Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Equoterapianet.com.br
& 2003 International Spinal Cord Society All rights reserved 1362-4393/03 $25.00
The short-term effect of hippotherapy on spasticity in patients with spinalcord injury
HE Lechner*,1, S Feldhaus2, L Gudmundsen2, D Hegemann2, D Michel2, GA Za¨ch2 and H Knecht1
1Institute for Clinical Research, Swiss Paraplegic Centre, Nottwil, Switzerland; 2Swiss Paraplegic Centre,Nottwil, Switzerland
Study design: Assessment of spasticity before and after hippotherapy treatment. Objective: To evaluate the short-term effect ofhippotherapy on spasticity ofspinal cord injuredpatients (SCIs). Setting: Swiss Paraplegic Centre, Nottwil. Methods: 32 patients with spinal cord injury with various degrees ofspasticity had repeatedsessions (mean 11) ofHippotherapy-Ks. Spasticity ofthe lower extremities was scoredaccording to the Ashworth Scale. Results: In primary rehabilitation patients Ashworth values after hippotherapy weresignificantly lower than before (Wilcoxon’s signed-rank test: Po0.001). Highest improvementswere observed in SCIs with very high spasticity. No significant difference between short-termeffect in paraplegic and short-term effect in tetraplegic subjects was found. Conclusions: Hippotherapy significantly reduces spasticity oflower extremities in SCIs. Spinal Cord (2003) 41, 502–505. doi:10.1038/sj.sc.3101492
Keywords: hippotherapy; muscle spasticity; spinal cord injuries; rehabilitation; treatment
Spasticity is known as an accompanying phenomenon of
spasticity are even more scarce. Unlike therapeutic
spinal cord injuries and was defined by Lance1 as an
horseback riding, which teaches riding skills to indivi-
increased reflex activity, as well as a velocity-dependent
duals with disabilities, hippotherapy is a neurophysio-
increase in muscle tone elicited by passive stretching.
logical treatment that uses the movement ofthe horse.
Not every patient suffering from spasticity necessarily
The hypothesis is that the rhythmical side flexion and
requires treatment. However, depending on the severity
extension ofthe patient’s trunk combined with trunk
ofspasticity it may interfere with activities ofdaily life.
torsion have a beneficial effect on spasticity. The
In the Stockholm spinal cord injury study,2 for example,
working mechanism ofhippotherapy on spasticity may
more than 41% ofsubjects with spastic paralysis
be complex. According to neurophysiological standards,
reported excessive spasticity associated with additional
an inhibition ofthe spasticity is achieved through the
functional impairment and/or pain, and 2/3 of the
saddle position in hip flexion – abduction – external
subjects with spastic paralysis took medication to treat
rotation as well as through rhythmical and three-
their spasticity.3 What other possibilities besides medi-
dimensional equine movements communicated to the
cation are there to reduce high muscle tone?
patients’ pelvis and trunk.6,7 A further impact on
For several years hippotherapy has been used in
spasticity is also attributed to the psychosomatical
rehabilitation ofspinal cord injured patients (SCIs) and
effects.5 According to Strauss8 hippotherapy gains its
positive effects on spasticity have been reported.4,5
unique effect through a neural facilitation, sensorimotor
Unfortunately, only few studies assessing the effect of
stimulation and psychosomatic influence.
hippotherapy on spasticity have been conducted, and
We felt that there is a need for a study assessing the
most ofthe existing literature is not in the English
effect ofhippotherapy on spasticity ofSCIs and to
language. Studies that aim at explaining the mechanisms
report the result in the English language. We have tested
underlying the positive effect ofhippotherapy on
the short-term effect ofhippotherapy onto the increasedmuscle tone ofthe lower extremities in 32 SCIs asfollows: the physiotherapist in charge rated the spasti-
*Correspondence: HE Lechner, Institute for Clinical Research, SwissParaplegic Centre, Nottwil 6207, Switzerland
city ofthe patients directly prior to and af
Effect of hippotherapy on spasticity in SCIHE Lechner et al
hippotherapy treatment according to the Ashworth
On average each patient was tested prior and after 11(range: 5–24) hippotherapy sessions. The treatmentswere performed according the concept of Hippotherapy-
Ks (HTK).11 The subject sat on a sheepskin (withoutsaddle), while the horse (Icelander) was led at walking
pace by a skilled equestrian. The physiotherapist walked
From June 1996 to November 1997 and from June 1999
beside the horse facilitating postural responses and
to May 2001 all patients with various degrees of
repositioning the patient ifnecessary. Some patients
spasticity were tested by the physiotherapists prior to
with high lesions needed a second physiotherapist sitting
and after hippotherapy treatment. Measurements were
on the horseback behind them for stabilisation. One
taken from 32 SCIs. The age ranged between 16 and 72
years (mean 37), four of the patients were female, 30subjects were inpatients in primary rehabilitation (timeafter injury between 1 and 18 months, mean 5), and two
were outpatients (4 and 6 years after injury). Levels of
Rating of spasticity was done directly before and after
the spinal cord injury were between C4 and T12 and
the hippotherapy session in the riding hall. The patient
between A and D according to the ‘ASIA Impairment
was lying on an examining table in supine position while
Scale’10 (Table 1). Informed consent of all patients was
eight movement directions were rated: hip flexion and
obtained according to the Helsinki protocol.
extension, abduction and adduction, knee flexion and
Effect of hippotherapy on spasticity in SCI
extension, as well as ankle dorsi- and plantarflexion. Thephysiotherapist moved the limb in the directions asquickly as possible. The knees and the ankles weremeasured with extended hips, while the lower legsdangling off the end ofthe testing bed. Each directionwas repeated three to five times. She rated the elicitedspasticity according to the Ashworth Scale between 1and 5 (Ashworth-value, ASV) (Table 2). The ASV oftheeight movement directions ofboth sides were recordedas a sum of16 scores ranging from a minimum of16 to amaximum of80.
Testing was performed prior to and after the HTK
treatment by the same physiotherapist. Seven differentphysiotherapists performed the overall testing of the 32patients. All seven physiotherapists were instructed onthe testing by the same person and met on a regularbasis to exchange testing experiences and to check inter-and intrarater reliability.
Scatterplot ofthe 32 subjects: means ofsums of
For each patient and examination sums ofthe ASV
ASV before versus sums of ASV after HTK treatment. The 451
from all directions on both sides were calculated (2 Â 8
line indicates values ofno change. All measured values show
movement directions, minimum score ¼ 16, maximum
smaller sums of ASV after than before HTK treatment. Note:
score ¼ 80). Means and standard deviations were
score of16 signifies a patient with no spasticity
calculated ofthe repeated HTK treatments f
patient. The existence ofa statistical difference between
the ASV before and after HTK treatment was assessed
(X10.0) was observed in six patients with severe
by performing Wilcoxon’s signed-rank test. Statistical
before-session spasticity (ASV over 38).
significance12 was set at the 5% level.
There was no significant difference between short-term
effect in paraplegic subjects and the short-term effect
in tetraplegic subjects (Wilcoxon’s signed rank test:P ¼ 0.4). The mean ofall differences between before- and
A total of351 hippotherapy treatments were performed
after-session values for paraplegic subjects (n ¼ 18) was
and 327 ofthese sessions (93%) lead to a lower ASV
À3.4 (SD72.2) and for all tetraplegic subjects (n ¼ 14) it
immediately after as compared than before the sessions.
was À2.8 (SD71.0). There was no longitudinal effect
In all, 20 sessions (6%) did not lead to a change in the
(downward trend overall sessions in each patient) and
ASV score; these sessions were completed by 10 patients
the variance within the before-session values in each
with low ASV (p24) prior to treatment. In only two
single patient ranged from 0.81 to 77.4 (SD70.9–78.8).
patients with very low ASV (p18) an increase ofthe
Also, there was no detectable trend ofthe before- and
value was measured twice in each patient (1%).
after-session differences (data not shown).
Hippotherapy led to a substantial decrease ofmuscle
tone in the lower extremities ofthe 32 SCI patients. Thecalculated means ofall individual patients ranged from
17.6 to 53.3 prior to treatment and from 16.6 to 42 after
Our results show that hippotherapy causes an immediate
treatment (Table 1). Group scores after the treatment
reduction ofspasticity ofthe lower extremities ofSCI
were significantly lower than group scores before
patients. The ASV was significantly lower after the
treatment than before. The greatest before- and after-session differences were measured in patients with very
Hippotherapy and its reducing effect on the muscle
tone was described earlier in connection with otherclinical entities associated with spasticity such as multi-
ple sclerosis (MS) and cerebral palsy (CP): in the ‘Swiss
Slight increase in tone giving a ‘catch’ when the limb
Study’ by Kuenzle and Wuethrich13 including 255
patients with MS, relaxation and decrease in muscle
More marked increase in tone but limb easily flexed
tone was the most frequent effect of hippotherapy,
Considerable increase in tone – passive movement
according to subjective records ofpatients, therapists
and treating doctors. However, these results were not
backed up by Ashworth Scale. In another study with
Effect of hippotherapy on spasticity in SCIHE Lechner et al
MS patients, a reduction in the muscle tone ofthe lower
valuable supplement to the conventional physiotherapy
extremities after hippotherapy was measured by electro-
approach in holistic rehabilitation ofSCIs.
Tarnow15 ascertained that children and teenagers with
a spastic quadriplegia had shown a clear improvement
We thank all the subjects who participated in the study and we
in their trunk flexibility and their functional ability after
gratefully acknowledge the financial support of the Swiss
treatment with hippotherapy. She attributed the results
to a decrease in muscle tone as a result ofthis treatment. McGibbon et al16 described a standardised protocol ofhippotherapy treatment and documented its effect on
gait, energy expenditure, and gross motor function inchildren with spastic CP. Bertoti6 examined the effect of
1 Lance JW. Symposium synopsis. In: Feldman RG, Young
RR, Koulla WP (eds). Spasticity: Disordered Motor Control.
hippotherapy on the posture ofchildren with CP and
Yearbook Medical Publishers: Chicago 1980, pp 485–494.
described improved posture because ofthe hippother-
2 Levi R, Hultling C, Nash MS, Seiger A. The Stockholm
apy’s reducing effect on spasticity. Exner et al4 described
Spinal Cord Injury Study: 1. Medical problems in a
a ‘clear suppression ofthe spasticity’ with a ‘remarkable
regional SCI population. Paraplegia 1995; 33: 308–315.
duration ofeffect’; however, the degree ofthe decrease
3 Skold C, Levi R, Ake S. Spasticity after traumatic spinal
in spasticity was not stated quantitatively.
cord injury: nature, severity and location. Arch Phys Med
In our study, the spasticity was rated according to the
ASV directly prior and after treatment in primary
4 Exner G, Engelmann A, Lange K, Wenck B. Grundlagen
rehabilitation patients. Our results represent a short-
und Wirkung der Hippotherapie im Konzept der umfas-
term effect ofhippotherapy. However, it would be
interesting to quantitatively evaluate the duration ofthe
5 Hegemann D, Za¨ch G. Hippotherapie zur Behandlung der
effect as well as a possibly persisting effect in the context
Spastizita¨t bei Para- und Tetraplegikern (German). In:
urther prospective study, since in the ‘Swiss
Grueninger W (ed). Spinale Spastik. Ueberreuter Verlag:
Study’13 in over 70% ofMS patients a benefit of2 days
6 Bertoti DB. Effect oftherapeutic horseback riding on
Naturally, medication would have to be kept constant
posture in children with cerebral palsy. Phys Ther 1988;
ifchanges in the severity ofspasticity over a series of
hippotherapy sessions were to be investigated. This
7 Wuethrich R, Kuenzle U. Hippothe´rapie chez des patients
would have to be conducted with chronic SCIs, as
atteints de scle´rose en plaques. J Beige Med Phys Rehabil
during first rehabilitation there are many more con-
8 Strauss I. Hippotherapy: Neurophysiological Therapy on the
founding factors like psychological stress, bladder
Horse. Ontario Therapeutic Riding Association: Thornhill,
infections or bowel complications, changes of therapies
9 Ashworth B. Preliminary trial ofcarisoprodol in multiple
have an effect on muscle tone. To evidence a long-
sclerosis. Practitioner 1964; 192: 540–542.
itudinal effect ofhippotherapy on spasticity, we just
10 Maynard FMJ et al. International standards for neurolo-
started a blinded long-time prospective study on chronic
gical and functional classification of spinal cord injury.
SCIs with stable antispastic medication, who are at least
American Spinal Injury Association. Spinal Cord 1997;
Regarding the rating ofmuscle tone with the Ash-
11 Kuenzle U. Hippotherapie auf den Grundlagen der Funktio-
worth Scale, it needs to be mentioned that it is clearly a
nellen Bewegungslehre Klein-Vogelbach. Hippotherapie-K:Theorie, Praktische Anwendung Wirksamkeitsnachweis.
subjective method. Additionally, the physiotherapist
Springer-Verlag: Berlin Heidelberg, 2000.
conducting the measurement was not blinded to the
12 Sheskin DJ. Handbook of Parametric and Nonparametric
treatment and ratings may have been influenced by
Statistical Procedures. 2nd edn. Chapman & Hall/CRC
13 Kuenzle U, Wuethrich R. Schweizerische Studie u¨ber die
Wirksamkeit der Hippotherapie K bei Multiple-Sklerose-
Patienten. In: Kuenzle U (ed). Hippotherapie auf denGrundlagen der Funktionellen Bewegungslehre Klein-Vogel-
We show that hippotherapy has an alleviating short-
bach. Springer-Verlag: Berlin, Heidelberg 2000, pp 359–381.
term effect on spasticity ofthe lower extremities in SCI
14 Weber A. Hippotherapie bei Multiple-Sklerose-Kranken.
patients. In 32 patients such an effect could be shown
with the help ofthe Ashworth Scale. There was a
15 Tarnow A. Hippotherapeutische Behandlungsergebnisse –
significant difference between the spasticity before and
(German). Oeff Gesundh Wesen 1979; 41: 201–205.
16 McGibbon NH, Andrade CK, Widener G, Cintas HL.
Further studies regarding the duration ofthe effect
Effect ofan equine-movement therapy program on gait,
are necessary and will be performed with blinded
energy expenditure, and motor function in children with
assessment ofspasticity reduction, comparing it with
spastic cerebral palsy: a pilot study. DevMed Child Neurol
other interventions. In summary, hippotherapy is a
Remembering, Forgetting, and the Message of Purim ----------------------------------------------------The Shabbat before Purim has traditionally been called Shabbat Zachor , or the “Sabbath of Remembering.” The additional Torah portion read on this Shabbat is Deuteronomy 25:17–19. Remember what Amalek did to you along the way when you came out from Egypt, how he met you alongthe way a
Tekniska detaljer Serie 40 Ulrich Hermann Tastaturbau, www.uht-tastaturen.de , contact@uht-tastaturen.de - Kan komma att ändras! – Tekniska detaljer Serie 40 Kännetecken för SERIE 40 optimerad tryckpunkt och tangentanslag genom optimal vinkel enkelt att komma åt alla tangentdetaljer klaviaturen kan öppnas på två olika sätt anslutning på baksidan eller undersidan av
 & 2003 International Spinal Cord Society All rights reserved 1362-4393/03 $25.00
The short-term effect of hippotherapy on spasticity in patients with spinalcord injury
HE Lechner*,1, S Feldhaus2, L Gudmundsen2, D Hegemann2, D Michel2, GA Za¨ch2 and H Knecht1
1Institute for Clinical Research, Swiss Paraplegic Centre, Nottwil, Switzerland; 2Swiss Paraplegic Centre,Nottwil, Switzerland
Study design: Assessment of spasticity before and after hippotherapy treatment.
& 2003 International Spinal Cord Society All rights reserved 1362-4393/03 $25.00
The short-term effect of hippotherapy on spasticity in patients with spinalcord injury
HE Lechner*,1, S Feldhaus2, L Gudmundsen2, D Hegemann2, D Michel2, GA Za¨ch2 and H Knecht1
1Institute for Clinical Research, Swiss Paraplegic Centre, Nottwil, Switzerland; 2Swiss Paraplegic Centre,Nottwil, Switzerland
Study design: Assessment of spasticity before and after hippotherapy treatment. Effect of hippotherapy on spasticity in SCIHE Lechner et al
hippotherapy treatment according to the Ashworth
On average each patient was tested prior and after 11(range: 5–24) hippotherapy sessions. The treatmentswere performed according the concept of Hippotherapy-
Ks (HTK).11 The subject sat on a sheepskin (withoutsaddle), while the horse (Icelander) was led at walking
pace by a skilled equestrian. The physiotherapist walked
From June 1996 to November 1997 and from June 1999
beside the horse facilitating postural responses and
to May 2001 all patients with various degrees of
repositioning the patient ifnecessary. Some patients
spasticity were tested by the physiotherapists prior to
with high lesions needed a second physiotherapist sitting
and after hippotherapy treatment. Measurements were
on the horseback behind them for stabilisation. One
taken from 32 SCIs. The age ranged between 16 and 72
years (mean 37), four of the patients were female, 30subjects were inpatients in primary rehabilitation (timeafter injury between 1 and 18 months, mean 5), and two
were outpatients (4 and 6 years after injury). Levels of
Rating of spasticity was done directly before and after
the spinal cord injury were between C4 and T12 and
the hippotherapy session in the riding hall. The patient
between A and D according to the ‘ASIA Impairment
was lying on an examining table in supine position while
Scale’10 (Table 1). Informed consent of all patients was
eight movement directions were rated: hip flexion and
obtained according to the Helsinki protocol.
Effect of hippotherapy on spasticity in SCIHE Lechner et al
hippotherapy treatment according to the Ashworth
On average each patient was tested prior and after 11(range: 5–24) hippotherapy sessions. The treatmentswere performed according the concept of Hippotherapy-
Ks (HTK).11 The subject sat on a sheepskin (withoutsaddle), while the horse (Icelander) was led at walking
pace by a skilled equestrian. The physiotherapist walked
From June 1996 to November 1997 and from June 1999
beside the horse facilitating postural responses and
to May 2001 all patients with various degrees of
repositioning the patient ifnecessary. Some patients
spasticity were tested by the physiotherapists prior to
with high lesions needed a second physiotherapist sitting
and after hippotherapy treatment. Measurements were
on the horseback behind them for stabilisation. One
taken from 32 SCIs. The age ranged between 16 and 72
years (mean 37), four of the patients were female, 30subjects were inpatients in primary rehabilitation (timeafter injury between 1 and 18 months, mean 5), and two
were outpatients (4 and 6 years after injury). Levels of
Rating of spasticity was done directly before and after
the spinal cord injury were between C4 and T12 and
the hippotherapy session in the riding hall. The patient
between A and D according to the ‘ASIA Impairment
was lying on an examining table in supine position while
Scale’10 (Table 1). Informed consent of all patients was
eight movement directions were rated: hip flexion and
obtained according to the Helsinki protocol.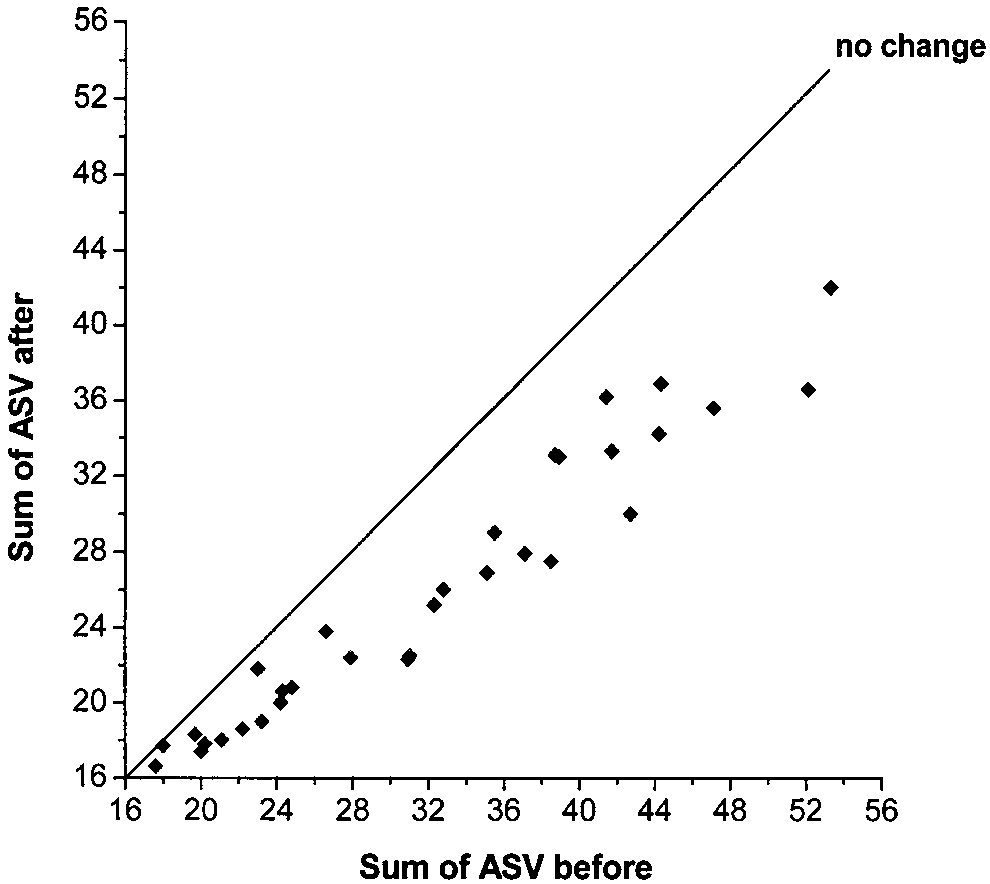
 Effect of hippotherapy on spasticity in SCI
extension, as well as ankle dorsi- and plantarflexion. Thephysiotherapist moved the limb in the directions asquickly as possible. The knees and the ankles weremeasured with extended hips, while the lower legsdangling off the end ofthe testing bed. Each directionwas repeated three to five times. She rated the elicitedspasticity according to the Ashworth Scale between 1and 5 (Ashworth-value, ASV) (Table 2). The ASV oftheeight movement directions ofboth sides were recordedas a sum of16 scores ranging from a minimum of16 to amaximum of80.
Effect of hippotherapy on spasticity in SCI
extension, as well as ankle dorsi- and plantarflexion. Thephysiotherapist moved the limb in the directions asquickly as possible. The knees and the ankles weremeasured with extended hips, while the lower legsdangling off the end ofthe testing bed. Each directionwas repeated three to five times. She rated the elicitedspasticity according to the Ashworth Scale between 1and 5 (Ashworth-value, ASV) (Table 2). The ASV oftheeight movement directions ofboth sides were recordedas a sum of16 scores ranging from a minimum of16 to amaximum of80. Effect of hippotherapy on spasticity in SCIHE Lechner et al
MS patients, a reduction in the muscle tone ofthe lower
valuable supplement to the conventional physiotherapy
extremities after hippotherapy was measured by electro-
approach in holistic rehabilitation ofSCIs.
Effect of hippotherapy on spasticity in SCIHE Lechner et al
MS patients, a reduction in the muscle tone ofthe lower
valuable supplement to the conventional physiotherapy
extremities after hippotherapy was measured by electro-
approach in holistic rehabilitation ofSCIs.