanisms for
macrophages and neutrophils recruitment.
Although dexamethasone was given to both lobectomy patients and brain AVM patients in thesame dose range, we cannot exclude the possibility that the drug may differentially impactAVM and temporal lobe differently, as the degree of inflammation in the control and brainAVM patients was clearly different and but there is a possibility that there is some differencein the dose response to diminishing the number cells. Because brain AVM tissues appear tohave a much higher inflammatory load, we would surmise that dexamethasone probably leadsto an underestimation of inflammation in AVM, and thus not affect our conclusions. Inflammatory cells could release various pro-inflammatory cytokines, MMPs, and otherproteolytic enzymes capable of weakening or destroying the vascular wall leading to vascularrupture and hemorrhage. MMP-9 is an effector as well as a regulator of leukocyte function. Itis stored in the tertiary granules of neutrophils, and is considered a specific marker of neutrophilmaturation (35). MMP-9 synthesis in leukocytes is stimulated by lipopolysaccaride andcytokines (12,15,39,45). Enhanced MMP-9 activity could lead to brain AVM hemorrhage. The amount of neutrophils correlates with MPO and MMP-9 levels
Myeloperoxidase (MPO) is a heme protein expressed at high levels in neutrophils (13,27,43),
and is a potent proinflammatory mediator (28,34). To validate the use of MPO as an index forquantitative assessment of neutrophils, we determined MPO and MMP levels in neutrophilsisolated from patients with brain AVMs. Our results demonstrate a linear relationship betweenneutrophil quantity and MPO expression. In addition, the amount of neutrophils has been foundto be tightly associated with the level of MMP-9. MMP-9 is a major component of neutrophilictertiary granules, and is released from neutrophils in inflammation in response to pro-inflammatory cytokines.(35,39,45) In our recent animal model studies, we have demonstratedthat neutrophil depletion lead to decreased MMP-9 activities.(19) In addition, it has beendemonstrated that neutrophils release neutrophil gelatinase-associated lipocalin (NGAL),which protects MMP-9 from degradation, thereby resulting in enhanced MMP-9 enzymaticactivity.(46) The data indicate that MPO level serves as a practical means of measuringneutrophil load. The data also imply that more neutrophils present in brain AVM tissues couldlead to higher MPO and MMP-9 levels. Neurosurgery. Author manuscript; available in PMC 2009 June 1. Contribution of the blood pool to tissue measurement of MMP-9
Because intra- or extravascular blood may affect MMP-9 expression (44), we assessed the
potential impact of blood pool-derived MMP-9 by correlating hemoglobin level with MMP-9level. The purpose of injecting blood into mice brain and measuring MMP-9 levels (datapresented in Figure 8) was to determine possible contribution of MMP-9 in blood, from eitherintra- and extravascular, on measurements of total MMP-9 levels. We measured MMP-9 levelsin mice brain tissues which contained injected blood. This was to mimic MMP-9 determinationin brain AVMs which contained a combination of AVM lesional tissue, intravascular blood,and extravascular blood. Since none of our cases in the present study presented withhemorrhage, the estimate of blood pool MMP-9 is a “worst-case” estimate.
In our previous study, we have reported that brain AVM samples had higher levels of MMP-9,TIMP-1, and TIMP-3. MMP-2 and TIMP-2 levels were below detection in brain AVMs.(22)MMP-9 has been implicated to play a critical role in vascular remodeling and rupture, thus wefocused on MMP-9 in this study. Our data indicate that MMP-9 derived from the blood poolcontributes only to a small degree to the otherwise large amount of total MMP-9 expressed inbrain AVM tissue amount, as determined by the ELISA method. This notion is supported byour animal study which showed that increasing dosage of blood only partially elevated MMP-9level. MMP-9 was determined at 3 hr after blood infusion. We chose this time point to mimicthe period for AVM tissue harvest at clinical settings. This is also the time period for neutrophil
in the blood to infiltrate and transmigrate to vascular wall (31). Infusion of whole blood intothe mouse brain increased MMP-9 level to 2.4 ng/mg compared to1.6 ng/mg with normal salineinjection. The mean MMP-9 level measured in brain AVM tissue was 28 ng/mg (6). Thesedata suggest that no more than 1/10 of total MMP-9 derives from the blood pool. We cannotdirectly translate from mouse to human tissue, but the result serves as an estimate of the orderof magnitude. Taken together, our results suggest that the influence of blood contamination,either by induction of astrocytic MMP or direct transfer, might be estimated to be in the rangeof 6% (by MMP-9 correlation with Hb in AVM tissue analysis) to 37% (by animal model usingblood injection), a range that is an order of magnitude lower than previous estimates of MMPand MPO expression in AVM compared to normal brain tissue (6). Conclusions and Limitations
The data presented here, when taken together with previously reported data linking cytokinegenotype with clinical course, are consistent with a view that inflammation is a contributorycause for disease pathogenesis or progression. Inflammation may act alone or perhaps inconcert with congenital defects, environmental exposures, or chronic hemodynamicderangements to result in the clinical phenotype. Our results do not prove that inflammatory
mechanisms are causative of disease or directly influence the disease progression, but there isa growing body of evidence that is consistent with such hypotheses (10,17). In our study, choiceof control tissue for brain AVM nidus has inherent limitations. We have described previouslyour use of brain taken from surgical epilepsy patients (22,23), but others have proposed usingsuperficial temporal arteries (40). Neither of these tissues is ideal, as neither containsintracranial blood vessels of the caliber found in brain AVM nidus. It is unlikely that precisechoice of normal comparator tissue would change the conclusions; as inflammation should beabsent in both normal parenchyma and conductance vessels. Further, the primary purpose toinclude tissues from surgical epilepsy patients is to use as a quality control assay to rule outthe possible effects of surgical trauma. Future work needs to address the mechanisms by whichpro-inflammatory pathways might influence brain AVM growth, progression or rupture. Improved understanding of the disease pathogenesis has the potential to assist in thedevelopment of novel therapeutics. Neurosurgery. Author manuscript; available in PMC 2009 June 1. Acknowledgements
This study was supported in part by PHS grants: R01 NS27713 (WLY), R01 NS34949 (WLY), P01 NS44155 (WLY,
The following members of the UCSF BAVM Study Project contributed to portions of this work including datacollection and analysis: Nancy J. Quinnine, RN; Yongfeng Fan, MD, PhD, Yiqian Zhu, MD, Trudy Poon, MS; VanV. Halbach, MD; Randall T. Higashida, MD; Brad Dispensa, BS; Helen Kim, PhD, and Phillipe Jolivalt. The authorswith manuscript preparation. Abbreviations References
1. Achrol AS, Pawlikowska L, McCulloch CE, Poon KY, Ha C, Zaroff JG, Johnston SC, Lee C, Lawton
MT, Sidney S, Marchuk DA, Kwok PY, Young WL. TNFa-238G>A promoter polymorphism isassociated with increased risk of new hemorrhage in the natural course of patients with brainarteriovenous malformations (Abstract). Stroke 2006;37:638–639.
2. Allavena P, Sica A, Solinas G, Porta C, Mantovani A. The inflammatory micro-environment in tumor
progression: The role of tumor-associated macrophages. Crit Rev Oncol Hematol. 2007
3. Audrain MA, Baranger TA, Moguilevski N, Martin SJ, Devys A, Lockwood CM, Muller JY, Esnault
VL. Anti-native and recombinant myeloperoxidase monoclonals and human autoantibodies. Clin ExpImmunol 1997;107:127–134. [PubMed: 9010267]
4. Campana D, Thompson JS, Amlot P, Brown S, Janossy G. The cytoplasmic expression of CD3 antigens
in normal and malignant cells of the T lymphoid lineage. J Immunol 1987;138:648–655. [PubMed:3098852]
5. Cavanagh SP, Gough MJ, Homer-Vanniasinkam S. The role of the neutrophil in ischaemia-reperfusion
injury: potential therapeutic interventions. Cardiovasc Surg 1998;6:112–118. [PubMed: 9610822]
6. Chen Y, Fan Y, Poon KY, Achrol AS, Lawton MT, Zhu Y, McCulloch CE, Hashimoto T, Lee C,
Barbaro NM, Bollen AW, Yang GY, Young WL. MMP-9 expression is associated with leukocyticbut not endothelial markers in brain arteriovenous malformations. Front Biosci 2006;11:3121–3128. [PubMed: 16720380]
7. Chen Y, Pawlikowska L, Yao JS, Shen F, Zhai W, Achrol AS, Lawton MT, Kwok PY, Yang GY,
Young WL. Interleukin-6 involvement in brain arteriovenous malformations. Ann Neurol 2006;59:72–80. [PubMed: 16278864]
8. Choi JH, Mohr JP. Brain arteriovenous malformations in adults. Lancet Neurol 2005;4:299–308. Neurosurgery. Author manuscript; available in PMC 2009 June 1.
9. Chou WH, Choi DS, Zhang H, Mu D, McMahon T, Kharazia VN, Lowell CA, Ferriero DM, Messing
RO. Neutrophil protein kinase Cdelta as a mediator of stroke-reperfusion injury. J Clin Invest2004;114:49–56. [PubMed: 15232611]
10. Chyatte D, Bruno G, Desai S, Todor DR. Inflammation and intracranial aneurysms. Neurosurgery
1999;45:1137–1146. [PubMed: 10549930]discussion 1146-1137
11. Dahlqvist K, Umemoto EY, Brokaw JJ, Dupuis M, McDonald DM. Tissue macrophages associated
with angiogenesis in chronic airway inflammation in rats. Am J Respir Cell Mol Biol 1999;20:237–247. [PubMed: 9922214]
12. Dasu MR, Barrow RE, Spies M, Herndon DN. Matrix metalloproteinase expression in cytokine
stimulated human dermal fibroblasts. Burns 2003;29:527–531. [PubMed: 12927975]
13. Daugherty A, Dunn JL, Rateri DL, Heinecke JW. Myeloperoxidase, a catalyst for lipoprotein
oxidation, is expressed in human atherosclerotic lesions. J Clin Invest 1994;94:437–444. [PubMed:8040285]
14. del Zoppo GJ, Schmid-Schonbein GW, Mori E, Copeland BR, Chang C-M. Polymorphonuclear
leukocytes occlude capillaries following middle cerebral artery occlusion and reperfusion in baboons. Stroke 1991;22:1276–1283. [PubMed: 1926239]
15. Ferroni P, Basili S, Martini F, Cardarello CM, Ceci F, Di Franco M, Bertazzoni G, Gazzaniga PP,
Alessandri C. Serum metalloproteinase 9 levels in patients with coronary artery disease: a novelmarker of inflammation. J Investig Med 2003;51:295–300.
16. Fleetwood IG, Steinberg GK. Arteriovenous malformations. Lancet 2002;359:863–873. [PubMed:
17. Frosen J, Piippo A, Paetau A, Kangasniemi M, Niemela M, Hernesniemi J, Jaaskelainen J.
Remodeling of saccular cerebral artery aneurysm wall is associated with rupture: histological analysisof 24 unruptured and 42 ruptured cases. Stroke 2004;35:2287–2293. [PubMed: 15322297]
18. Halim AX, Singh V, Johnston SC, Higashida RT, Dowd CF, Halbach VV, Lawton MT, Gress DR,
McCulloch CE, Young WL. Characteristics of brain arteriovenous malformations with coexistinganeurysms: a comparison of two referral centers. Stroke 2002;33:675–679. [PubMed: 11872886]
19. Hao Q, Chen Y, Zhu Y, Fan Y, Palmer D, Su H, Young WL, Yang GY. Neutrophil depletion decreases
VEGF-induced focal angiogenesis in the mature mouse brain. J Cereb Blood Flow Metab2007;27:1853–1860. [PubMed: 17392691]
20. Hashimoto T, Lawton MT, Wen G, Yang GY, Chaly T Jr, Stewart CL, Dressman HK, Barbaro NM,
Marchuk DA, Young WL. Gene microarray analysis of human brain arteriovenous malformations. Neurosurgery 2004;54:410–423. [PubMed: 14744289]discussion 423-415
21. Hashimoto T, Meng H, Young WL. Intracranial aneurysms: links between inflammation,
hemodynamics and vascular remodeling. Neurol Res 2006;28:372–380. [PubMed: 16759441]
22. Hashimoto T, Wen G, Lawton MT, Boudreau NJ, Bollen AW, Yang GY, Barbaro NM, Higashida
RT, Dowd CF, Halbach VV, Young WL. Abnormal expression of matrix metalloproteinases andtissue inhibitors of metalloproteinases in brain arteriovenous malformations. Stroke 2003;34:925–931. [PubMed: 12649522]
23. Hashimoto T, Wu Y, Lawton MT, Yang GY, Barbaro NM, Young WL. Co-expression of angiogenic
factors in brain arteriovenous malformations. Neurosurgery 2005;56:1058–1065. 1058–1065. [PubMed: 15854255]
24. Hashimoto T, Yang GY, Young WL. Abnormal expression of MMP9 and TIMPs in brain
arteriovenous malformations (Abstract). Anesthesiology 2002;96:A721.
25. Hultin LE, Hausner MA, Hultin PM, Giorgi JV. CD20 (pan-B cell) antigen is expressed at a low level
on a subpopulation of human T lymphocytes. Cytometry 1993;14:196–204. [PubMed: 7679964]
26. Kazi M, Thyberg J, Religa P, Roy J, Eriksson P, Hedin U, Swedenborg J. Influence of intraluminal
thrombus on structural and cellular composition of abdominal aortic aneurysm wall. J Vasc Surg2003;38:1283–1292. [PubMed: 14681629]
27. Klebanoff SJ. Myeloperoxidase. Proc Assoc Am Physicians 1999;111:383–389. [PubMed:
28. Klebanoff SJ. Myeloperoxidase: friend and foe. J Leukoc Biol 2005;77:598–625. [PubMed:
Neurosurgery. Author manuscript; available in PMC 2009 June 1.
29. Lifson JD, Rossio JL, Piatak M Jr, Parks T, Li L, Kiser R, Coalter V, Fisher B, Flynn BM, Czajak S,
Hirsch VM, Reimann KA, Schmitz JE, Ghrayeb J, Bischofberger N, Nowak MA, Desrosiers RC,Wodarz D. Role of CD8(+) lymphocytes in control of simian immunodeficiency virus infection and
resistance to rechallenge after transient early antiretroviral treatment. J Virol 2001;75:10187–10199. [PubMed: 11581387]
30. Lucchesi BR, Mullane KM. Leukocytes and ischemia-induced myocardial injury. Annu Rev
Pharmacol Toxicol 1986;26:201–224. [PubMed: 3521455]
31. Maier CM, Hsieh L, Yu F, Bracci P, Chan PH. Matrix metalloproteinase-9 and myeloperoxidase
expression: quantitative analysis by antigen immunohistochemistry in a model of transient focalcerebral ischemia. Stroke 2004;35:1169–1174. [PubMed: 15060315]
32. Moulton KS, Vakili K, Zurakowski D, Soliman M, Butterfield C, Sylvin E, Lo KM, Gillies S,
Javaherian K, Folkman J. Inhibition of plaque neovascularization reduces macrophage accumulationand progression of advanced atherosclerosis. Proc Natl Acad Sci U S A 2003;100:4736–4741. [PubMed: 12682294]
33. Murakami M, Iwai S, Hiratsuka S, Yamauchi M, Nakamura K, Iwakura Y, Shibuya M. Signaling of
vascular endothelial growth factor receptor-1 tyrosine kinase promotes rheumatoid arthritis throughactivation of monocytes/macrophages. Blood 2006;108:1849–1856. [PubMed: 16709927]
34. Nicholls SJ, Hazen SL. Myeloperoxidase and cardiovascular disease. Arterioscler Thromb Vasc Biol
35. Opdenakker G, Van den Steen PE, Dubois B, Nelissen I, Van Coillie E, Masure S, Proost P, Van
Damme J. Gelatinase B functions as regulator and effector in leukocyte biology. J Leukoc Biol
36. Parums DV, Cordell JL, Micklem K, Heryet AR, Gatter KC, Mason DY. JC70: a new monoclonal
antibody that detects vascular endothelium associated antigen on routinely processed tissue sections. J Clin Pathol 1990;43:752–757. [PubMed: 2212067]
37. Pawlikowska L, Tran MN, Achrol AS, McCulloch CE, Ha C, Lind DL, Hashimoto T, Zaroff J, Lawton
MT, Marchuk DA, Kwok PY, Young WL. Polymorphisms in genes involved in inflammatory andangiogenic pathways and the risk of hemorrhagic presentation of brain arteriovenous malformations. Stroke 2004;35:2294–2300. [PubMed: 15331795]
38. Pober JS, Sessa WC. Evolving functions of endothelial cells in inflammation. Nat Rev Immunol
39. Pugin J, Widmer MC, Kossodo S, Liang CM, Preas HLn, Suffredini AF. Human neutrophils secrete
gelatinase B in vitro and in vivo in response to endotoxin and proinflammatory mediators. Am JRespir Cell Mol Biol 1999;20:458–464. [PubMed: 10030844]
40. Shenkar R, Elliott JP, Diener K, Gault J, Hu LJ, Cohrs RJ, Phang T, Hunter L, Breeze RE, Awad IA.
Differential gene expression in human cerebrovascular malformations. Neurosurgery 2003;52:465–478. [PubMed: 12535382]
41. Shimakura A, Kamanaka Y, Ikeda Y, Kondo K, Suzuki Y, Umemura K. Neutrophil elastase inhibition
reduces cerebral ischemic damage in the middle cerebral artery occlusion. Brain Res 2000;858:55–
42. Soares HD, Hicks RR, Smith D, McIntosh TK. Inflammatory leukocytic recruitment and diffuse
neuronal degeneration are separate pathological processes resulting from traumatic brain injury. JNeurosci 1995;15:8223–8233. [PubMed: 8613756]
43. Sugiyama S, Okada Y, Sukhova GK, Virmani R, Heinecke JW, Libby P. Macrophage
myeloperoxidase regulation by granulocyte macrophage colony-stimulating factor in humanatherosclerosis and implications in acute coronary syndromes. Am J Pathol 2001;158:879–891. [PubMed: 11238037]
44. Tejima E, Zhao BQ, Tsuji K, Rosell A, van Leyen K, Gonzalez RG, Montaner J, Wang X, Lo EH.
Astrocytic induction of matrix metalloproteinase-9 and edema in brain hemorrhage. J Cereb BloodFlow Metab 2007;27:460–468. [PubMed: 16788715]
45. Wize J, Sopata I, Smerdel A, Maslinski S. Ligation of selectin L and integrin CD11b/CD18 (Mac-1)
induces release of gelatinase B (MMP-9) from human neutrophils. Inflamm Res 1998;47:325–327. [PubMed: 9754865]
Neurosurgery. Author manuscript; available in PMC 2009 June 1.
46. Yan L, Borregaard N, Kjeldsen L, Moses MA. The high molecular weight urinary matrix
metalloproteinase (MMP) activity is a complex of gelatinase B/MMP-9 and neutrophil gelatinase-associated lipocalin (NGAL). Modulation of MMP-9 activity by NGAL. J Biol Chem
2001;276:37258–37265. [PubMed: 11486009]
47. Young WL, Yang GY. Are there genetic influences on sporadic brain arteriovenous malformations?
Stroke 2004;35:2740–2745. [PubMed: 15472089]
Neurosurgery. Author manuscript; available in PMC 2009 June 1. Figure 1. Immunohistochemical staining of neutrophil marker MPO on sections from un-ruptured and non-embolized brain AVM tissue (figure a–f) and epilepsy (figure g–h) control tissue. Brown color, indicated by arrows, is positive MPO signal, and blue color is the counter staining with hematoxylin of nuclei. Figure a showed that neutrophils were present in the vascular wall and lumen of AVMs. Figure b was photographed under higher power from selected area of the figure a, indicted by rectangle. Figure c showed neutrophils were present in the vascular wall as well as parenchymal tissue of AVMs, and figure d was photographed under higher power from selected area of c, indicted by rectangle. Figure e showed that neutrophils were predominantly present in the vascular wall, and image f showed selected area from e under Neurosurgery. Author manuscript; available in PMC 2009 June 1.
higher magnification. Neutrophils were absent in cortical tissue of epilepsy patient (figure gand h). Representative images from 3 AVM patients and an epilepsy patient; size bar for a, c,
e, and g: 100μm; size bar for b, d, f, and h: 25μm
Neurosurgery. Author manuscript; available in PMC 2009 June 1. Figure 2. Immunohistochemical staining of macrophage/monocyte marker CD68 on sections from un- ruptured and non-embolized brain AVM tissue and epilepsy control tissue. Brown color, shown by arrows, indicates positive CD68 immunoreactivity. Cell nuclei appear blue with hematoxylin counter staining. Figure a showed that macrophages were mainly present in the parenchymal tissue adjacent to the vascular wall, and figure b showed higher magnification of rectangle area from a. Figure c showed that macrophages predominantly reside in the vascular wall and figure d showed higher magnification of rectangle area of c. Similar to figure a, figure e showed that macrophages were mainly present in the parenchymal tissue adjacent to the vascular wall. Figure f was photographed under higher power from selected area, indicted by Neurosurgery. Author manuscript; available in PMC 2009 June 1.
rectangle, of e. Weak CD68 positive signals were also observed in the cortical tissue fromepilepsy patients (figure g and h). Representative images from 3 AVM patients an epilepsy
patient; size bar for a, c, e, and g: 100μm; size bar for b, d, f, and h: 25μm
Neurosurgery. Author manuscript; available in PMC 2009 June 1. Figure 3. Co-localization of MPO and CD68 signal. Adjacent AVM tissue sections were stained with MPO, or CD68 marker. Brown color, shown by arrows, indicates positive MPO, or CD68 immunoreactivity. Cell nuclei appear blue with hematoxylin counter staining. Figure a and e showed that neutrophils and macrophages were present in proximity at the same vessels. Figure b and f were photographed under higher power from selected area, indicted by rectangle, of a,
e respectively. Figure c and g showed that neutrophils and macrophages were present atdifferent locations: neutrophils were mainly present at the inner wall; macrophages weremainly located at the outer vascular wall. Figure d and h were photographed under higher powerfrom selected area, indicted by rectangle, of c, g respectively. Size bar for a, c, e, and g:50μm; size bar for b, d, f, and h: 50μm
Neurosurgery. Author manuscript; available in PMC 2009 June 1. Figure 4.
Comparison of the amount of neutrophil and macrophage between brain AVM patients andepilepsy patients. Cell counting was performed on the slides immunostained with MPO, orCD68. Cell counts were from vascular wall and parenchyma, and normalized by tissue sectionarea (mm2) and the amount of endothelial cells (CD31, pixel). Brain AVM tissues had moreMPO and CD68 than the cortical tissues from epilepsy patients (MPO: 434 ± 333 vs 5 ± 4,P=0.0001; CD68: 454 ± 404 vs 4 ± 2, P=0.0001; cells/mm2/EC mass pixel). Neurosurgery. Author manuscript; available in PMC 2009 June 1. Figure 5. Double staining of MMP-9 (a, green color) and MPO (b, red color) in brain AVM tissue. Yellow color in c indicates co-localization of MMP-9 with MPO. size bar: 50μm Neurosurgery. Author manuscript; available in PMC 2009 June 1. Figure 6. A. Correlation of neutrophil number with MPO level. R2 = 0.99, y = 1.85 – 0.37x, n = 4, P<0.01. B. Correlation of neutrophil number with MMP-9 level. R2 = 0.98, y = 0.25 – 0.05x, n = 4, P<0.01. C. Correlation of MMP-9 with MPO. R2 = 0.99, y = 0.14x – 0.02, n = 4, P < 0.01. Neutrophils were isolated from the peripheral blood of four AVM patients at the density of 2.5 ×105. Three serial dilution of each sample was: 1.25×105, 0.625 ×105, 0.312 ×105. Neurosurgery. Author manuscript; available in PMC 2009 June 1. Figure 7. Correlation of MMP-9 with hemoglobin in brain AVM tissue. R2 = 0.057, y = 0.048x + 9.79, n = 77, P = 0.04 Neurosurgery. Author manuscript; available in PMC 2009 June 1. Figure 8. A. coronal section of mouse brain showing the site of blood infusion and tissue sampling. Arrow indicates the position of blood (in red) infusion into striatum of the mouse brain. Yellow circled area represents the area of tissue sampling for assessing the level of MMPs. B. MMP-9 and MMP-2 level assessed by zymography in mice brain 3hr following whole blood injection. N= 3 for each treatment group. S: MMP standards, 1: 100% of original hematocrit, 2: 50% of original hematocrit, 3: 25% of original hematocrit, 4: normal saline. C. Quantitation (Optical density) of MMP-9 and MMP-2 levels. Neurosurgery. Author manuscript; available in PMC 2009 June 1.
Thirteen years experience in computer systems and network analysis, design and administration on a wide varietyof server and workstation systems. Hands-on experience and extensive knowledge of UNIX, networking, VoIP,languages, databases, architectures, training and day-to-day operations. Emphasis on problem solving, innovativeanalysis and design. Brings an end-to-end perspective to all work. •
GOODRICH AREA SCHOOLS GENESEE, OAKLAND & LAPEER COUNTIES, MI. REGULAR MEETING OF THE BOARD OF EDUCATION Time and Date: 6:00 p.m. – Monday, January 28, 2013 Location: Community Room – High School Building Telephone: 810-591-2201 ROLL CALL: Present: David Cramer, Jeff Gardner, Niki Wiederman, Chip Schultz, Linda Jackson, Ryan Starski and Timothy J
 NIH Public Access
NIH Public Access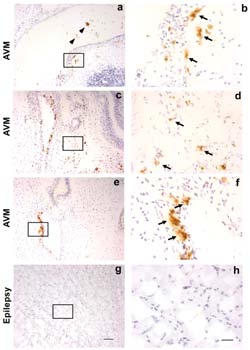 Figure 1.
Figure 1.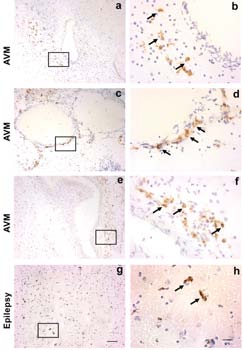 Figure 2.
Figure 2. Figure 3.
Figure 3.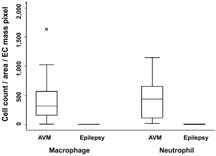 Figure 4.
Figure 4. Figure 5.
Figure 5. Figure 6.
Figure 6.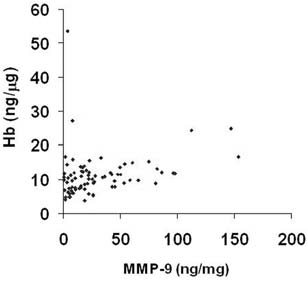 Figure 7.
Figure 7. Figure 8.
Figure 8.