Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
V3n1doc
NEUMOSUR: REVISTA DE LA ASOCIACIÓN DE NEUMÓLOGOS DEL SUR VOL.3, NUMERO 1, ABRIL 1991
PLEURODESIS IN MALIGNANT PLEURAL EFFUSION WITH SPECIAL EMPHASIS ON TETRACYCLINE AS THE SCLEROSING AGENT
K. Viskum. Department of Pulmonary Medicine. Bispebjerg Hospital. Copenhagen. Denmark.
INTRODUCTION
Treatment intended to obliterate the pleural space has been in use since introduced in the operative treatment
of tuberculosis by Bethume in 1935(1). It has since been used Observation widely in the treatment of pneumothorax
and pleural effusion due to malignant disease.
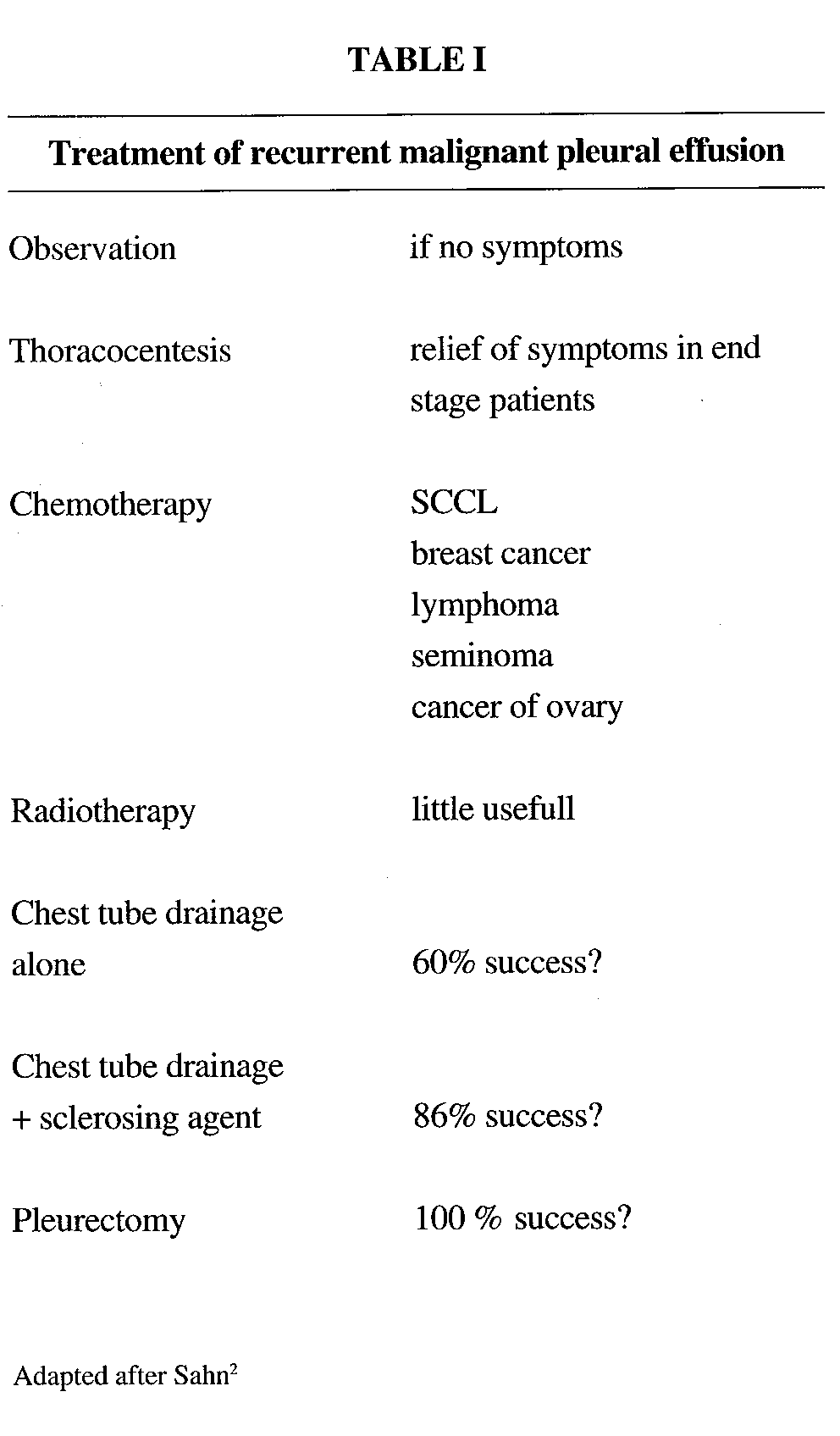
Repeated thoracocentesis is unpleasant and
cumbersome.Therefore other therapeutic procedures
have been popular,but in general they are not very
effective (Table I). Pleurodesis Chemotherapy is one of
the most effective and it has become a frequent
procedure in recent years. In developed countries
approximately 40% of pleural effusions are now due to a
malignancy, the most frequent cause being lung cancer,
followed by cancer of the breast(3).
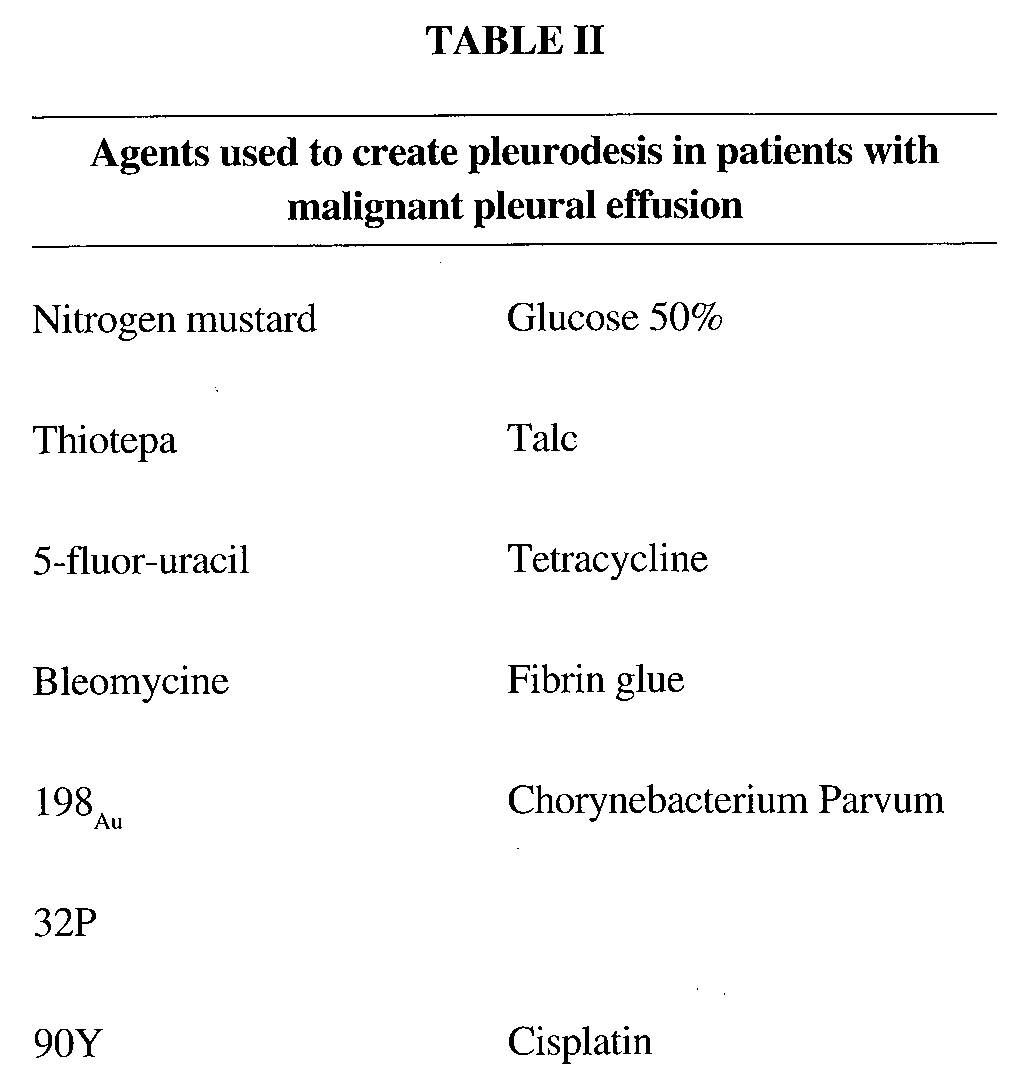
During the years many treatments have been used in pleural effusion connected with malignant disease in
order to obtain pleurodesis (Table II). Tetracycline has since it was first introduced in an animal study(4) and in man
1972(5) been increasingly popular in the treatment of as well pneumothorax as malignant effusion(6).
NEUMOSUR: REVISTA DE LA ASOCIACIÓN DE NEUMÓLOGOS DEL SUR VOL.3, NUMERO 1, ABRIL 1991
In the following the role of Tetracycline as a sclerosing agent in malignant pleural effusion is emphasised, but a
number of controlled randomized studies dealing with other sclerosing agents will be mentioned.
A statement like: Tetracycline is currently considered as the optimal sclerosing agent due to its high efficacy,
good patient tolerance, simple and repeatable application and low cost of treatment(6), is probably endorsed by many
clinicians. I shall try to find from the literature the evidence to justify this popular statement - if available.
MODE OF ACTION
Tetracycline was believed to create pleurisy leading to pleurodesis because of the low pH. It is not as simple as
that. Three different concentrations of Tetracycline with the same pH were given intrapleurally to rabbits. Only 35
mg/kg. created a pleural fibrosis and symphysis, whereas 7 and 20 mg/kg. did not. There seems to be a dose
response curve(7).
In a randomized study in patients this observation was confirmed. The occurrence of pleurodesis did not
depend on pH in the instilled substance but on the presence of Tetracycline(8).
The mode of action is not known for sure, but fibroblasts growth seems to be stimulated(9) probably by a factor
released by mesothelial cells(10). PROCEDURE
Before attempting pleurodesis it is essential to make sure the lung can expand.
The procedure can be performed in local anaesthesia.
Preoperative medication is necessary. It is well known, that the instillation of Tetracycline hurts and the patient it
often scared of the situation. Many different drugs have been used. We have for a long time used Levopromazine,
which at the same time is tranquilizer and a pain-killer(11), but many drugs are used with good results. The local
anesthesia for inserting the tube drainage has to be sufficient, as complications can occur if attention is not paid to this
detail(12).
Administration has mainly been through an indwelling tube drainage or a small bore catheter, which is clamped
Often a local anaesthetic is administered intrapleurally right before the Tetracycline is given. If Lidocain is used
a dosis of less than 3 mg/kg. is recommended(13), as this will not give blood levels that are toxic. Higher dosages, 250
mg as standard, have, however, been used without problems(14) and other local anaesthetics have been used as well.
By giving Tetracycline 20 mg/kg. intrapleurally therapeutic blood levels were found in 80% of the patients after 1
1/2 hour(13). 20 mg/kg is more than usually given. Most often a standard dose of 500 ing of Tetracycline is used(5).
The size of the tube does not seem essential for the result. Repeated instillation of Tetracycline has been
advocated. In a prospective, randomized study of one or two doses of 20 mg/ kg. Tetracycline intrapleurally no
difference was observed between the gropups, and thus just one dosis can be recommended(15).
There has been a tradition for shifting the patient into various positions in order to obtain a uniform distribution
of the drug. Isotope studies seem to indicate that this distribution will take place in all events(16). It is essential, that all
fluid is drained from the cavity and the drain is therefore left in situ until only a minimal amount of fluid is drained
during 24 hours, usually no more than 100 ml.
NEUMOSUR: REVISTA DE LA ASOCIACIÓN DE NEUMÓLOGOS DEL SUR VOL.3, NUMERO 1, ABRIL 1991
INDICATION AND CONTRAINDICATIONS FOR PLEURODESIS IN MALIGNANCY
The diagnosis of a malignancy must be certain and the turnourtype not sensitive to chemotherapy. The pleural
fluid should be present in such an amount, that symptoms arise (shortness of breath), and it recurs after evacuation.
The lung must not be trapped. This should be tested by expanding the lung before an irritant is instilled.
The general condition of the patient should be good and the life expectancy is at least 3 months. This last is a
difficult clinical evaluation. Some help may be gained by studies of pH and glucose levels in the pleural fluid(17). Very
old patients tolerate the procedure less well. It is a trauma to have tetracycline or other sclerosing substances instilled
in the pleura and in a weak patient this might be sufficient to hasten deterioration considerably.
COMPLICATIONS AND UNWANTED SIDE EFFECTS
Most patients experience some pain when Tetracycline is intilled in the pleural cavity. Pain is difficult to
measure, but the pain seems to be stronger in patients with pneumothorax than in patients with malignant pleural
The pain is ameliorated by proper premedication, by local anaesthesia in the pleural cavity and by a proper
preoperative explanation and psychic conditioning of the patient. Still it hurts some. The pain can provoke a vasovagal
attack with severe bradycardia and should for this reason too be minimised.
On the evening of the pleurodesis and on the following 23 days a rise in temperature in usual. Initial
temperatures up to 39-40 degrees centigrade are seen. This is not a sign of an infection but of anon-specific
inflammation. If the temperature elevation persists the possibility of a bacterial infection should be taken into
consideration. This is a rare complication, but empyemas are seen, as is local wound infection. The frequency of
these complications obviously depend on the sterile technique and on the number of days the tube drainage is left in
situ. The last statement is an assumption as no evidence from the literature is available. .
Spread of the neoplasm through the incision wound is known to occur after thoracoscopy, especially in
mesothelioma(18). Some will give profylactic irradiation to prevent this complication(18).
Subcutaneous emphysema is a very common finding but in the vast majority of cases it is unimportant, not
giving symptoms and will disappear by itself.
Respiratory insufficiency. If a plcurodesis is made in a patient with a severely reduced lung function the
following pain may inmobilise the chest and later the sedation may suppres the respiration. If patients are properly
selected respiratory insufficiency is no problem.
Pleural haemorrhage. If thrombocyte count is above 40.000 and prothrombine time over 40% haemorrhagic
complications of importance are rare. Patients receiving chemotherapy or on dialysis may give unexpected problems.
Trapped lung. The ability of the lung to expand after evacuation of fluid should be tested before pleurodesis. If
this is not done or if an inability to expand is ignored, the result will be a pleural cavity with a sterile inflammation,
which will make a possible later decortication even more difficult.
A search of the literature for complications to pleurodesis has been made. This did not prove productive. In the
very few prospective randomised studies no difference was found between tale and Tetracycline pleurodesis(19). No
significant difference was observed as far as complications were concerned between simple drainage and drainage +
talc. These results were substantiated in a study of patients treated with simple drainage, drainage + tale or drainage
NEUMOSUR: REVISTA DE LA ASOCIACIÓN DE NEUMÓLOGOS DEL SUR VOL.3, NUMERO 1, ABRIL 1991
+ Tetracycline for pneumothora(20). In a prospective comparison of corynebacterium parvum versus tetracycline fever
and pain was significantly less pronounced in the latter treatment(21).
Long term sequelae. From treatment of patients with pneumothorax with Tetracycline we know, that a few
continue to have an occasional stabbing pain in the chest(20).
As most patients with pleural effusion due to malignancy have a rather short survival, long term sequelae can
Effectivenes. As mentioned, the number of agents
and procedures used during the years in order create a
pleurodesis has been considerable. Most of them have
been published as effective, the success rate varying
between 25 and 100% (Table III). In most Studies
neoplasms originating in the lung and the breast
dominate, but this of course does not make the results
of the studies comparable. We know that success rate
with tale, Quinacrine ant Tetracycline are high whereas
lower success rate have been found using other
substances. Still we are not sure that the difference are
real, as controlled prospective randomised studies are
In our department at Bispebjerg Hospital, two
studies have been performed. In one study simple
repeated thoracocentesis was compared with repeated
thoracocentesis + Quinacrine(23). The Quinacrine
treatment was significantly better than thoracocentesis
In a later study from the department(11) simple drainage was compared to drainage + talc. Simple drainage was
followed by pleurodesis in approximately 60%, significantly lower than in the group in which talc was added, but still
higher than in reports on some sclerosing agents.
The number of non-evaluable patients is high, 7 died early, in 2 the lung could not be expanded and one got an
empyema, which illustrates the difficulties in these studies.
A randomized study of patients with breast cancer receiving either drainage alone or drainage+ 32 P showed no
significant difference betwen the groups. Again the response to drainage alone was approximately 60%(24).
The effect of corynebacterium parvum has been compared to Bleomycine in both conditions without drainage.
The sucess rate was highly in favour or corynebacteiiumparvum(25).
Corynebacterium parvum and Tetracycline have been compared. The study(21) is from two centers and
techniques were not uniform, but it seems that there was no significant difference in the sucess rate.
A comparison of tube drainage + Quinacrine or Tetracycline showed the treatments equally effective(26).
Doxycycline + tube drainage compaired with tale + drainage gave no difference of significance between the two
treatments(19). Fibrine glue + drain and Tetracycline + drain has been compared in a prospective study. There seems
to be no difference between the treatment(27).
NEUMOSUR: REVISTA DE LA ASOCIACIÓN DE NEUMÓLOGOS DEL SUR VOL.3, NUMERO 1, ABRIL 1991
STAY IN HOSPITAL, LENGTH OF DRAINAGE, COMPLICATIONS
Comparable data are available to a very limited extend. No difference was found between Tetracycline and talc
treatment in the study by Muir et al. 19. In the study by Bayly et al.(26) fever and pain was significantly less pronounced
in the Tetracycline than in the Quinacrine group. No significant difference was found between patients with
spontaneous pneumothorax, but this gruop is hardly comparable to the cancer group (20). PROGNOSIS
As the obliteration of the pleural space is only a palliative procedure little influence on the survival can be
expected. No study is available to give exact information on this topic.
It seems that the survival of patient eligeable forpleurodesis can be predicted by the pH and glucose level. This
should be used in the evaluation of patients for pleurodesis(28).
Low glucose and pH levels in the pleural fluid are predictors of a lower success rate in pleurodesis treatment(28).
The results are, however, not so much poorer that the treatment should not be attempted.
CONCLUSION
Following the established indications and procedures Tetracycline is an acceptable sclerosing agent in patients
with malignant pleural effusion. The results and side effects seem to be comparable to the results obtained with talc
LITERATURE
1. Bethune N.: Pleural pouderage: New technique for the deliberate production of pleural adhesion as preliminary to
lobectomy. J. Thorac. Surg. 1935; 4: 251-26 1.
2. Sahn SA.: Malignant pleural effusion. Clinics in Chest Medicine. 1985; 6: 113-125.
3. Enk B. and Viskum K.: Diagnostic Thoracoscopy. Eur. J. Respir. Dis. 198 1; 62: 344-35 1.
4. Thorsrud GK.: Pleural reaction to irritants, an experimental study with special reference to pleural adhesions and
concrescence in relation to pleural tum-over of fluid. Acta Chir. Scand. 1965; suppl. 355: 1-74.
5. Rubinson RM., Bolooki H.: Intrapleural tetracycline for control of malignant effusion: A preliminary report. South
6. Frank W., Grosser H., Mai J. and Loddenkermper R.: Pleurodese mit Tetracyclin-Hydrochlorid. Pneumonologie.
7. Satin SA. and Good JT.: The effect of common sclerosing agents on the rabbit pleural space.
8. Zaloznik AJ., Oswald SG., Langin M.: Intrapleural tetracycline in malignant pleural effusions. Cancer. 1983; 51:
9. Antony VB, Owen CL., Sahn SA.: Mechanisms of Tetracycline induced pleural fibrosis: Tetracycline stimulates
fibroblast proliferation in vivo and in vitro. Am. Rev. Resp. Dis. 1985; 131 suppl. A 33.
NEUMOSUR: REVISTA DE LA ASOCIACIÓN DE NEUMÓLOGOS DEL SUR VOL.3, NUMERO 1, ABRIL 1991
10. Rennard SI, Jaurand M-C., Bignon J., Kawanami 0., Ferans VJ., Davidson J. and Chrystal RG.: Role of Pleural
mesothelial cells in the production of the submesothelial connective tissue matrix of lung. Am. Rev. Respir Dis. 1984;
11. Sorensen PG., Svendsen TL. and Erik B.: Treatment of malignant pleural effusion with drainage with and without
12. Viskum K. and EnK B.: Complications of thoracoscopy. Poumon et Coeur 1981; 37: 25-28.
13. Wooten SA., Barbarash RA., Strange C. and Sahn SA.: Systemic absorption of Tetracycline and Lidocaine
following intrapleural instillation. Chest. 1988; 94: 960-963.
14. Sherman S., Ravikrishnan KP., Patel AS. and Seidman JC.: Optimum anesthesia with intrapleural Lidocaine
during chemical pleurodesis with Tetracycline. Chest. 1988; 93: 533-536.
15. Landvater L., Hix WR., Mills M., Siegel RS. and Aaron BL.: Malignant pleural effusion treated by Tetracycline
sclerotherapy. Chest. 1988; 93: 1196-1198.
16. Lorch DG., Gordon L., Wooten S., Cooper JF., Strange C. and Satin SA.: Effect of patient positioning on
distribution of Tetracycline in the pleural space. Chest 1988; 93: 527-529.
17.Rodrfguez-Panadero F. and López-Mejías J.: Survival time of patients with Pleural Metastatic Carcinoma predicted
by glucose and pH studies. Chest. 1989; 95: 320-324.
18. Boutin C., Villat JR., Cargnino P. and Farisse P.: Thoracoscopy in malignant pleural effusions. Am. Rev. Resp.
19. Muir JF., Cerisel F., Defouilloy C., Broussier PM., Hermont A., Aubry P., Ndarunze S., Botto MJ. and Arlati S.:
Pleural drainage with talc versus Doxycycline in the control of malignant pleural effusion. 6th Congress of the
European Society of Pneumonology, Amsterdam 1987. Congress report page 212.
20. Almind M., Lange P. and Viskum K.: Spontaneous pneumothorax: Comparison of simple drainage, talc
pleurodesis and Tetracycline pleurodesis. Thorax. 1989; 44: 627-630.
21. Leahy BC., Honeybourne D., Brear SG., Carroll KB., Thatcher N. and Stretton TB.: Treatment of malignant pleural
effusions with intrapleural corynebacterium parvurn or Tetracycline. Eur. J. Resp. Dis. 1985; 66: 50-54.
22. Austin EA. and Flye MW.: The treatment of Recurrent Malignant Pleural effusion. Ann. Thorac Surg. 1979; 28:
23. Mejer J., Mortensen KM and Hansen HH.: Mepacrine Hydrochloride in the treatment of malignant pleural effusion.
24. lzbicki R., Weyhing BT., Baker L., Caoili EM. and Vaitkevicius VK.: Pleural effusion in cancer patients. A
prospective randomized study of pleural drainage with the addition of radioactive phosphorous to the pleural space
pleural drainage alone. Cancer. 1975; 36: 1511-1518.
25. Hillerdal G., Kiviloog J., N6u E., Steinholtz L.,: Corynebacterium parvum in malignant pleural effusion. A
randomized prospective study. Eur. J. Respir Dis. 1986; 69: 204-206.
26.Baylic TC., Kisner DL., Sybert A., MacDonald JS., Tsou E., Schein PS: Tetracycline and Quinacrine in the control
of malignant pleural effusions. Cancer 1978; 41: 1188-1192.
27. Gust R. and Fabel H. Fibrinkleber-Pleurodese bei rezidivierenden malignen Pleuraergüssen. Pneumonologie
28. Rodríguez-Panadero F., López Mejías J.: Low glucose and pH levels in malignant pleural effusions. Diagnostic
significance and prognostic value in respect to pleurodesis. Am. Rev. Respir. Dis.1989; 139: 663-667.
MEDICATION GUIDE LYRICA (LEER-i-kah) (pregabalin) Capsules and Oral Solution, CV Read this Medication Guide before you start taking LYRICA and each time you get a refill. There may be new information. This information does not take the place of talking to your healthcare provider about your medical condition or treatment. If you have any questions about LYRICA, ask your healthcare pro
CONTRATO MARCO Entre …………………………. en…………………………………………, representada por su Director General …………………., con C.I Nº ……………. en adelante LA EMPRESA, y la SOCIEDAD PARAGUAYA DE CIRUGIA (SOPACI) representada por el Dr. Osmar Cuenca , con C.I Nº …………… y los Capítulos de Cirugía Torácica representad
 NEUMOSUR: REVISTA DE LA ASOCIACIÓN DE NEUMÓLOGOS DEL SUR VOL.3, NUMERO 1, ABRIL 1991
PLEURODESIS IN MALIGNANT PLEURAL EFFUSION WITH
NEUMOSUR: REVISTA DE LA ASOCIACIÓN DE NEUMÓLOGOS DEL SUR VOL.3, NUMERO 1, ABRIL 1991
PLEURODESIS IN MALIGNANT PLEURAL EFFUSION WITH 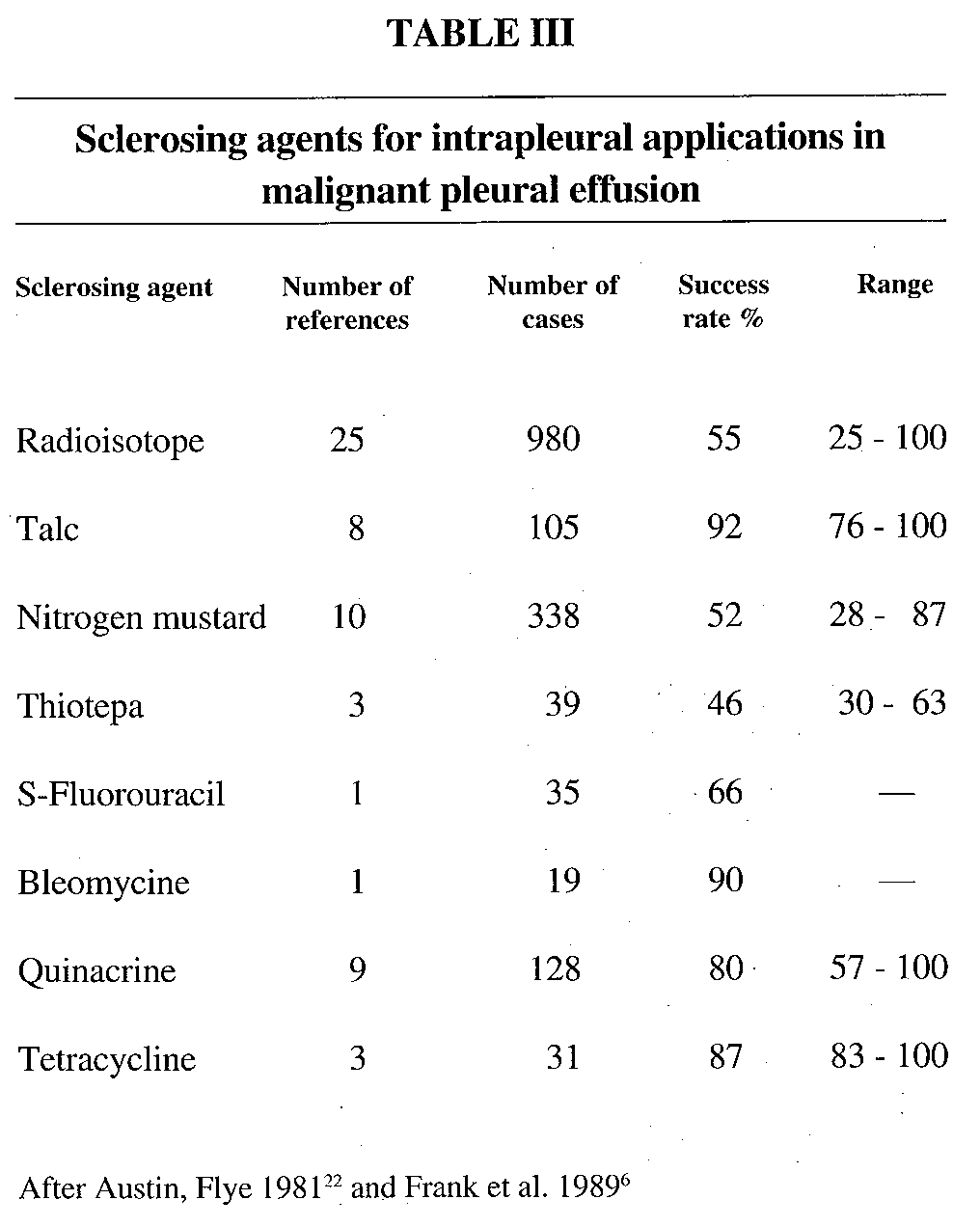 NEUMOSUR: REVISTA DE LA ASOCIACIÓN DE NEUMÓLOGOS DEL SUR VOL.3, NUMERO 1, ABRIL 1991
NEUMOSUR: REVISTA DE LA ASOCIACIÓN DE NEUMÓLOGOS DEL SUR VOL.3, NUMERO 1, ABRIL 1991