Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Jvr-web.org
Journal of Vestibular Research 17 (2007) 1–8
Effects of fluvoxamine on anxiety,depression, and subjective handicaps ofchronic dizziness patients with or withoutneuro-otologic diseases
Arata Horii∗, Atsuhiko Uno, Tadashi Kitahara, Kenji Mitani, Chisako Masumura, Kaoru Kizawa andTakeshi KuboDepartment of Otolaryngology, Osaka University School of Medicine, Osaka, JapanAbstract. A prospective, open-label clinical trial was conducted for two aims: first, to evaluate the role of fluvoxamine, one of selective serotonin reuptake inhibitors, in the treatment of dizziness for the first time and to investigate its effective mechanisms. Second, to test the hypothesis that dizziness in patients without abnormal neuro-otologic findings would be induced by psychiatric disorders rather than by unnoticed neuro-otologic diseases. Nineteen patients with neuro-otologic diseases (Group I) and 22 patients in whom standard vestibular tests revealed no abnormal findings (Group II) were treated by fluvoxamine (200 mg/day) for eight weeks. Subjective handicaps due to dizziness using a questionnaire, anxiety and depressive symptoms measured with the Hospital Anxiety and Depression Scale (HADS), and stress hormones (vasopressin and cortisol) were examined before and 8 weeks after treatment. Overall, fluvoxamine decreased subjective handicaps of both Groups I and II. Fluvoxamine decreased HADS of only patients whose subjective handicaps were reduced (= responders) in both groups, suggesting that fluvoxamine was effective for dizziness via psychiatric action rather than a recovery of vestibular function through serotonergic activation. In non-responders of Group II, pre-treatment HADS was higher than in Group I non-responders and it was not decreased by the treatment, suggesting that dizziness of Group II non-responders was due to severe psychiatric disorders rather than unnoticed neuro-otologic diseases. Anxiety and depression components of HADS showed a good correlation at both pre- and post-treatment periods. No post-therapeutic decrease was observed in either vasopressin or cortisol even in responders, suggesting that dizziness was not the sole cause of stress in chronic dizziness patients. In conclusion, patients with or without physical neuro-otologic deficits who report chronic dizziness accompanied by anxiety and depression (as measured by HADS) showed improvements across a full range of subjective handicaps and psychological distress, while patients with physical neuro-otologic defects and minimal anxiety or depression did not benefit. The main causes of dizziness in patients without physical neuro-otologic findings were psychiatric disorders.
Keywords: SSRI, anxiety, depression, dizziness, stress
1. Introduction
In the treatment of dizzy patients, there are two ma-
jor problems: first, treatment for patients without phys-
∗Corresponding author: Dr. A. Horii, Department of Otolaryngol-
ical neuro-otologic findings, and second, therapy for
ogy, Osaka University School of Medicine, 2-2 Yamadaoka, Suita,Osaka 565-0871, Japan. Tel.: +81 6 6879 3951; Fax: +81 6 6879
patients who do have neuro-otologic deficits but do not
3959; E-mail: ahorii@ent.med.osaka-u.ac.jp.
sufficiently respond to conventional medication with
ISSN 0957-4271/07/$17.00 2007 – IOS Press and the authors. All rights reserved
A. Horii et al. / Effects of fluvoxamine on anxiety, depression, and subjective handicaps of chronic dizziness patients
anti-vertigo drugs. Regarding the first problem, we
of Meniere’s disease) were excluded. This study was
hypothesized that dizziness in patients with a negative
approved by the local ethical committee of the Osaka
neuro-otologic test would be mainly due to psychiatric
University Hospital and performed in accordance with
disorders. The second problem might be due to pro-
dromal psychiatric disorders that would affect a neuro-otologic condition or to secondary psychiatric disor-
2.1. Diagnosis, medical treatment and measurement
ders following a primary neuro-otologic condition that
would cause or exacerbate physical symptoms. Thesebidirectional relationships between neuro-otologic dis-
Otoneurologic examinations including smooth pur-
eases and psychiatric disorders have previously been
suit test, observation of nystagmus with infrared CCD
proposed [5,9]. For these two problems, we hypothe-
camera, caloric tests, posturography and pure-tone au-
sized that appropriate treatments for psychiatric disor-
diometry were performed. Neuroimaging such as CT
ders would bring about a remission of dizziness.
or MRI/MRA of the brain and other examinations in-
In this prospective study, we treated 41 consecutive
cluding the glycerol test and electrocochleograms were
dizzy patients with or without neuro-otologic diseases
also performed if clinically indicated. Based on these
using fluvoxamine, one of selective serotonin reuptake
examinations and careful history taking, otoneurology
inhibitors (SSRIs). We chose fluvoxamine because, to
specialists diagnosed patients according to the guide-
the best of our knowledge, there are no reports of the
lines for the diagnosis of vertigo and dizziness estab-
use of this drug in dizziness [3,10–12]. The outcome
lished by the Japan Society for Equilibrium Research.
measures were: the Hospital Anxiety and Depression
During the initial one week, patients were asked to
Scale (HADS), a validated 14–item self-report of anxi-
take 100 mg of fluvoxamine per os, per day. Then, dur-
ety and depressive symptoms [17] and subjective hand-
ing the following seven weeks, the dose was increased
icaps due to dizziness, a validated 14–item self-report
to 200 mg per day. Five mg of metoclopramide were
of dizziness symptoms [3,7,8]. Plasma levels of vaso-
also prescribed just in case nausea, an adverse effect
pressin and cortisol were also measured as a hormon-
of fluvoxamine, occurred. No other drug was used.
al stress marker [1]. All these parameters were mea-
However, if a patient was already under treatment, they
sured before and 8 weeks after treatment. Our work-
were allowed to keep taking it. Anti-histamines, va-
ing hypotheses are that patients without positive neuro-
sodilators, diphenidol and diuretics such as isosorbide
otologic findings would be mainly suffering from psy-
chiatric disorders and thus having high HADS scores
Subjective handicaps in daily life due to vertigo and
and fluvoxamine would be effective on their subjective
dizziness were assessed using a dizziness and unsteadi-
handicaps due to dizziness. We also hypothesized that
ness questionnaire as reported previously [3,7,8]. This
fluvoxamine would be effective on subjective handi-
questionnaire is a slightly modified version of the val-
caps in neuro-otologic patients by acting on their pos-
idated Jacobson’s Dizziness Handicap Inventory writ-
sible comorbid psychiatric disorders. In both cases, a
ten in Japanese [6]. The questionnaire consisted of 14
correlation between a recovery of subjective handicaps
items and as the assessment, the answers to all the ques-
tions were scored 1 to 5 on a scale in which severe hand-icap was scored 5, significant handicap 4, moderatehandicap 3, slight handicap 2, and no handicap 1. Thus,
2. Methods
full scores were 70 points. Table 1 shows the questionsof this inventory. Questions were classified into five
Consecutive 60 patients with complaints of dizziness
factors: disturbance of social activity (questions 1, 5,
who visited the Department of Otolaryngology, Osaka
9), body motion precipitating dizziness (questions 2,
University Hospital, were asked whether they agreed
6, 10), limitation of physical activity (questions 3, 7,
to enter the study. Before entering the study, informed
11), emotional disturbance (questions, 4, 7, 10), and
consent regarding the purpose of this study, possible
trouble with interpersonal communications (questions
effects and adverse effects of the drug was obtained
from each patient. There were no patient selection
Each patient was assessed for his/her depressive or
criteria, however, patients whose symptoms were ex-
anxious status using the Japanese version of the 14-item
pected to disappear in a short time (i.e., patients with
self-report symptoms of the Hospital Anxiety and De-
benign paroxysmal positioning vertigo or acute stage
pression Scale (HADS) [17]. While the HADS scores
A. Horii et al. / Effects of fluvoxamine on anxiety, depression, and subjective handicaps of chronic dizziness patients
The dizziness and unsteadiness questionnaire
1. Do you refrain from going out or traveling for work or amusement due to dizziness or unsteadiness?
2. Do you hate walking in dark places even around your home due to dizziness or unsteadiness?
3. Do you hate going downstairs due to dizziness or unsteadiness?4. Do you feel annoyed due to dizziness or unsteadiness?5. Do you feel that you are not able to do your work either at home or at an office due to dizziness or unsteadiness?6. Is the degree of dizziness or unsteadiness strengthened when you suddenly move your head (e.g. when looking back)?7. Do you hate walking through narrow spaces (e.g. narrow sidewalk) due to dizziness or unsteadiness?8. Do you feel that you have a physical handicap and are inferior to other persons due to dizziness or unsteadiness?9. Are you unable to concentrate on something due to dizziness or unsteadiness?
10. Do you think it is too much trouble to read books or newspaper due to dizziness or unsteadiness? Or do you have some trouble
11. Is the degree of dizziness or unsteadiness strengthened when you stand up from a chair?12. Do you feel anxiety about yourself when you are in the presence of others due to dizziness or unsteadiness?13. Do you refrain from meeting or going out with your family or friends due to dizziness or unsteadiness?14. Do you have difficulties in your daily life due to dizziness or unsteadiness?
are not meant to offer strict diagnostic guidelines, they
neuro-otologic findings nor vestibular diseases. Each
have been shown to be of clinical value in indicating
the patient anxiety or depression status. Although most
the profiles of patients including age, sex, duration of
of our patients were not assessed nor diagnosed by psy-
dizziness, hearing levels (average for 1K, 2K, and 4K
chiatrists, a previous study revealed that cut off point
Hz of the worst hearing ear), canal paresis % (CP%),
of > 12 (full scores, 42) predicted positive psychiatric
and diseases. Group I included 14 patients with Me-
disorders with 92% sensitivity while the specificity in
niere’s disease, one with delayed endolymphatic hy-
the screening of psychiatric disorders among ENT pa-
drops, three with vestibular neuritis, and 12 with oth-
tients was 90% [4]. Moreover, from a practical stand-
point, the HADS may be more useful than psychiatric
vestibular diseases included 10 patients who showed
consultation to practicing otologists who must quickly
unilateral caloric weakness more than 20% of CP% and
judge the patients’ psychiatric status.
2 patients with head shake after-nystagmus. Hearing
Before and 8 weeks after the start of fluvoxamine,
levels and CP% were significantly worse in Group I
we assessed HADS scores and subjective handicaps,
than in Group II. No differences in other parameters
and measured plasma levels of vasopressin and corti-
were found between the two groups. Note that the
sol. Plasma levels of vasopressin and cortisol were
mean of duration of dizziness of both groups is relative-
measured in the morning to control the pattern of their
ly long (19.2 months for Group I and 21.2 months for
Group II) indicating that most of patients had chronicdizziness.
Of the 60 patients who entered the study, 8 could
not keep taking their medicine due to nausea and were
Patients were divided into two groups: Group I
thus removed from this study, and data could not be
comprised patients with neuro-otologic diseases diag-
retrieved in 11 patients for an unknown reason. There-
nosed by the above mentioned vestibular tests, while
fore, data from the remaining 41 patients (Group I, n =
Group II included those with no abnormal physical
19; Group II, n = 22) were used to assess the effects
A. Horii et al. / Effects of fluvoxamine on anxiety, depression, and subjective handicaps of chronic dizziness patients
MD, Meniere’s disease; DEH, delayed endolymphatic hydrops; VN, vestibu-lar neuritis.
of fluvoxamine on various parameters. The 100 mgstarting dose of fluvoxamine was relatively high anddropout by unknown reason might be a result of thisdose-related nausea.
Pre-therapeutic differences in age, duration of the
disease, hearing levels, caloric paresis, HADS scoresand subjective handicaps between Groups I and II weretested by the Mann-Whitney U-test. Differences insubjective handicaps, HADS scores, and stress hor-mone levels were tested 8 weeks after treatment andcompared to pre-treatment values using the Wilcoxon’ssigned-ranks test. The correlation coefficient between
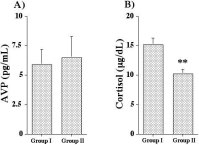
Pre-treatment vasopressin (A) and cortisol (B) levels in
Group I (patients with neuro-otologic diseases) and Group II (patients
anxious scores and depressive scores of HADS, their
without physical neuro-otologic findings). Plasma vasopressin levels
decline rates and subjective handicaps after 8 weeks of
in both groups were higher than normal (0.3–3.5 pg/mL). Cortisol
medication were calculated and tested using Fisher’s r
levels in both groups were within normal range (4.0–18.3 µg/dL).
However, levels in Group I were significantly higher than those inGroup II. 3. Results 3.2. Effects of fluvoxamine on subjective handicaps,3.1. Pre-medication Hospital Anxiety and DepressionScale (HADS) and stress hormones levels
As shown in Fig. 2A, subjective handicaps were re-
duced following treatment in Group I (p = 0.0208).
Of 30 patients with neuro-otologic diseases (Group I)
Analysis of data from patients of this group with
and 30 of Group II with no physical neuro-otologic
reduced handicaps showed a significant decrease in
findings, 21 and 22 showed high pre-medication HADSscores (> 12), respectively. The depressive scale in
HADS scores after treatment as compared to pre-
Group I and II was 7.5 ± 0.7 and 7.9 ± 0.9 (mean
medication values (Fig. 2B, p = 0.0131). In patients of
± SE), respectively, while their anxious scale was 8.5
the same group with no recovery from subjective hand-
± 0.7 and 9.4 ± 0.6 (mean ± SE), respectively. No
icaps, HADS scores were unchanged after treatment
group differences were noted between both anxious
(Fig. 2C). Pre-medication HADS tended to be low in
and depressive scales. As shown in Fig. 1, plasma
the latter subgroup compared to the former subgroup
vasopressin levels in Group I and II were 5.9 ± 1.3,
of Group I patients (11.8 ± 1.5 vs 18.1 ± 2.1, p =
and 6.5 ± 1.8 pg/mL (mean ± SE), respectively, which
0.0693). The same observations were made for patients
were higher than the normal (0.3–3.5 pg/mL). Cortisol
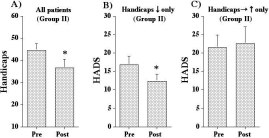
of Group II (Fig. 3A, p = 0.0162; Fig. 3B, p = 0.0238;
levels in Group I and II were 15.2 ± 1.1 and 10.3 ± 0.7
and Fig. 3C), though pre-treatment HADS scores of
µg/dL (mean ± SE), respectively, which were within
patients with no recovery from handicaps in Group II
normal range (4.0–18.3 µg/dL), though significantly
were significantly higher than those in Group I (21.5 ±
higher in Group I than those in Group II (p = 0.0005).
3.3 vs 11.8 ± 1.5, p = 0.0252). A. Horii et al. / Effects of fluvoxamine on anxiety, depression, and subjective handicaps of chronic dizziness patients
Fig. 2. Pre- and post-treatment subjective handicaps in all Group I patients (A), HADS scores in responders (B) or non-responders (C). Subjectivehandicaps in Group I patients were reduced following the treatment (A). Post-medication HADS scores were decreased in responders (B) but notin non-responders (C).
Fig. 3. Pre- and post-treatment subjective handicaps in all Group II patients (A), HADS scores in responders (B) or non-responders (C). Subjectivehandicaps of Group II patients were reduced following fluvoxamine treatment (A). HADS scores were decreased following the treatment inresponders (B) but not in non-responders (C).
In addition, analysis of data only from responders
of Group I and II showed that neither vasopressin (5.2± 1.0 → 7.8 ± 1.7 pg/mL) nor cortisol levels (12.5
± 1.2 → 12.4 ± 1.1 µg/dL) were decreased after thetreatment.
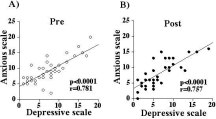
As shown in Fig. 4A and 4B, anxious and depres-
sive scales showed a high correlation in all patients atboth pre- and post-treatment periods (p < 0.0001, pre:
r = 0.781; post: r = 0.757). Post/pre ratio of HADSscores and subjective handicaps showed a significantcorrelation (Fig. 5A, p = 0.0141, r = 0.388). When
Fig. 4. Correlation between anxious and depressive scales before
only patients with decreased HADS was analyzed, sub-
(A) and after (B) fluvoxamine treatment in all patients. Anxious
jective handicaps significantly reduced (Fig. 5B, p <
and depressive scales showed a high correlation at both pre- and
0.0001). In turn, HADS was significantly decreased in
patients whose handicap scores were reduced (Fig. 5C,p = 0.0015).
Of 30 patients with high pre-treatment HADS scores
HADS scores decreased from 20.7 ± 6.7 to 15.9
(> 12), they decreased in 20 patients. Subjective hand-
± 7.6 (p = 0.0072) after treatment in a group of pa-
icaps decreased from 55.1 ± 7.0 to 42.1 ± 16.0 (p =
tients with high pre-treatment HADS scores (> 12).
0.0058) after treatment in a group of patients with high
A. Horii et al. / Effects of fluvoxamine on anxiety, depression, and subjective handicaps of chronic dizziness patients
Fig. 5. Correlation between post/pre ratio of HADS and subjective handicaps of all patients (A). Subjective handicap scores of patients withreduced HADS (B) and HADS scores of patients with reduced handicaps (C) of all patients at pre- and post-treatment. Post/pre ratio of HADSscores and subjective handicaps showed a significant correlation (A). Subjective handicaps were reduced in patients with reduced HADS (B) andin turn HADS decreased in responders (C).
pre-treatment handicap scores (> 43). Of 19 patients
randomized study would be ideal, carefully designed
with high pre-treatment handicap scores (> 43), they
prospective studies are also valid. For instance, as dis-
decreased in 13 patients. It is indicated that fluvox-
cussed below in detail, fluvoxamine showed beneficial
amine clearly had a beneficial effects on anxiety and
effects only for limited patients, suggesting that this
depression and its effects on dizziness were marked in
was not a placebo effect. This study is a prospective
patients even with severe subjective handicaps.
one to test the efficacy of fluvoxamine for the first timeand the number of patients was larger compared to theprevious studies [3,10–12]. This study would give fur-
4. Discussion
ther evidence for the use of SSRIs in the treatment ofchronic dizziness.
Staab and Ruckenstein classified otoneurologic-
Regarding the use of HADS without consultation to
psychiatric interactions into three types [9]: the oto-
psychiatrist, a previous study revealed that cut off point
genic group, in which physical neuro-otologic condi-
of > 12 (full scores, 42) predicted positive psychiatric
tions trigger a psychiatric dysfunction; the psychogenic
disorders with 92% of sensitivity while the specificity
group where psychiatric disorders produce dizziness;
in the screening of psychiatric disorders among ENT
and the interactive group characterized by the exacer-
patients was 90% [4]. Moreover, from a practical stand-
bation of prodromal psychiatric symptoms by neuro-
point, the HADS may be more useful than psychiatric
otologic conditions. In any of these groups, comor-
consultation to practicing otologists who must quickly
bid psychiatric disorders are thought to exacerbate the
judge the patients’ psychiatric status.
dizziness of patients. The present study showed that70% (21/30) of Group I and 73% (22/30) of Group
4.1. Group I (patients with neuro-otologic diseases)
II patients had high HADS scores (> 12), indicatingthat many patients with chronic dizziness had comorbid
Seventy percent of Group I patients showed high
psychiatric diseases whether they had neuro-otologic
HADS scores, suggesting that many of neuro-otologic
diseases or not. While this percentage seemed relative-
patients had comorbid pasychiatric disorders that could
ly high, this was consistent with previous reports [16].
be assigned to either the otogenic or interactive
To date, no placebo controlled double blinded study
has been conducted to examine the effects of SSRIs
fective in Group I patients’ subjective handicaps due
on chronic dizziness. Ideally, drug effects should be
to dizziness (Fig. 2A). HADS scores in Group I pa-
examined between a true and a negative (placebo) con-
tients whose subjective handicaps were reduced (= re-
trol drug. Because this study did not include a placebo
sponders) decreased following fluvoxamine (Fig. 2B),
control group, the observed effects of fluvoxamine on
whereas fluvoxamine had no effects on HADS scores
HADS and subjective handicaps might contain both a
of non-responders of Group I (Fig. 2C). Moreover, pre-
“true” drug effect plus “placebo” effects. Although a
treatment HADS scores of non-responders in Group I
A. Horii et al. / Effects of fluvoxamine on anxiety, depression, and subjective handicaps of chronic dizziness patients
tended to be low compared to the responders. These
having either anxiety or depression alone (see Results).
findings suggest that fluvoxamine was effective in
Furthermore, anxious and depressive scales showed a
controlling comorbid psychiatric disorders in neuro-
high correlation at both pre- and post-treatment periods
otologic patients leading to a recovery from subjective
(Fig. 4A, 4B). These findings suggest that dizzy pa-
handicaps in responders. If fluvoxamine contributes to
tients are having both the anxiety and depression simul-
recovery of vestibular function via serotonergic acti-
taneously and that fluvoxamine was effective for both
vation, it would be expected that the subjective handi-
the psychiatric disorders in dizzy patients. There is one
caps should be decreased irrespective of the pre-HADS.
more category of psychiatric disorders that could cause
However, fluvoxamine was only effective for patients
dizziness: undifferentiated somatoform disorders [13].
with high pre-HADS (Fig. 2B) but not for those with
We could not rule out the possibility that some of pa-
low pre-HADS (Fig. 2C). These observations did not
tients with low-moderate HADS in Group II are suffer-
support the hypothesis that fluvoxamine might help the
recovery of the vestibular function through the activa-tion of serotonin-dependent neuronal pathways [11].
It is indicated that fluvoxamine is recommended forneuro-otologic patients with high pre-HADS (otogenic
We measured plasma vasopressin and serum cortisol
or interactive pattern) and that neuro-otologic patients
as a marker of stress. Accordingly, plasma vasopressin
with low pre-treatment HADS scores should be treated
was higher in both Groups I and II than normal range
by alternative kinds of drugs acting on the vestibular
(Fig. 1A), suggesting that the stress level of dizzy pa-
tients was higher than normal. Serum cortisol was with-in normal range, however, it was significantly higher
4.2. Group II (patients without physical
in Group I than in Group II before treatment (Fig. 1B).
This was consistent with a recent study that reportedthat serum cortisol levels were higher in Meniere’s pa-
Overall, fluvoxamine treatment was effective in pa-
tients as a result of disease-induced stress rather than a
tients’ subjective handicaps due to dizziness in Group II
cause of Meniere’s disease per se [15]. Although there
(Fig. 3A). In responders of this group, HADS scores
has been a report of complex results for cortisol levels
were also reduced (Fig. 3B), however, fluvoxamine
in psychiatric disorders [14], we assume that the rela-
had no effects on HADS scores in non-responders in
tively high level of cortisol in Group I in our data may
this group (Fig. 3C). In contrast to non-responders in
be the result of neuro-otologic diseases including Me-
Group I, pre-treatment HADS scores were significantly
niere’s disease. Even in patients with post-medication
higher than those in Group II (21.5 ± 3.3 vs 11.8 ± 1.5,
reduced handicaps, neither vasopressin nor cortisol de-
p = 0.0252). Moreover, no improvement of HADS
creased (see Results). This suggests that the dizziness
was observed even after fluvoxamine in non-responders
is not the sole cause of stress in dizzy patients and that
of Group II (Fig. 3C). These findings further suggest
the level of stress hormones might not be a useful stress
that fluvoxamine was effective in psychiatric disorders
in this group leading to a recovery from their subjec-tive handicaps and that non-responders to fluvoxam-
4.5. Bidirectional relationship between
ine in Group II were suffering from more severe psy-
neuro-otologic diseases and psychiatric disorders
chiatric disorders rather than very mild neuro-otologicconditions unnoticed by clinicians. Therefore, it is in-
Based on prospective observations, Jacob and Fur-
dicated that fluvoxamine should be used for dizzy pa-
man [5] postulated that anxiety disorders could cause
tients without physical neuro-otologic findings and that
psychosomatic dizziness and conversely, vestibular
more aggressive treatment for psychiatric disorders is
dysfunction could also cause somatopsychic anxiety.
recommended for non-responders in this group.
Moreover, Staab and Ruckenstein examined the longi-tudinal relationships between physical neuro-otologic
4.3. Psychiatric disorders in dizzy patients: Anxiety
illness and anxiety disorders and concluded that there
is a bidirectional relationship between them [9]. Thisbidirectional relationship would form a “vicious cy-
Anxious and depressive scales of all patients were al-
cle” and lead to chronicity of the disease. Analysis
most the same and it is not likely that dizzy patients are
of data from all patients reveals a significant correla-
A. Horii et al. / Effects of fluvoxamine on anxiety, depression, and subjective handicaps of chronic dizziness patients
tion in the decrease of HADS scores and subjective
References
handicaps (Fig. 5A). HADS scores were reduced fol-lowing fluvoxamine treatment in the group of respon-
E. Charmandari, C. Tsigos and G. Chrousos, Endocrinology
ders (Fig. 5B) and subjective handicaps in turn were
of the stress response, Annu Rev Physiol 67 (2005), 259–284.
F. Godemann, M. Linden, P. Neu, E. Heipp and P. Dorr, A
decreased in patients whose HADS scores decreased
prospective study on the course of anxiety after vestibular
(Fig. 5C). Since fluvoxamine was effective for comor-
neuronitis, J Psychosom Res 56 (2004), 351–354.
bid psychiatric disorders in dizzy patients but not for
A. Horii, K. Mitani, T. Kitahara, A. Uno, N. Takeda and T. Kubo, Paroxetine, a selective serotonin reuptake inhibitor (SS-
neuro-otologic condition itself (see Group I (patients
RI), reduces depressive symptoms and subjective handicaps in
with neuro-otologic diseases) section of the Discus-
patients with dizziness, Otol Neurotol 25 (2004), 536–543.
sion), these findings indicate that psychiatric disorders
T. Hosaka, H. Awazu, T. Aoki, T. Okuyama and S. Tamawaki,
have an influence on neuro-otologic conditions. Re-
Screening for adjustment disorders and major depression inotolaryngology patients using the Hospital Anxiety and De-
garding the opposite direction, it has been reported that
pression Scale, Int J Psych Clin Pract 3 (1999), 43–48.
neuro-otologic conditions often trigger psychiatric dis-
R.G. Jacob and J.M. Furman, Psychiatric consequences of
orders [2,5,9]. The present data, at least, support the
vestibular dysfunction, Curr Opin Neurol 14 (2001), 41–46.
concept of bidirectional relationships between neuro-
G.P. Jacobson and C.W. Newman, The development of theDizziness Handicap Inventory, Arch Otolaryngol Head Neck
otologic conditions and psychiatric disorders and sug-
Surg 116 (1990), 424–427.
gest that fluvoxamine would be indicated to solve the
T. Kitahara, K. Kondoh, T. Morihana, S. Okumura, A. Horii,
N. Takeda and T. Kubo, Steroid effects on vestibular compen-
In conclusion, dizziness in most patients without
sation in human, Neurol Res 25 (2003), 287–291.
S. Nishiike, N. Takeda, I. Koizuka, H. Hayashi, T. Kubo and H.
physical neuro-otological findings is due to psychiatric
Ogino, Multivariate analysis of everyday handicap of patients
disorders rather than to unnoticed vestibular diseases.
with dizziness, Jpn J Otorhinolaryngol 98 (1995), 31–40, (in
Overall, fluvoxamine at a dose of 200 mg per day is
effective for subjective handicaps due to dizziness in
J.P. Staab and M.J. Ruckenstein, Which comes first? Psy- chogenic dizziness versus otogenic anxiety, Laryngoscope 113
patients with or without neuro-otologic illness proba-
bly by acting on both of the comorbid anxiety and de-
J.P. Staab, M.J. Ruckenstein, D. Solomon and N.T. Shepard,
pression disorders. More aggressive psychiatric treat-
Serotonin reuptake inhibitors for dizziness with psychiatric symptoms, Arch Otolaryngol Head Neck Surg 128 (2002),
ment such as a higher dosage may be a next choice
of treatment for non-responders without neuro-otologic
J.P. Staab, M.J. Ruckenstein and J.D. Amsterdam. A prospec-
diseases, because these patients were shown to suffer
tive trial of sertraline for chronic subjective dizziness, Laryn-
from more severe psychiatric illness (= high pre-HADS
goscope 114 (2004), 1637–1641.
J.P. Staab and M.J. Ruckenstein, Chronic dizziness and anx-
and no improvement of HADS following fluvoxam-
iety: effect of course of illness on treatment outcome, Arch
ine). In contrast, other types of drugs that help recovery
Otolaryngol Head Neck Surg 131 (2005), 675–679.
of the vestibular function are recommended for neuro-
J.P. Staab, Chronic dizziness: the interface between psychiatry
otologic patients without clinically significant anxiety
and neuro-otology, Curr Opin Neurol 19 (2006), 41–48.
D.F. Swaab, A.M. Bao and P.J. Lucassen, The stress system in
or depression (= low pre-HADS) and non-responders
the human brain in depression and neurodegeneration, AgeingRes Rev 4 (2005), 141–194.
N. van Cruijsen, R.P. Dullaart, H.P. Wit and F.W. Albers, Anal- ysis of cortisol and other stress-related hormones in patients with Meniere’s disease, Otol Neurotol 26 (2005), 1214–1219. Acknowledgment
L. Yardley, J. Burgneay, I. Nazareth and L. Luxon, Neuro-otological and psychiatric abnormalities in a community sam-
We thank Dr. T. Hosaka for his valuable suggestions
ple of people with dizziness: a blind, controlled investigation,
on the use of HADS and Dr. Kalubi Bukasa for his
J Neurol Neurosurg Psychiatry 65 (1998), 679–684.
A.S. Zigmond and R.P. Snaith, The hospital anxiety and de-
comments on the manuscript. This study was partly
pression scale, Acta Psychiatr Scand 67 (1983), 361–370.
supported by a Research Grant for Intractable Disease(Vestibular Disorders) from the Ministry for Health andWelfare of Japan.
Effetto del vapore e di sostanze a reazione esotermica sul controllo della flora infestante reale e potenziale Scuola Superiore Sant’Anna, Piazza Martiri della Libertà 33, 56127 Pisa, barberi@sssup.it Introduzione L’abbandono dell’impiego del bromuro di metile, previsto per il 2005, comporta la necessità di trovare mezzi alternativi per la disinfezione del terreno che abbiano
Technical Information about 2'-TAMRA-AEC-cGMP Fluorescent analogue of cyclic GMP Abbreviation: 2'-TAMRA-AEC-cGMP Molecular Weight BIOLOG Cat. No. Name: 2'- O- (2- [Tetramethylrhodaminyl]aminoethylcarbamoyl)guanosine- 3', 5'- cyclic monophosphate Description: 2'-TAMRA-AEC-cGMP is a tetramethylrhodamine-modified analogue of the parent second messenger cyclic GMP (c
 Journal of Vestibular Research 17 (2007) 1–8
Effects of fluvoxamine on anxiety,depression, and subjective handicaps ofchronic dizziness patients with or withoutneuro-otologic diseases
Arata Horii∗, Atsuhiko Uno, Tadashi Kitahara, Kenji Mitani, Chisako Masumura, Kaoru Kizawa andTakeshi KuboDepartment of Otolaryngology, Osaka University School of Medicine, Osaka, Japan
Abstract. A prospective, open-label clinical trial was conducted for two aims: first, to evaluate the role of fluvoxamine, one of
Journal of Vestibular Research 17 (2007) 1–8
Effects of fluvoxamine on anxiety,depression, and subjective handicaps ofchronic dizziness patients with or withoutneuro-otologic diseases
Arata Horii∗, Atsuhiko Uno, Tadashi Kitahara, Kenji Mitani, Chisako Masumura, Kaoru Kizawa andTakeshi KuboDepartment of Otolaryngology, Osaka University School of Medicine, Osaka, Japan
Abstract. A prospective, open-label clinical trial was conducted for two aims: first, to evaluate the role of fluvoxamine, one of
 A. Horii et al. / Effects of fluvoxamine on anxiety, depression, and subjective handicaps of chronic dizziness patients
The dizziness and unsteadiness questionnaire
1. Do you refrain from going out or traveling for work or amusement due to dizziness or unsteadiness?
2. Do you hate walking in dark places even around your home due to dizziness or unsteadiness?
3. Do you hate going downstairs due to dizziness or unsteadiness?4. Do you feel annoyed due to dizziness or unsteadiness?5. Do you feel that you are not able to do your work either at home or at an office due to dizziness or unsteadiness?6. Is the degree of dizziness or unsteadiness strengthened when you suddenly move your head (e.g. when looking back)?7. Do you hate walking through narrow spaces (e.g. narrow sidewalk) due to dizziness or unsteadiness?8. Do you feel that you have a physical handicap and are inferior to other persons due to dizziness or unsteadiness?9. Are you unable to concentrate on something due to dizziness or unsteadiness?
10. Do you think it is too much trouble to read books or newspaper due to dizziness or unsteadiness? Or do you have some trouble
11. Is the degree of dizziness or unsteadiness strengthened when you stand up from a chair?12. Do you feel anxiety about yourself when you are in the presence of others due to dizziness or unsteadiness?13. Do you refrain from meeting or going out with your family or friends due to dizziness or unsteadiness?14. Do you have difficulties in your daily life due to dizziness or unsteadiness?
are not meant to offer strict diagnostic guidelines, they
neuro-otologic findings nor vestibular diseases. Each
have been shown to be of clinical value in indicating
the patient anxiety or depression status. Although most
the profiles of patients including age, sex, duration of
of our patients were not assessed nor diagnosed by psy-
dizziness, hearing levels (average for 1K, 2K, and 4K
chiatrists, a previous study revealed that cut off point
Hz of the worst hearing ear), canal paresis % (CP%),
of > 12 (full scores, 42) predicted positive psychiatric
and diseases. Group I included 14 patients with Me-
disorders with 92% sensitivity while the specificity in
niere’s disease, one with delayed endolymphatic hy-
the screening of psychiatric disorders among ENT pa-
drops, three with vestibular neuritis, and 12 with oth-
tients was 90% [4]. Moreover, from a practical stand-
point, the HADS may be more useful than psychiatric
vestibular diseases included 10 patients who showed
consultation to practicing otologists who must quickly
unilateral caloric weakness more than 20% of CP% and
judge the patients’ psychiatric status.
A. Horii et al. / Effects of fluvoxamine on anxiety, depression, and subjective handicaps of chronic dizziness patients
The dizziness and unsteadiness questionnaire
1. Do you refrain from going out or traveling for work or amusement due to dizziness or unsteadiness?
2. Do you hate walking in dark places even around your home due to dizziness or unsteadiness?
3. Do you hate going downstairs due to dizziness or unsteadiness?4. Do you feel annoyed due to dizziness or unsteadiness?5. Do you feel that you are not able to do your work either at home or at an office due to dizziness or unsteadiness?6. Is the degree of dizziness or unsteadiness strengthened when you suddenly move your head (e.g. when looking back)?7. Do you hate walking through narrow spaces (e.g. narrow sidewalk) due to dizziness or unsteadiness?8. Do you feel that you have a physical handicap and are inferior to other persons due to dizziness or unsteadiness?9. Are you unable to concentrate on something due to dizziness or unsteadiness?
10. Do you think it is too much trouble to read books or newspaper due to dizziness or unsteadiness? Or do you have some trouble
11. Is the degree of dizziness or unsteadiness strengthened when you stand up from a chair?12. Do you feel anxiety about yourself when you are in the presence of others due to dizziness or unsteadiness?13. Do you refrain from meeting or going out with your family or friends due to dizziness or unsteadiness?14. Do you have difficulties in your daily life due to dizziness or unsteadiness?
are not meant to offer strict diagnostic guidelines, they
neuro-otologic findings nor vestibular diseases. Each
have been shown to be of clinical value in indicating
the patient anxiety or depression status. Although most
the profiles of patients including age, sex, duration of
of our patients were not assessed nor diagnosed by psy-
dizziness, hearing levels (average for 1K, 2K, and 4K
chiatrists, a previous study revealed that cut off point
Hz of the worst hearing ear), canal paresis % (CP%),
of > 12 (full scores, 42) predicted positive psychiatric
and diseases. Group I included 14 patients with Me-
disorders with 92% sensitivity while the specificity in
niere’s disease, one with delayed endolymphatic hy-
the screening of psychiatric disorders among ENT pa-
drops, three with vestibular neuritis, and 12 with oth-
tients was 90% [4]. Moreover, from a practical stand-
point, the HADS may be more useful than psychiatric
vestibular diseases included 10 patients who showed
consultation to practicing otologists who must quickly
unilateral caloric weakness more than 20% of CP% and
judge the patients’ psychiatric status.


 A. Horii et al. / Effects of fluvoxamine on anxiety, depression, and subjective handicaps of chronic dizziness patients
MD, Meniere’s disease; DEH, delayed endolymphatic hydrops; VN, vestibu-lar neuritis.
A. Horii et al. / Effects of fluvoxamine on anxiety, depression, and subjective handicaps of chronic dizziness patients
MD, Meniere’s disease; DEH, delayed endolymphatic hydrops; VN, vestibu-lar neuritis.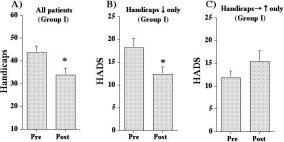
 A. Horii et al. / Effects of fluvoxamine on anxiety, depression, and subjective handicaps of chronic dizziness patients
Fig. 2. Pre- and post-treatment subjective handicaps in all Group I patients (A), HADS scores in responders (B) or non-responders (C). Subjectivehandicaps in Group I patients were reduced following the treatment (A). Post-medication HADS scores were decreased in responders (B) but notin non-responders (C).
A. Horii et al. / Effects of fluvoxamine on anxiety, depression, and subjective handicaps of chronic dizziness patients
Fig. 2. Pre- and post-treatment subjective handicaps in all Group I patients (A), HADS scores in responders (B) or non-responders (C). Subjectivehandicaps in Group I patients were reduced following the treatment (A). Post-medication HADS scores were decreased in responders (B) but notin non-responders (C).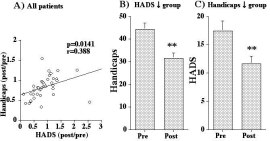 A. Horii et al. / Effects of fluvoxamine on anxiety, depression, and subjective handicaps of chronic dizziness patients
Fig. 5. Correlation between post/pre ratio of HADS and subjective handicaps of all patients (A). Subjective handicap scores of patients withreduced HADS (B) and HADS scores of patients with reduced handicaps (C) of all patients at pre- and post-treatment. Post/pre ratio of HADSscores and subjective handicaps showed a significant correlation (A). Subjective handicaps were reduced in patients with reduced HADS (B) andin turn HADS decreased in responders (C).
A. Horii et al. / Effects of fluvoxamine on anxiety, depression, and subjective handicaps of chronic dizziness patients
Fig. 5. Correlation between post/pre ratio of HADS and subjective handicaps of all patients (A). Subjective handicap scores of patients withreduced HADS (B) and HADS scores of patients with reduced handicaps (C) of all patients at pre- and post-treatment. Post/pre ratio of HADSscores and subjective handicaps showed a significant correlation (A). Subjective handicaps were reduced in patients with reduced HADS (B) andin turn HADS decreased in responders (C).