Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Microsoft word - 6623fd7d.doc
NEW PATIENTS' INFORMATION SHEET Please print clearly. Please complete all information so that your claim can be processed quickly and efficiently. Thank you!
Type of Injury: Back Leg Hip Neck Shoulder Arm Head Other:
In Litigation: Yes NO Amount of Medical Benefits: Notice of Compensation Payable: Yes NO
Relationship to Patient: Self /Spouse / Dependent
If the patient is covered by another insurance policy, please complete the following information for coordination of benefits. This information will enable your insurance company to process your claim more quickly. Thank you!
Relationship to Patient: Self /Spouse / Dependent
I hereby assign, transfer, and set over to Center for Pain Control all of my rights, title, and interest to my medical reimbursement benefits under my insurance policy. I authorize the release of any medical information needed to determine these benefits. This authorization shall remain valid until written notice is given by me revoking said authorization. I understand that I am financially responsible for all charges whether or not they are covered by insurance. Patient's Signature
PLEASE COMPLETE THESE FORMS PRIOR TO YOUR APPOINTMENT AND BRING THEM WITH YOU THE DAY OF YOUR SCHEDULED APPOINTMENT. If you are unable to fill them out yourself, please have your family doctor give you a list of your medical history and current medication. You will need to arrive at our clinic 30 min prior to your appointment so we can assist you with this form.
• What is your chief complaint? (example: 30% low back pain and 70% right leg pain)
• When did it start? (example: 2months ago, or “7-26-03”)
• Did you sustain any trauma immediately prior to the onset?
• Is this work related or motor vehicle accident related? • Do you have an attorney? (Please provide their contact information)
• Please describe the trauma.
• Is the pain there constantly, intermittently, or both? (example: constant back pain with intermittent left leg pain)
• Please describe the characteristics of your pain. (sharp vs. dull, burning, squeezing, throbbing, tingling, etc.)
• What makes the pain worse? (Please circle)
Sitting Standing Walking Lying flat Bending over Lifting Others
• What makes the pain better? (Please circle)
Sitting Standing Walking Lying flat Lifting Change Positions Other_________________
• What have you tried?
Dosage? H o w l o n g ? Helpful?
Hydrocodone/APAP (Vicodin, Lortab, Norco)
Oxycodone/APAP (Percocet, Endocet, Tylox, Roxicet)
How long? Helpful? Reason stopped
• Images (X-Ray, CT Scan, Bone Scan, etc.) Study Date Where
• Spine Injections
Helpful? How long did it last?
• Spine surgery
Helpful? How long did it last? • Current Medication (Please list all meds including vitamins and OTC meds) Medication Why prescribed • Are you allergic to any medications? (Please list and describe reaction) Medication Reaction
IV contrast allergy? Shellfish allergy?
• Past Medical History (Please circle all)
AIDS / HIV Alcoholism Asthma Cancer Diabetes Emphysema Epilepsy Heart Disease
Hepatitis Herpes High Blood Pressure Multiple Sclerosis Pacemaker Seizures Stroke
Thyroid Disorders Tuberculosis Fibromyalgia Depression Bipolar Disorder Schizophrenia
Anxiety Disorder Other Psychiatric Issues Irritable Bowel Syndrome Chronic Pelvic Pain Migraine
• Past Surgical History
• Family History (Please list all significant family medical history such as bleeding problems (hemophilia), psychiatric
disorders, chronic pain, or any substance abuse) • Social history
Who do you live with now?
Are you currently working? If not, why not?
Have you ever gone through rehab for drug or alcohol abuse? .
Are you currently pregnant or plan to become pregnant?
Have you ever been discharged from a doctor’s office because of noncompliance not following their directions?
• Review of system
In the past month, have you experience any significant (Please circle all)
Weight loss/gain Fever/chills Changes in hearing/vision Dizziness Pass out Shortness of breath
Productive cough Chest pain Abdominal pain Diarrhea/constipation Weakness in the extremities
Lost control of bowel/urinary functions Bleeding problems Rashes Depression Suicidal thoughts
Homicidal thoughts Others ________________________
• Please shade in on the drawings the areas where you feel pain.
Please rate the severity of your pain (mark “baseline” and “with exacerbation”)
BASELINE WITH ACTIVITY • Who has treated you since the onset of the chief complaint?
Varese, 2 Maggio 2011 COMUNICATO STAMPA EVENTI AL PARCO DEL CAMPO DEI FIORI Nell'ambito del progetto Viaggiando Liberty il Parco Campo dei Fiori ha organizzato una serie di eventi culturali e ricreativi e alcuni momenti di studio e ricerca. L’insieme di azioni che verranno proposte intendono valorizzare aspetti architettonici, culturali e artistici del Parco e valorizzarne e pr
[.] In the last years the introduction of UVB fototherapy, PUVA therapy, usage of biological products and, in nations of Germanic area, usage of fumaric acid derivatives led to a concept of long term biological modulation in psoriasis. (www.poscare.it/terapia) PRODUCT NAME: PSOCAPS PRODUCT CATEGORY Food supplement based on salts of fumaric acid LIST OF INGREDIENTS ACCORDING TO TYPE AND

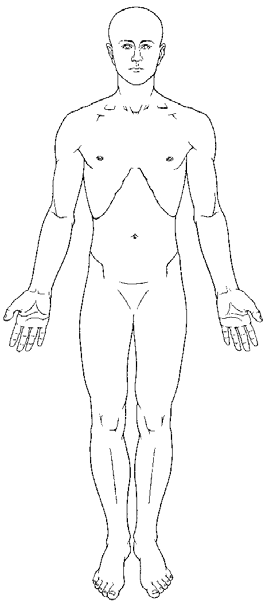
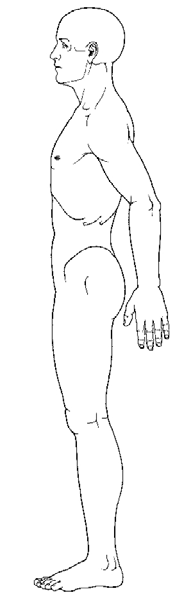
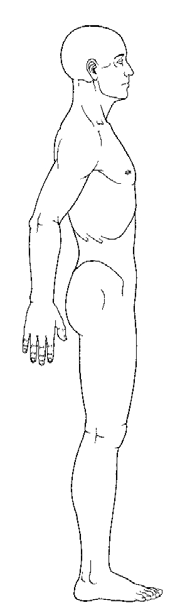
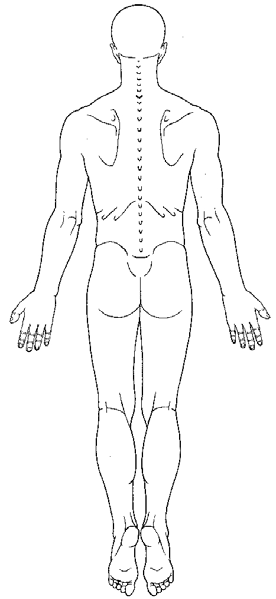
 • Please shade in on the drawings the areas where you feel pain.
• Please shade in on the drawings the areas where you feel pain.