Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Untitled
Anterior Vitrectomy
The art of visualizing the vitreous. BY SCOTT E. BURK, MD, PHD; ANDREA P. DA MATA , MD; ROBERT H. OSHER, MD; AND ROBERT J. CIONNI, MD
Vitreous gel, transparent by design, is virtually the agent. On the contrary, eyes receiving intracameral
invisible under the operating microscope.
triamcinolone have a quieter postoperative course versus
Furthermore, it is particularly unwelcome in
those in which the agent is not used.
makes surgery more difficult and is associatedwith a variety of serious intraoperative andpostoperative complications such as a droppedlens fragment, corneal edema, cystoid macularedema, retinal detachment, and endophthalmi-tis.1-14 Fortunately, meticulous vitreous clean-up can reduce the incidence of many vision-threatening complications associated with vit-reous loss.9 Until recently, however, surgeonshad only indirect intraoperative clues to deter-mine if vitreous gel were present in the anteriorchamber and, if so, to what extent.
Triamcinolone acetonide (Kenalog; Bristol-
Myers Squibb Company, New York, NY) hasproven quite useful for visualizing vitreous inthe anterior chamber15 and has become a rou-tine part of our practice for complicatedcataracts with large zonular dialyses. To date,we have performed more than 200 cases of tri-
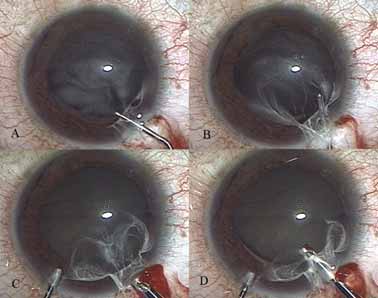
Figure 1. The surgeon injects triamcinolone acetonide into the prolapsed
amcinolone-assisted anterior vitrectomy and
vitreous (A and B) and then performs an anterior vitrectomy (C and D).
have not seen a complication attributable to
Note the vitreous present in the wound at the time of injection. APRIL 2005 I CATARACT & REFRACTIVE SURGERY TODAY I 61 P R E PA R AT I O N A LT E R N AT I V E S
We continue to prepare triamcinolone as originally
Realizing that the vitreous gel will capture and hold
described15 and remove the preservative by a sterile
nearly any particulate matter, some groups are evaluat-
capture-and-wash technique. Our decision is based on
ing alternative techniques of vitreous identification. The
a lack of data regarding the intracameral effects of ben-
most notable is 11-deoxycortisol, a steroid precursor
zyl alcohol, the preservative in Kenalog. Clearly, howev-
er, our original washing technique is a bit tedious, par-
Nonetheless, we prefer triamcinolone acetonide because
ticularly when the encounter with vitreous is unexpect-
it is readily available, is nontoxic,17-19 and has a 25-year
ed or the OR staff is unfamiliar with the technique.
track record for intraocular use since it was first described
It is therefore not surprising that one of the most
in 1980 by Tano et al.20 In addition, one should not under-
common questions regarding intracameral triamcino-
estimate the role of intracameral triamcinolone in stabiliz-
lone is, “Can the preparation be simplified?” There are
ing the blood-aqueous barrier and minimizing inflamma-
actually several options (and wide variation among sur-
tion on postoperative day one in complicated anterior
geons) that range from using the agent directly out of
the bottle to simple dilution. Others fill a syringe withtriamcinolone, stand it inverted until the particles set-
Q U E S T I O N S
tle, express the vehicle, and resuspend the triamci-
To date, two questions about triamcinolone-assisted
nolone particles in the desired volume of BSS. In addi-
vitrectomy are unresolved. As mentioned earlier, the
tion, compounding pharmacies sell preservative-free
first regards the method of preparation and the effects
triamcinolone, but it has a limited shelf life.
of the benzyl alcohol preservative. The use of preserva-tive-free or washed triamcinolone makes intuitive sense,
T E C H N I Q U E
but we are unaware of any evidence suggesting that the
When asked the best way to use triamcinolone, the
removal of the benzyl alcohol preservative is helpful or
answer is not to lose vitreous in the first place. The
next best answer is to get lots of practice. Neither reply
The second question relates to the probability of
is practical for most surgeons, who instead must gain
steroid-induced glaucoma. It is well known that our vit-
insight from the experience of others. Here at the Cin-
reoretinal colleagues observe increased IOP after the
cinnati Eye Institute, we typically withdraw 0.2mL of
depot injection of an intraocular steroid. Indeed, the
40mg/mL triamcinolone acetonide, then wash and
amount of steroid deposited correlates with the per-
resuspend the agent in 2.0mL of BSS (10X dilution).
centage of patients experiencing elevated IOPs and with
Much higher concentrations tend to leave too much
unbound triamcinolone in the anterior chamber,
Although it is certainly possible that an eye will devel-
whereas a larger volume of a lower concentration of
op glaucoma after undergoing triamcinolone-assisted
triamcinolone tends to distribute the particles more
anterior vitrectomy, we have not observed this complica-
tion. Furthermore, the risk of steroid-induced glaucoma
Ideally, one injects the agent directly within the sub-
seems to be minimal when the surgeon uses a small
stance of the vitreous to obtain maximum visualiza-
amount of triamcinolone and then removes most of it
tion. Dusting the surface of the gel works, but only
along with the vitreous gel that was identified. In sum-
until one has removed the surface, at which point rein-
mary, we have found triamcinolone acetonide to be safe
jection is necessary. Dr. Burk likes to swirl a little triam-
and quite useful for identifying and removing vitreous. ■
cinolone around the anterior chamber to get an over-view of the situation. He then buries the cannula’s tip
Scott E. Burk, MD, PhD, is Clinical Ophthalmolo-
within the gel and makes a very controlled injection. It
gist at the Cincinnati Eye Institute and Volunteer
is important to remember that, if the vitreous is near
Faculty for the Department of Ophthalmology,
the wound and fluid comes out upon the injection, so
University of Cincinnati College of Medicine. He
will vitreous. Inserting the cannula through the para-
states that he holds no financial interest in any
centesis often avoids such reflux. Vitrectomy should be
product or company mentioned herein. Dr. Burk may be
performed with a high cutting rate, a low aspiration
rate, and separate irrigation. Although not always
needed, a pars plana approach can be quite helpful,
Robert J. Cionni, MD, is Medical Director of
particularly for vitreous at the site of the corneal inci-
the Cincinnati Eye Institute. He states that heholds no financial interest in any product or62 I CATARACT & REFRACTIVE SURGERY TODAY I APRIL 2005 Vision of a perfect flap may overlooksafety advantages of microkeratomesover the IntraLase FS devicecompany mentioned herein. Dr. Cionni may be reached at(513) 984-5133; rcionni@cincinnatieye.com.Andrea P. Da Mata, MD, is Research Ophthal-mologist at the Cincinnati Eye Institute. She statesAlthough there is more than one waythat she holds no financial interest in any prod-to create a flap, some surgeons may beuct or company mentioned herein. Dr. Da Mataswayed by the perceived advantages ofmay be reached at (513) 984-5133; using the IntraLase femtoseconddevice instead of the microkeratometo solve a problem that, in essence, hasRobert H. Osher, MD, is a professor in theDepartment of Ophthalmology at the Uni-versity of Cincinnati College of Medicine and isphysicians should be aware of someMedical Director Emeritus at the Cincinnati Eye
Robert K. Maloney, MD important safety concerns associatedInstitute. Dr. Osher is also the founder and edi-tor of the Video Journal of Cataract and Refractive Sur-gery. He states that he holds no financial interest in anyThough rare, flap complications can occur with both methods.product or company mentioned herein. Dr. Osher may beIt really comes down to the type of problem a surgeon wouldreached at (513) 984-5133; rhosher@cincinnatieye.com.prefer to deal with. My practice receives a lot of referrals forcomplications, so I have the opportunity to see many of the
1. Shah DP, Krishnan AA, Albanis CV, et al. Visual acuity outcomes following vitreous
problems associated with both microkeratomes and the
loss in glaucoma and diabetic patients. Eye. 2002;16:271-274. 2. Tan JH, Karwatowski WS. Phacoemulsification cataract surgery and unplanned ante-
IntraLase device. In my experience, microkeratomes are more
rior vitrectomy—is it bad news? Eye. 2002;16:117-120. likely to cause buttonholes, whereas the IntraLase device
3. Ionides A, Minassian D, Tuft S. Visual outcome following posterior capsule rupture
appears to be more frequently associated with flap tears.
during cataract surgery. Br J Ophthalmol. 2001;85:222-224. Referring surgeons have also mentioned loss of suction with the
4. Chitkara DK, Smerdon DL. Risk factors, complications, and results in extracapsularcataract extraction. J Cataract Refract Surg. 1997;23:570-574. IntraLase device – a complication caused by the time required
5. Berrod JP, Sautiere B, Rozot P, Raspiller A. Retinal detachment after cataract surgery. to make the flap. Some surgeons – I being one of them – find it
Int Ophthalmol. 1996-1997;20:301-308. easier to manage buttonhole flaps, and are therefore better off
6. Frost NA, Sparrow JM, Strong NP, Rosenthal AR. Vitreous loss in planned extracap-
using the microkeratome. For doctors who are more comfort-
sular cataract extraction does lead to a poorer visual outcome. Eye. 1995;9(pt 4):446-451. able coping with flap tears, the IntraLase device may be a more
7. Banker AS, Freeman WR. Retinal detachment. Ophthalmol Clin North Am. 2001;14:
695-704. 8. Drolsum L, Haaskjold E. Causes of decreased visual acuity after cataract extraction. While the IntraLase is widely marketed as a better way to create
J Cataract Refract Surg. 1995;21:59-63. flaps, there is data that suggests that its complication rates are
9. Spigelman AV, Lindstrom RL, Nichols BD, Lindquist TD. Visual results following vit-reous loss and primary lens implantation. J Cataract Refract Surg. 1989;15:201-204. similar to the microkeratome, and that in fact, it can present
10. Balent A, Civerchia LL, Mohamadi P. Visual outcome of cataract extraction and lens
additional, unique problems. Visual recovery with Intralase
implantation complicated by vitreous loss. J Cataract Refract Surg. 1988;14:158-160. appears to take longer, with referring IntraLase surgeons telling
11. Berger BB, Zweig KO, Peyman GA. Vitreous loss managed by anterior vitrectomy. me of 20/20 to 20/30 acuities day one post op versus the 20/15,
Long-term follow-up of 59 cases. Arch Ophthalmol. 1980;98:1245-1247. 12. Kanski JJ, Ramsay JH. Vitrectomy techniques in the management of complications
20/20 I typically see in my keratome patients. Currently, there is
in cataract surgery. Trans Ophthalmol Soc UK. 1980;100(pt 1):216-218.
no substantive scientific or clinical proof that IntraLase offers
13. Mamo JG. Late effects of vitreous loss. Ann Ophthalmol. 1974;6:935-941. advantages over the microkeratome, and it will take time to
14. Ruiz RS, Teeters VW. The vitreous wick syndrome. A late complication following
confirm longer-term visual results.
cataract extraction. Am J Ophthalmol. 1970;70:483-490. 15. Burk SE, Da Mata AP, Snyder ME, et al. Visualizing vitreous using Kenalog suspen-sion. J Cataract Refract Surg. 2003;29:645-651. A new area of concern involves track-related iridocyclitis and
16. Kaji Y, Hiraoka T, Okamoto F, et al. Visualizing the vitreous body in the anterior
scleritis (TRISC), a condition that can surface with the IntraLase
chamber using 11-deoxycortisol after posterior capsule rupture in an animal model. device. This syndrome can be extremely debilitating – forcingpatients to wear sunglasses indoors for months and endure
17. McCuen BW 2nd, Bessler M, Tano Y, et al. The lack of toxicity of intravitreallyadministered triamcinolone acetonide. Am J Ophthalmol. 1981;91:785-788. aggressive steroid therapy. Topical corticosteroids can elevate
18. Hida T, Chandler D, Arena JE, Machemer R. Experimental and clinical observations
IOP and induce fluid accumulation in the interface. This may
of the intraocular toxicity of commercial corticosteroid preparations. Am J Ophthalmol. lead to falsely low IOP readings, which could potentially result
19. Young S, Larkin G, Branley M, Lightman S. Safety and efficacy of intravitreal triam-cinolone for cystoid macular oedema in uveitis. Clin Experiment Ophthalmol. 2001;29:2-6. When considering a flap-creation method, physicians should
20. Tano Y, Chandler D, Machemer R. Treatment of intraocular proliferation with intrav-
take into account all of these factors.
itreal injection of triamcinolone acetonide. Am J Ophthalmol. 1980;90:810-816.
PET HEALTH BULLETIN Summer 2011/12 1. An Itchy Dog possible. Fly repellent containing permethrin or pyrethrin can be warmer, is your dog starting to itch? Are they rubbing, scratching and chewing their skin until it becomes bald, red, inflamed and painful? If so, let us explore some of the most common If Fluffy suddenly starts itching after venturing out to bush or farmland,
J Oral Pathol Med (2004) 33: 445–50ª Blackwell Munksgaard 2004 Æ All rights reservedOral histoplasmosis associated with HIV infection:a comparative studyS. L. Herna´ndez1, S. A. Lo´pez de Blanc1,2, R. H. Sambuelli3,4, H. Roland3, C. Cornelli3, V. Lattanzi1,M. A. Carnelli41Clinical Stomatology B, School of Dentistry, National University of Co´rdoba, Co´rdoba; 2Department of Oral Pathol
 Anterior
Anterior
 P R E PA R AT I O N
P R E PA R AT I O N 

 Vision of a perfect flap may overlooksafety advantages of microkeratomesover the IntraLase FS device
company mentioned herein. Dr. Cionni may be reached at
(513) 984-5133; rcionni@cincinnatieye.com.
Andrea P. Da Mata, MD, is Research Ophthal-
mologist at the Cincinnati Eye Institute. She states
Although there is more than one way
that she holds no financial interest in any prod-
to create a flap, some surgeons may be
uct or company mentioned herein. Dr. Da Mata
swayed by the perceived advantages of
may be reached at (513) 984-5133;
using the IntraLase femtoseconddevice instead of the microkeratome
to solve a problem that, in essence, has
Robert H. Osher, MD, is a professor in the
Department of Ophthalmology at the Uni-
versity of Cincinnati College of Medicine and is
physicians should be aware of some
Medical Director Emeritus at the Cincinnati Eye
Robert K. Maloney, MD important safety concerns associated
Institute. Dr. Osher is also the founder and edi-
tor of the Video Journal of Cataract and Refractive Sur-gery. He states that he holds no financial interest in any
Though rare, flap complications can occur with both methods.
product or company mentioned herein. Dr. Osher may be
It really comes down to the type of problem a surgeon would
reached at (513) 984-5133; rhosher@cincinnatieye.com.
prefer to deal with. My practice receives a lot of referrals forcomplications, so I have the opportunity to see many of the
1. Shah DP, Krishnan AA, Albanis CV, et al. Visual acuity outcomes following vitreous
problems associated with both microkeratomes and the
loss in glaucoma and diabetic patients. Eye. 2002;16:271-274.
Vision of a perfect flap may overlooksafety advantages of microkeratomesover the IntraLase FS device
company mentioned herein. Dr. Cionni may be reached at
(513) 984-5133; rcionni@cincinnatieye.com.
Andrea P. Da Mata, MD, is Research Ophthal-
mologist at the Cincinnati Eye Institute. She states
Although there is more than one way
that she holds no financial interest in any prod-
to create a flap, some surgeons may be
uct or company mentioned herein. Dr. Da Mata
swayed by the perceived advantages of
may be reached at (513) 984-5133;
using the IntraLase femtoseconddevice instead of the microkeratome
to solve a problem that, in essence, has
Robert H. Osher, MD, is a professor in the
Department of Ophthalmology at the Uni-
versity of Cincinnati College of Medicine and is
physicians should be aware of some
Medical Director Emeritus at the Cincinnati Eye
Robert K. Maloney, MD important safety concerns associated
Institute. Dr. Osher is also the founder and edi-
tor of the Video Journal of Cataract and Refractive Sur-gery. He states that he holds no financial interest in any
Though rare, flap complications can occur with both methods.
product or company mentioned herein. Dr. Osher may be
It really comes down to the type of problem a surgeon would
reached at (513) 984-5133; rhosher@cincinnatieye.com.
prefer to deal with. My practice receives a lot of referrals forcomplications, so I have the opportunity to see many of the
1. Shah DP, Krishnan AA, Albanis CV, et al. Visual acuity outcomes following vitreous
problems associated with both microkeratomes and the
loss in glaucoma and diabetic patients. Eye. 2002;16:271-274.