Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Services.aarc.org
Scott P Marlow RRT and James K Stoller MD MSc FAARC
Introduction Epidemiology of Cigarette Smoking Nicotine Addiction Smoking Cessation Interventions: Overview Behavioral Interventions Pharmacologic Interventions Nicotine Replacement Therapy Bupropion Second-Line Smoking Cessation Drugs Alternative Smoking Cessation Interventions Combined Smoking Cessation Interventions Cost The Respiratory Therapist’s Role in Smoking Cessation Summary Cigarette smoking is the primary cause of chronic obstructive pulmonary disease, and smoking cessation is the most effective means of stopping the progression of chronic obstructive pulmonary disease. Worldwide, approximately a billion people smoke cigarettes and 80% reside in low-income and middle-income countries. Though in the United States there has been a substantial decline in cigarette smoking since 1964, when the Surgeon General’s report first reviewed smoking, smoking remains widespread in the United States today (about 23% of the population in 2001). Nicotine is addictive, but there are now effective drugs and behavioral interventions to assist people to over- come the addiction. Available evidence shows that smoking cessation can be helped with counseling, nicotine replacement, and bupropion. Less-studied interventions, including hypnosis, acupuncture, aversive therapy, exercise, lobeline, anxiolytics, mecamylamine, opioid agonists, and silver acetate, have assisted some people in smoking cessation, but none of those interventions has strong research evidence of efficacy. To promote smoking cessation, physicians should discuss with their smoking patients “relevance, risk, rewards, roadblocks, and repetition,” and with patients who are willing to attempt to quit, physicians should use the 5-step system of “ask, advise, assess, assist, and arrange.” An ideal smoking cessation program is individualized, accounting for the reasons the person smokes, the environment in which smoking occurs, available resources to quit, and individual preferences about how to quit. The clinician should bear in mind that quitting smoking can be very difficult, so it is important to be patient and persistent in developing, implementing, and adjusting each pa- tient’s smoking-cessation program. One of the most effective behavioral interventions is advice from a health care professional; it seems not to matter whether the advice is from a doctor, respiratory therapist, nurse, or other clinician, so smoking cessation should be encouraged by multiple clinicians. However, since respiratory therapists interact with smokers frequently, we believe it is particularly important for respiratory therapists to show leadership in implementing smoking cessation. Key words: chronic obstructive pulmonary disease, COPD, smoking cessation.
[Respir Care 2003;48(12):1238 –1254. 2003 Daedalus Enterprises]
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
Fig. 1. Percentage of adult current, former, and never smokers. (Adapted from Reference 4.)
Introduction
that smoking prevalence has increased to approximately1.1 billion people (1 in 3 adults), with 80% of these re-
In reviewing smoking cessation the present report first
siding in low- and middle-income countries.2 Smoking
summarizes the epidemiology of smoking cessation and
remains widespread in the United States, though trends
evidence that smoking causes harm. We next review the
show a substantial decline since 1964. Cigarette smoking
physiology of nicotine and smoking addiction and the ben-
was rare in the early 20th century, when the annual per
efits of smoking cessation. Finally, we present a system-
capita United States consumption rate was 54 cigarettes. In
atic review of smoking cessation methods, with evidence-
1964 the per capita consumption was 4,345 cigarettes/
person/y, and that rate had declined to 2,261 cigarettes/
Although primary smoking prevention (eg, education,
person/y in 1998.3 As shown in Figure 1, the prevalence of
regulation of advertising) is recognized as an integral part
current smokers peaked in 1965 at 42.4% and had declined
of combating smoking, the reader is referred to other re-
to 23.4% in 2001.4,5 This decline has been referred to by
cent publications for comprehensive reviews of this issue,
the Centers for Disease Control and Prevention as one of
such as the Report of the Surgeon General released in
the “Ten Great Public Health Achievements in the 20th
Though the decline in smoking certainly represents a
Epidemiology of Cigarette Smoking
favorable trend, smoking is, disturbingly, most commonamong groups of lower socioeconomic status. Figure 2
Smoking is a modern day epidemic that poses substan-
shows that the prevalence of smoking is higher among
tial health burden and cost. Worldwide estimates suggest
individuals in families with combined incomes Ͻ $9,000(35% prevalence) than in families with a combined in-come exceeding $75,000 (19% prevalence).7 Figure 3
Scott P Marlow RRT and James K Stoller MD MSc FAARC are affili-
shows that these trends are also evident by education
ated with the Department of Pulmonary and Critical Care Medicine, TheCleveland Clinic Foundation, Cleveland, Ohio.
level, with a higher frequency of smoking among thosewho have not completed high school (33%) than among
Scott P Marlow RRT presented a version of this report at the 32nd
those who have completed 4 years of college (14%).7
RESPIRATORY CARE Journal Conference, Chronic Obstructive PulmonaryDisease: Translating New Understanding Into Improved Patient Care,
For example, in 1965, 51.9% of men and 33.9% of
held July 11–13, 2003, in Los Cabos, Mexico.
women reported smoking, whereas in 2000 25.7% ofmen and 21.0% of women reported smoking.4,8 Smok-
Correspondence: Scott P Marlow RRT, Department of Pulmonary and
ing rates among high school students continue to exceed
Critical Care Medicine, A90, The Cleveland Clinic Foundation, 9500Euclid Avenue, Cleveland OH 44195. E-mail: marlows@ccf.org.
the national rate for adults, having increased during the
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
Fig. 2. Percentage of people Ն 18 years old who reported smoking in the past month, by combinedtotal family income, 1999 –2000. (Adapted from Reference 7.)
Fig. 3. Percentage of people Ն 18 years old who reported smoking in the past month, by educationlevel, 1999 –2000. (Adapted from Reference 7.)
1990s to a peak of 36.4% in 1997 and since decreased
smoking.10 Smoking also increases the risk of death in
to 28.5% in 2001 (29.2% among boys versus 27.7%
many illnesses. Table 1 shows the relative risk of smok-
ing-attributable morbidity and mortality from various con-
Because smoking is common, the economic impact is
ditions, largely including respiratory, cardiovascular, and
profound. In 1998 the direct medical cost of smoking
neoplastic diseases.11 Table 2 shows estimates of the num-
was estimated to be $75.5 billion, with productivity
ber of deaths attributed to smoking. Notably, the 35,053
losses estimated at $82 billion and smoking-related neo-
second-hand-smoke-related deaths are not included in those
natal costs estimated at $366 million.10 When all ex-
penses are combined, they represent a total of $3,391
Smoking confers a risk of serious illness, and smoking
per smoker per year, which amounts to approximately
cessation offers health benefits, which is evident in Table
8% of all annual health care expenditures in the United
1: former smokers have lower relative risk of death in all
disease categories.11 For example, compared to never-
The morbidity and mortality attributed to smoking are
smokers, men who are current or former smokers have a
also substantial. For example, between 1995 and 1999
higher relative risk of death from cancer of the trachea,
approximately 440,000 deaths annually were attributed to
lung, or bronchus (23.26 times higher in current smokers
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
Relative Risk of Death: Current Smokers Versus Former
decline (30.2 mL/y among men and 21.5 mL/y amongwomen) than active smokers (66 mL/y among men and
and 8.7 times higher in former smokers).11 The 1990 re-
port of the United States Surgeon General on the healthbenefits of smoking cessation concluded that people who
Nicotine Addiction
quit smoking before the age of 50 have half the risk ofdying in the next 15 years, compared to continuing smok-
Concepts of nicotine addiction have evolved over the 40
ers.12 Smokers have twice the risk of dying of coronary
years since the Surgeon General’s report first reviewed
heart disease or stroke, and the risk of coronary heart
smoking. For example, in 1964 the Report of the Advisory
disease diminishes by half in the first year after cessa-
Committee to the Surgeon General classified tobacco as
tion.12 After 5–15 years of abstinence from smoking, the
“an habituation rather than an addiction” and that prevent-
risk of both stroke and heart disease drops to the level of
ing the psychogenic drive of the habit was more important
Another benefit of quitting smoking is a slowing of the
Concepts about the physiology of nicotine addiction have
accelerated rate of lung function decline that occurs in
since evolved. For example, in 1979 the Report of the Sur-
susceptible smokers. For example, the Lung Health Study
geon General cited nicotine as “a powerful addictive drug.”16
randomized and followed 5,887 smokers with early chronic
And in 1988 the Report of the Surgeon General on The
obstructive pulmonary disease in one of 3 arms: usual
Consequences of Smoking: Nicotine Addiction17 concluded:
care; aggressive smoking intervention with ipratropium
• Cigarettes and other forms of tobacco are addicting.
bromide via metered-dose inhaler; and smoking inter-vention with placebo inhaler.13 Long-term follow-up of
• Nicotine is the drug in tobacco that causes addiction.
the Lung Health Study cohort found that 11-year sus-tained ex-smokers experienced a lower rate of FEV
• Pharmacologic and behavioral processes that determine
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
tobacco addiction are similar to those that determine
addiction to drugs such as heroine and cocaine.
Though debated, the physiology of nicotine addiction
Individual counseling by nurse or other nonphysician
has recently been characterized as biphasic, in that it stim-
ulates the pleasure response to the brain, and when taken
for longer periods, also creates a relaxed state. As with
cocaine, amphetamines, and morphine, addiction to nico-
tine is believed to result from increased release of dopa-
First-Line: Nicotine replacement therapy (transdermal patch, gum,
mine in the region of nucleus acumbens.18–20 Nicotinic
acetylcholine receptors are located throughout the central
nervous system, but the neurons located in the ventral
tegmental area increase activity with nicotine administra-
tion and concurrently activate the increased release of do-
pamine into the nucleus acumbens.18,21,22 Corrigall et al23,24
found that self-administered nicotine in vivo is reduced by
lesions to these pathways or by a nicotinic antagonist in-
fused into the ventral tegmental area.
As with all addictions, nicotine withdrawal elicits a num-
ber of clinical consequences, avoidance of which promotessmoking. Nicotine withdrawal symptoms are time-limited,can last for several weeks, and include physical symptoms
mends discussing the 5 “R”s: relevance, risk, rewards,
of irritability, anxiety, depression, difficulty concentrating,
roadblocks, and repetition (Table 5).28
weight gain, restlessness, and impatience.25 The intensity
In summarizing the literature and offering recommen-
of these withdrawal symptoms can be related to the level
dations, we first present evidence from the Cochrane Col-
of nicotine dependence. A common measuring tool is the
laboration reviews of smoking cessation interventions,
Fagerstrom Test for Nicotine Dependence, which rates
which considered studies up to 2002. We also review data
addiction on a 0 –10 scale. The test places the most em-
presented in the USDHHS Clinical Practice Guideline for
phasis on the length of time after waking before the first
Treating Tobacco Use and Dependence, originally pub-
cigarette and the number of cigarettes smoked per day.26
lished in 1996 and updated in 2000.28 To identify the most
As evidence of the power of nicotine addiction, estimates
recent available data, we searched MEDLINE for research
suggest that 70% of smokers would like to quit, that ap-
conducted in 1999 through June 2003, using the search
proximately 41% try to quit each year, but that only 4.7%
terms “smoking cessation” and “tobacco.” Our ratings of
the strength of the available evidence are based on thesystem adopted by Fiore et al (Table 6).28 To assess the
Smoking Cessation Interventions: Overview
efficacy of the available interventions, we largely restrictedthe analysis to studies that compared interventions to no-
The spectrum of available smoking cessation interven-
tions can be classified into behavioral, pharmacologic, and
Overall, the available literature supports the efficacy of
alternative methods (Table 3). Behavioral interventions
behavioral counseling, nicotine replacement, and bupro-
include physician advice, individual counseling, group
pion in smoking cessation (Table 7). Clinicians should
counseling, and telephone counseling. Pharmacologic in-
know that an ideal smoking cessation program is individ-
terventions include nicotine replacement therapy, sus-
ualized, accounting for the person’s reasons to smoke, the
tained-release bupropion, clonidine, and nortriptyline. Fi-
environment in which smoking occurs, available resources
nally, alternative (and less-studied) interventions include
to quit, and individual preferences about how to quit.
hypnosis, acupuncture, aversive therapy, exercise, lobe-line, anxiolytics, mecamylamine, opioid agonists, and sil-ver acetate. Behavioral Interventions
Smoking cessation should begin with assessing the smok-
er’s desire to quit. Table 4 describes the 5 “A”s: ask,
Behavioral interventions differ according to who is per-
advise, assess, assist, and arrange. For smokers unwilling
forming the intervention: the physician, nurse, nonphysi-
to attempt quitting, the United States Department of Health
cian clinician, telephone counselor, or patient self-help.
and Human Services (USDHHS) Clinical Practice Guide-
The present analysis compares cessation rates for each
line for Treating Tobacco Use and Dependence recom-
behavioral intervention to a control group with no (or
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
Smoking Cessation Intervention: The 5 “A”s
If patient is willing to quit, assess potential intensity of support
If patient is not willing to quit, see Table 5
Enlist support and understanding of family and friends
Anticipate challenges, especially first few weeks
Provide practical counseling (eg, problem-solving and skills training)
Review relationship of alcohol to tobacco use
Point out that having other smokers in the home will increase the difficulty
Provide a supportive clinical environment
Help obtain extra treatment social support
Help obtain patient-environment support from family, friends, and coworkers
Sources: organizations that promote smoking cessation, including federal, state, and nonprofit organizations
Type: Are the materials appropriate for the patient, in relation to culture, race, education, and age?
Location: Are the materials readily available?
Timing: Follow up within the first week of the quit date, and follow up again within the first month
Remind that lapse is a learning experience
Consider increased intervention when necessary
minimal) intervention. Limitations of available studies
1.23–1.68 and OR 2.66, 95% CI 2.06 –3.45).29 In agree-
are that behavioral interventions are supplied in a vari-
ment with the Cochrane Collaboration reviews, findings
ety of environments or with other (confounding) inter-
from the USDHHS Clinical Practice Guideline review of
ventions. For example, a study may provide physician
available studies showed that brief (ie, 2–5 min) physician
and group advice for smoking cessation along with nic-
advice was associated with a 2–3% higher rate of smoking
otine gum, as in the Lung Health Study,13 thereby con-
cessation (OR 1.3, 95% CI 1.1–1.6).28 Denny et al30 re-
founding direct comparisons of the nicotine and the
ported that 70% of smokers who had seen their doctor
within the last 12 months received advice to quit smoking.
Among the simplest of behavioral interventions, even
However impressive that 70% figure appears, the 30% of
brief, direct physician advice to quit smoking is effective.
smokers who did not receive quit-smoking advice is ap-
For example, in the Cochrane Library review of 16 stud-
proximately 1,915,000 smokers in the 10-state survey ar-
ies, Silagy et al29 found that brief physician advice in-
ea—a tremendous number of missed opportunities to en-
creased the absolute rate of abstinence by 2.5% over usual
courage smoking cessation.29 If only 2.3–2.5% of those
care (odds ratio [OR] 1.69, 95% confidence interval [CI]
individuals had quit after brief advice, an additional
1.45–1.98). Furthermore, the rate of smoking abstinence
44,000 – 48,000 smokers may have quit.
increased when the intensity of advice was increased and
With regard to counseling by nurses, Rice and Stead31
when follow-up visits were included (OR 1.44, 95% CI
reported small increases in smoking cessation rate follow-
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
Enhancing Motivation to Quit Tobacco: The 5 “R”s
Why would quitting be personally relevant? Consider family, children, health concerns, previous experience, work
Clinician should ask patient to identify negative consequences of smoking:
Emphasize that low-tar, low-nicotine, and other forms of tobacco do not eliminate risk
Cancer: lung, larynx, oral cavity, pharynx, esophagus, pancreas, bladder, cervix
Increased risk of lung cancer and heart disease in spouse
Higher rate of smoking among children of tobacco users
Increased risk of low birth weight, sudden infant death syndrome, asthma, middle ear disease, and respiratory infections
Ask patient to identify potential rewards and highlight those most relevant to the patient
Home, clothing, and breath will smell better
Ask patient to identify barriers to quitting and address elements of treatment that can assist
Repeat every time an unmotivated patient visits the clinic setting. Tobacco users who have failed in previous quit attempts
should be told that most people make repeated quit attempts before they are successful.
ing nurse advice (OR 1.5, CI 1.29 –1.73). Pooled results of
and should be encouraged (OR 1.7, CI 1.3–2.1), and no
16 trials in a Cochrane Collaboration review showed that
specific clinician type demonstrated superiority, so smok-
receipt of nursing advice was associated with a cessation
ing cessation should be encouraged by multiple health care
rate of 13.3%, compared with the control group rate of
providers. The strength of evidence supporting these rec-
12.1%.31 A review of 29 studies by Fiore et al28 offered 2
ommendations is rated A (see Table 7).
conclusions: smoking cessation intervention by nonphysi-
In a Cochrane Library review of 15 studies Lancaster
cians increases abstinence, compared to control groups,
and Stead32 compared individual smoking intervention by
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
Strength of Evidence Categories for Recommendations
junct to face-to-face intervention and can be provided pro-actively or reactively (eg, telephone help lines). Meta-
analyses by Stead et al34 and Fiore et al28 found a similar
magnitude of effect. Telephone counseling, compared tominimal or no intervention, conferred an approximately
Multiple well designed randomized clinical
2% absolute rise in the cessation rate (OR 1.56, CI 1.38 –
trials, directly relevant to therecommendation, that yield a consistent
1.77 and OR 1.2, CI 1.1–1.4, respectively).
Telephone help lines have been harder to assess. How-
Some evidence from randomized clinical trials
ever, in a comparison of smokers who received mailed
self-help material to those who received self-help material
and notification of a help line, Ossip-Klein et al35 reported
instance, few randomized trials exist, the
a 2.6% absolute increase in abstinence among those who
trials that exist are somewhat inconsistent, orthe trials are not directly relevant to the
knew about the help line. Evidence that telephone contact
is effective in supporting smoking cessation is rated A (see
Reserved for important clinical situations
where the panel achieved consensus on the
Self-help information is marginally beneficial for in-
recommendation in the absence of relevant
creasing smoking cessation. Examples of self-help mate-
rials include booklets, leaflets, brochures, videotapes, com-
pact discs, help lines, and various computer and Internetinterventions. For example, Lancaster and Stead36 con-firmed benefit in a review of 12 studies that compared
a counselor trained in smoking cessation to no intervention
self-help cessation materials to no intervention; self-help
and found that counseling by an individual improved the
materials slightly improved cessation rates (OR 1.24, CI
abstinence rate by 4% (OR 1.62, CI 1.35–1.94). The
1.07–1.45). Enhanced or tailored self-help material was
USDHHS Clinical Practice Guideline used a different ap-
associated with better cessation rate than standard self-
proach; Fiore et al28 assessed the effectiveness of individ-
help material (OR 1.36, 1.13–1.64), but the addition of
ual counseling by pooling 58 studies involving physicians,
self-help material to counseling did not increase cessation
nurses, and nonphysicians. They reported an overall 6%
rate, nor did the use of multiple self-help interventions,
absolute increase in the abstinence rate (OR 1.7, CI 1.4 –
such as multiple mailings.36 Fiore et al28 reported only a
2.0). In summary, available meta-analyses and key indi-
minimally better cessation rate with self-help materials
vidual studies establish the efficacy of individual counsel-
than with no intervention (OR 1.2 1.02–1.3). Overall,
ing from a physician, nurse, or nonphysician in increasing
though the effectiveness was nominal, self-help also
achieved evidence level A (see Table 7).28,36 Other reasons
Available studies also suggest that group counseling is
that self-help, despite its small impact, should be included
effective in promoting smoking cessation.28,33 Examples
in smoking programs are increased population awareness,
of group formats include the American Lung Associa-
low expense, and the opportunity to customize the mes-
tion’s “Freedom from Smoking” program and the Amer-
ican Cancer Society’s “Fresh Start” program. In a Co-
Another lesson from available meta-analyses of behav-
chrane Library review of 54 trials of various group
ioral interventions is that adding formats confers incre-
intervention formats, Stead and Lancaster33 found a 10%
mental effectiveness.28 As shown in Figure 4, combining
higher abstinence rate in the 6 trials that compared group
up to 3– 4 formats (eg, self-help with individual counsel-
intervention to no intervention (OR 2.19, CI 1.42–3.37). In
ing, or individual counseling and telephone counseling)
a concordant analysis of pooled studies, the USDHHS
may increase the absolute cessation rate by 12%.28
study reported an overall 3% absolute rise in the absti-
Also, increasing the intensity of interventions enhances
nence rate after group counseling (OR 1.3, CI 1.1–1.6).28
smoking cessation rates (Figures 5–7). Fiore et al28 found
The difference in cessation rates (10% vs 3%) between the
a strongly dose-related increase in cessation rate as the
2 reviews may reflect the fact that the USDHHS review
number of separate interventions increased. Factors in-
did not directly compare group intervention to no inter-
creasing effectiveness include the duration of each indi-
vention, but rather pooled 58 studies and used a variety of
vidual session, the total time spent in all sessions, and the
comparators.28 Overall, the evidence supporting the effi-
number of sessions. With minimal (Ͻ 3 min) counseling,
cacy of group counseling satisfies level A (see Table 7).
the cessation rate was 13.4%; with low-intensity counsel-
Telephone counseling is simple and permits reaching a
ing (3–10 min), the rate was 16.0%; with high-intensity
large number of people at critical cessation moments. Tele-
counseling (Ͼ 10 min), the rate was 22.1%.28 Total con-
phone counseling can be provided in lieu of or as an ad-
tact time ranged from zero to Ͼ 300 min, with no en-
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
Summary of Behavioral and Pharmacologic Smoking Cessation Interventions
Physician advice is effective and should be routinely .
Marginal but measurable benefit from intervention.
Improvement increased with pooled USDHHS data.
Better margin of improvement with the Cochrane
Collaboration data because of looking only at group
versus no intervention. If group versus self-help were
included, effect size would diminish.
Individual counseling Health care specialist
Health care specialist counseling improves cessation and
Proactive telephone calls are successful for improving
Marginal effectiveness but an important adjunct to
Evidence clear that nicotine gum improves success of
smoking cessation. Increase dose to 4 mg for highlydependent smokers (odds ratio 2.18, 95% confidenceinterval 1.48–3.7)
Evidence supports nicotine patch for improved smoking
abstinence. No difference found between 16-h and
Improvement in smoking cessation rate. Limited number
of studies compared to other NRT interventions.
Evidence supports inhaler use. Limited number of studies
compared to other NRT interventions.
Bupropion (300 mg/d 150 mg/d for 3 d, then
Evidence is strong that bupropion increases cessation
rate. May also prove effective with NRT.
*When possible, studies compare intervention to no or minimal intervention. †Absolute increase in smoking cessation rate (ie, intervention vs control)‡Italicized data is from the Cochrane Collaboration reviews. USDHHS ϭ United States Department of Health and Human ServicesNRT ϭ nicotine replacement therapy(Adapted from References 28, 29, 31–34, 36, 38, 39.)
hanced effectiveness beyond 90 min of counseling.28 A
a quit rate of 12.4%, whereas those with Ն 8 sessions had
review of the impact of the number of counseling sessions
a quit rate of 24.7% (see Fig. 7).28 In the Cochrane Col-
found that the greater the number of sessions, the greater
laboration review, the intensity of interventions was de-
the chance for cessation. Programs with 0 –1 sessions had
fined differently. For example, nursing interventions were
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
Fig. 4. Meta-analysis of estimated cigarette-smoking abstinence rates relative to number of smokingcessation formats used. The formats included self-help, proactive counseling, group counseling, andindividual counseling (n ϭ 54). (Adapted from Reference 28.)
Fig. 5. Estimated cigarette-smoking abstinence rates relative to the duration of the individual coun-seling session (n ϭ 43 studies). (Adapted from Reference 28.)
Fig. 6. Meta-analysis of estimated cigarette-smoking abstinence rates relative to the total amount ofcontact time (n ϭ 35 studies). (Adapted from Reference 28.)
considered low intensity if Յ 10 min and high intensity
with one follow-up.28 Based on these definitions, increased
if Ͼ 10 min with a follow-up appointment,30 whereas phy-
intensity of nursing intervention did not significantly in-
sician interventions were defined as minimal intensity if Յ
crease cessation rates (low intensity OR 1.67, CI 1.14 –
20 min with one follow-up visit and intensive if Ͼ 20 min
2.45, high intensity OR 1.47, CI 1.26 –1.72),30 whereas
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
Fig. 7. Estimated cigarette-smoking abstinence rates relative to the number of counseling sessions(n ϭ 43 studies). (Adapted from Reference 28.)
increasing intensity of physician intervention did modestly
cations assist in smoking cessation, and some are available
increase the smoking cessation rate (OR 1.67, CI 1.45–
over-the-counter, caution is advised not to overestimate
1.98).28 In contrast, in an analysis of 3 trials involving
their efficacy and undermine the power of will in quitting.
individual counseling with various intensities, Lancaster
Prochazka42 cautioned against considering cessation med-
and Stead32 did not find evidence to suggest that increased
icines a “magic bullet,” but instead counsels against un-
intensity of individual counseling increased cessation rate
realistic expectations and advises a detailed understanding
A more recent study by Simon et al37 randomized 228
patients to either low- or high-intensity intervention, with
Nicotine Replacement Therapy
all receiving nicotine replacement therapy (NRT) via patch. The 1-year abstinence rate was significantly higher in thehigher-intensity counseling group (29% vs 20%, OR 1.6,
Nicotine replacement therapy is supplied in several
forms: patch, gum (polacrilex), nasal spray, inhaler, and
Overall, evidence suggesting that increased intensity of
lozenges. Favorable features of NRT are that it is readily
counseling enhances abstinence achieves evidence level A
available, easy to use, relatively inexpensive, and effec-
(see Table 7). Limitations of counseling include the cost of
counseling sessions, limited availability to large popula-
Nicotine patch is applied transdermally and nicotine is
tions, and the time-intensiveness of the interventions for
absorbed through the skin. Nicotine patches are available
over-the-counter and come in doses of 7 mg, 14 mg, or 21mg (generic or Nicoderm CQ patch) or 5 mg, 10 mg, or 15
Pharmacologic Interventions
A Cochrane Library review by Silagy et al38 of 96 trials
The first-line pharmacologic interventions are NRT and
comparing all forms of NRT to controls found that absti-
bupropion (an antidepressant). The 2 second-line drugs are
nence rates were 7% better with NRT (OR 1.74, CI 1.64 –
clonidine (an antihypertensive) and nortriptyline (a tricy-
1.86). Nicotine patch was associated with a 6% better
clic antidepressant). Available guidelines suggest that NRT,
abstinence rate than controls (OR 1.74, CI 1.57–1.93).
antidepressants, and certain antihypertensives effectively
Similar findings were reported by the USDHHS Clinical
increase smoking cessation rates.28,38–40 Table 8 summa-
Practice Guideline,28 which showed an increased quit rate
rizes the 5 first-line Food and Drug Administration (FDA)
of 7.7%, based on review of 26 studies (OR 1.9, CI 1.7–
approved smoking cessation medications.
The mechanisms of drugs to aid smoking cessation dif-
Regarding the duration of patch use, the 16-hour and
fer. NRT offsets the craving for nicotine. Although the
24-hour patches appear to confer similar benefit.38 Still,
precise mechanism is unknown, bupropion is thought to
the long-term effectiveness of NRT has decreased since
blunt the impact of nicotine withdrawal in smoking ces-
NRT became available over-the-counter in 1996, possibly
sation by diminishing the uptake of dopamine and norepi-
because advice from health care providers diminished as
nephrine, thus decreasing cravings.41 Though these medi-
the need for a prescription to receive the patch vanished.43
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
First-Line Medications for Smoking Cessation
nicotine achievedwithin 20–30 min.
*Cost data are from average price from 3–4 national pharmacies(Adapted from Reference 28 and manufacturers’ information.)
Overall, the evidence supporting nicotine patches warrants
Murray et al44 found no adverse cardiovascular effects
from nicotine gum, even among those who smoked and
Nicotine gum (polacrilex) has also been available over-
continued to chew gum. Still, approximately 25% of nic-
the-counter since 1996 and is also effective in promoting
otine gum users experienced one or more adverse effects,
smoking cessation.28,38 Nicotine gum is available in 2-mg
including mouth irritation, headache, and indigestion.44 The
and 4-mg doses (Nicorette, Nicorette Mint, or generic).
evidence supporting the efficacy of nicotine gum to in-
Nicotine gum allows absorption of nicotine through the
crease smoking abstinence is substantial and is rated A
Regarding efficacy, a Cochrane review of 51 studies by
Nicotine nasal spray (Nicotrol NS) provides the most
Silagy et al38 found that nicotine gum increased the effec-
rapid nicotine administration of all the NRTs, with peak
tiveness of cessation attempts by 8%, compared to controls
effects within 5–10 min.28,38 Nicotine nasal spray must be
(OR 1.66, CI 1.52–1.81). Similarly, in a meta-analysis of
administered correctly for maximum effectiveness. One squirt
13 studies Fiore et al28 estimated a 6.6% better cessation
(0.5 mg) into each nostril delivers a total dose of 1 mg.
rate with nicotine gum (OR 1.5, CI 1.3–1.8). Patients who
The dose should not be inhaled or sniffed and should be
are highly nicotine dependent (who smoke Ͼ 25 ciga-
delivered with the head slightly tilted.28 Adverse effects
rettes/d) or those who have failed the 2-mg dose should
are common, with 94% of users reporting some nasal ir-
use the 4-mg dose, but should use no more than 24 pieces
ritation, which persists in 81% of users for up to 3 weeks
per day.28,38 In a study of 3,094 patients receiving nicotine
after initiation.28 Attractive features of nicotine spray are
gum in both treatment arms of the Lung Health Study,
that it is rapidly absorbed and can reduce nicotine craving,
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
offers a substitute for the cues of smoking, and can be
Regarding combined NRT use, the Cochrane Collabo-
administered as needed, up to 40 doses per day. Disad-
ration analysis38 pooled 5 studies of combined nicotine
vantages are the adverse effects, which include the social
replacement therapies and observed a small benefit with
stigma of squirting a spray into one’s nostrils, and that the
combination NRT (OR 1.55, CI 1.17–2.05). A recent study
drug is contraindicated in patients with reactive airway
by Hand et al48 found no benefit from combining coun-
disease.28 The Cochrane Library analysis by Silagy et al38
seling, nicotine patch, and nicotine inhaler, compared to
of 4 studies reported a 12% absolute increase in the rate of
counseling alone (15% and 14% 1-year cessation rates,
smoking cessation (OR 2.28, 1.61–3.20). The USDHSS
respectively). Conversely, Blondal et al49 found a signifi-
review of 3 studies found a higher quit rate: 16.6%.28 The
cantly higher 1-year cessation rate with nicotine patch and
difference in those cessation rate estimates may be due to
nasal spray (28% cessation rate) compared to nicotine patch
exclusion in one meta-analysis of the trial by Hjalmarson
alone (11% cessation rate). Overall, the evidence is too
et al,45 which found a 12-month cessation rate of 12%.
sparse at present to allow specific recommendations on
Evidence supporting the efficacy of nicotine nasal spray is
Regarding the dose responsiveness of NRT, the Co-
Nicotine inhaler (Nicotrol inhaler) is the fifth FDA-
chrane Collaboration analysis pooled 6 studies that used
approved NRT. The inhaler cartridge contains 10 mg of
higher doses of nicotine patch, but found only marginal
nicotine that can supply 4 mg of nicotine (2 mg are sys-
evidence of additive benefit (OR 1.2, CI 1.03–1.42).38
temically available) over 80 inhalations (suggested to take
In summary, all forms of NRT recommended by the
place over 20 min; see Table 8). Advantages of the nico-
FDA as first-line drugs are effective for smoking cessa-tion. At this time there is insufficient evidence to recom-
tine inhaler include that it mimics smoking (albeit with
mend one form of NRT over another. Patients with lesser
rapid puffing), it delivers nicotine rapidly, and it has min-
dependence on nicotine (ie, Յ 10 cigarettes/d) may con-
imal side effects. Disadvantages are that the inhaler is the
sider lower-dose or alternative interventions.28 Given the
most expensive form of NRT (average wholesale price
lack of clear-cut evidence supporting one NRT form over
$1.08 per cartridge) and requires more intense puffing than
another, patient and physician preference should play a
smoking. The Cochrane Library meta-analysis of 4 studies
large role in choosing a specific NRT drug.
demonstrated an absolute 8% increase in the cessation rateover placebo inhalers (OR 2.09, CI 1.49 –3.04).38 The meta-
Bupropion
analysis by Fiore et al28 reported a 12.3% increase in ces-sation rates with nicotine inhaler (OR 2.5, CI 1.7–3.6).
The antidepressant bupropion is the first non-NRT in-
Adverse effects reported by Hjalmarson et al46 were in-
tervention recommended by the FDA as a first-line drug
creased cough (28%) and irritation of the mouth or throat
for smoking cessation.28,39,50 The Cochrane Collaboration
(15%). With caution, because of the small number of stud-
analysis39 of 7 trials found 10% better cessation among
ies available, the evidence regarding nicotine inhalers also
those who received bupropion than among control subjects
(OR 2.54, CI 1.9 –3.41). The USDHHS Clinical Practice
Nicotine lozenge/tablet (Commit) is not an FDA-ap-
Guideline also found better cessation rate with bupropion:
proved first-line medication but does show promise. Nic-
13.2% higher than controls (OR 2.1, CI 1.5–3.0).28 With
otine lozenges (polacrilex) come in 2-mg and 4-mg doses.
regard to combined bupropion and NRT Jorenby et al51
They are easy to use, have minimal adverse effects (heart-
found significantly better cessation rates with the combi-
burn, hiccups, and nausea), and provide 25% more nico-
nation of NRT and bupropion than with nicotine patch
tine than similar doses of nicotine gum.47 In a large, ran-
alone (OR 2.07, CI 1.22–3.53 and 2.65 CI 1.58 – 4.45,
domized trial (n ϭ 1,818 smokers) concurrently conducted
in the United States and England, Shiffman et al47 found
Another observed benefit of bupropion is its ability to
an increased abstinence rate in high-dependence smokers
blunt the weight gain that may accompany smoking ces-
(receiving the 4-mg dose) of 8.7% over placebo and in
sation.50 For example, Jorenby et al51 reported that com-
low-dependence smokers (receiving the 2-mg dose) of 8.2%
bined bupropion and nicotine patch recipients experienced
over placebo. Though there are few studies reviewing nic-
a lower mean weight gain than did nonrecipients (ie, 2.1kg vs 1.1 kg at 7 wk).
otine lozenges or tablets, these medications are promising.
Overall, the evidence regarding bupropion for smoking
Despite the substantial body of supportive evidence,
there is continuing uncertainty about some aspects of NRT. For example, does the use of multiple forms of NRT en-
Second-Line Smoking Cessation Drugs
hance effectiveness? Is there a dose-response beyond theusual recommended doses? Do nicotine lozenges or tablets
Clonidine is an antihypertensive medication that is pro-
vided orally or transdermally (Catapres). In a meta-anal-
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
ysis of 6 studies, Gourlay et al40 found that clonidine in-
be done in the presence of a health care professional. Our
creased smoking cessation rate by 11% (OR 1.89, CI 1.30 –
view is that currently the evidence is insufficient to sup-
2.74). Similarly, Fiore et al28 analyzed 5 studies and reported
a similar enhanced abstinence rate: 11.7% (OR 1.4 –3.2).
The 4 available meta-analyses of alternative interven-
Unfortunately, clonidine can produce important adverse
tions fail to support efficacy in aiding smoking cessation.
events, such as dry mouth, dizziness, sedation, and pos-
For example, 2 available meta-analyses of acupuncture
tural hypotension, which may discourage its use.28,40
failed to show efficacy (OR 1.08, CI 0.77–1.52 and OR
Overall, although the evidence supporting clonidine for
1.1, CI 0.7–1.6).28,54 A meta-analysis and a recent study of
smoking cessation achieves an A rating, the adverse effect
exercise intervention with 299 smokers showed no in-
profile relegates it to second-line status. Clonidine has not
creased rate of smoking cessation.55,56 Similarly, neither a
been approved by the FDA for smoking cessation, but has
review of available studies nor an unpublished pharma-
found use as a salvage regimen with individuals who have
ceutical study of lobeline, a partial nicotine agonist, showed
Finally, nortriptyline is a tricyclic antidepressant that
The Cochrane Collaboration review58 of trials of anx-
has been used to assist smoking cessation.28,39 Results of 3
iolytics (3 trials of buspirone, 1 trial of diazepam, 1 trial of
available studies demonstrate a 12% absolute improve-
meprobamate, and 1 trial of  blockers) concluded that
ment in cessation rates over controls (OR 1.73, 1.73–
none of the trials supported efficacy for improving smok-
4.44).52 Also, the USDHHS Clinical Practice Guideline28
ing cessation. Adverse effects and the availability of other
review of 2 studies noted 18.4% improvement over control
interventions discourage the use of any of these drugs.
cessation rates (OR 3.2, 1.8 –2.7).
In a review of 2 studies of the nicotine antagonist
Overall, the limited number of trials and the adverse
mecamylamine, Lancaster et al59 found that mecamylamine
effects of nortriptyline make it a second-line intervention.
combined with nicotine patch produced better cessation
Evidence supporting the use of nortriptyline in smoking
rates than nicotine patch alone. However, lack of any long-
term studies precludes current endorsement ofmecamylamine. Similarly, the USDHHS Clinical Practice
Alternative Smoking Cessation Interventions
Guideline report did not advocate mecamylamine.28
Silver acetate is a pharmaceutical aversive therapy that
Alternative behavioral interventions for smoking cessa-
leaves an unpleasant taste in the mouth when combined
tion include hypnotherapy, aversive therapies, acupunc-
with cigarettes.60 The Cochrane Collaboration reported 2
ture, and exercise. Other medications that have been tried
studies comparing silver acetate to placebo and found no
for smoking cessation include lobeline, anxiolytics,
measurable improvement in cessation rates (OR 1.05, CI
mecamylamine, opioid agonists, and silver acetate. There
0.63–1.73). The USDHSS Clinical Practice Guidelines re-
is less supportive research for these interventions than for
view also found no benefit from silver acetate.28 In light of
current available information, we do not recommend silver
Regarding hypnotherapy, a review of 9 trials by Abbot
et al52 did not find efficacy for smoking cessation. Chal-lenges to validating hypnotherapy include the small size of
Combined Smoking Cessation Interventions
most of the trials and the confounding issue of separatingthe impact of time spent with the therapist from the hyp-
Many studies establish the superiority of combined in-
nosis itself.52 The USDHHS Clinical Practice Guideline
terventions over individual smoking cessation strategies.
For example, in the largest available trial with chronic
Aversive therapies were mainly used before current in-
obstructive pulmonary disease patients, the Lung Health
terventions became available; they include rapid smoking,
Study (n ϭ 5,887 subjects) found that the group that re-
smoke holding, rapid puffing, excessive smoking, and elec-
ceived nicotine gum and counseling (physician counseling
tric shock. The theory underlying aversive therapy is that
and group counseling) had a better smoking cessation rate
linking a negative sensation to smoking will encourage
(22% at 11 years) than the usual-care group (6%).14
cessation. Hajek and Stead53 reviewed aversive smoking
Regarding the additive effect of bupropion, Tashkin et
therapies and found rapid smoking to be the most effec-
al61 compared individual counseling plus proactive tele-
tive. However, they concluded that there was insufficient
phone calls plus bupropion to individual counseling plus
evidence to support the effectiveness of aversive therapy.
proactive telephone calls plus placebo, and found that the
In contrast, the USDHHS Clinical Practice Guideline re-
bupropion group had a higher cessation rate than the con-
ported that rapid smoking improved abstinence rates by
trol group (16% versus 9% at 26 wk, OR 1.74, CI 1.01–
8% over controls (OR 2.0, CI 1.1–3.5).28 One important
3.0). Overall, given the effectiveness of individual strate-
limitation is that, if attempted, rapid smoking should only
gies and the weight of evidence supporting combined
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
approaches, current practice often offers both counseling
interventions. Also, the paucity of available literature in-
and drug interventions to assist smoking cessation.
vites further study of RTs’ effectiveness in smoking ces-sation.
As with all medications, cost is an important issue for
smoking cessation therapy. At the same time, the cost of
Because smoking remains common and is associated
therapy must be offset against the cost associated with
with substantial morbidity, mortality, and costs, aggressive
buying cigarettes and the personal and societal costs of
efforts to eradicate smoking are justified. Of the available
sequelae of smoking. Currently, the average cost of a pack
methods to effect smoking cessation, level A evidence
of cigarettes is $3.15.62 Thus, the yearly cost of a 1 pack/
supports the efficacy of various behavioral and pharma-
day habit is $1,149.75. An estimate of the cost of medical
cologic interventions: counseling by various health care
care associated with each pack of cigarettes sold is $3.45.10
providers, nicotine replacement therapy, and bupropion. In
Additionally, the estimated cost of lost productivity due to
addition, combination therapy (eg, counseling plus nico-
morbidity and mortality from smoking add $3.73 as the
tine replacement therapy, nicotine plus bupropion) seems
societal cost per pack.10 Thus, the aggregate cost per pack
to confer additional benefit. Still, disappointing longer-
of cigarettes is $7.18. In this context the daily cost of
term abstinence rates for the strongest available studies (ie,
nicotine patches ($3.57) looks quite favorable. Table 8
Ͻ 25%) establish the need for continued investigation of
shows price estimates for the available medications.
smoking cessation strategies. Finally, we believe that RTscan and should play key roles in smoking cessation pro-
The Respiratory Therapist’s Role
grams and that this subject warrants further study. in Smoking Cessation
As both hospital-based and home-care practitioners, re-
REFERENCES
spiratory therapists (RTs) have extraordinary opportunitiesto encourage smoking cessation. The opportunity is ad-
1. US Department of Health and Human Services. Reducing tobacco
use: a report of the Surgeon General. Atlanta, Georgia: US Depart-
vanced by therapists’ favorable attitudes toward smoking
ment of Health and Human Services, Centers for Disease Control
cessation. For example, Sockrider et al63 surveyed 354
and Prevention, National Center for Chronic Disease Prevention and
RTs therapists as to whether they believed that advising
Health Promotion, Office on Smoking and Health, 2000 Surgeon
smoking cessation was a necessary aspect of their job. The
General’s Report. Available at http://www.cdc.gov/tobacco/sgr/
rating system was 5 ϭ strongly agree and 1 ϭ strongly
2. Curbing the epidemic: governments and the economics of tobacco
disagree. The mean aggregate score was 4.3. The mean
control. Developments in practice. The World Bank Group. Wash-
level of agreement that smoking cessation should be in-
cluded in training was 3.4 and that cessation advice was as
3. Centers for Disease Control and Prevention. Achievements in public
important as other aspects of an RT’s job was 3.6.63
health, 1900–1999: tobacco use—United States, 1900–1999. MMWR:
Despite the opportunity and the favorable attitude, the
Nov 05. 1999;48(43):986–993. Available at http://www.cdc.gov/mmwr (accessed 10/2/03).
subject of RTs’ effectiveness in conducting smoking ces-
4. Center for Disease Control and Prevention. Percentage of adults who
sation interventions has received little attention, with only
were current, former, or never smokers, overall and by sex, race,
2 studies identified in our literature search.
Hispanic origin, age and education. National Health Interview Sur-
In a randomized trial reported by Stevens et al,64 in
veys, selected years- United States, 1965–2000. Tobacco Informa-
which RTs provided counseling, no difference in cessation
tion and Prevention Source (TIPS). Apr 11, 2003. Available at http://www.cdc.gov/tobacco/research_data/adults_prev/adstat1.htm
rates was observed between the group receiving RT coun-
seling and the usual-care group (14.2% and 13.6%, respec-
5. Center for Disease Control and Prevention. Prevalence of current
tively). One possible explanation for RTs’ lack of impact
cigarette smoking among adults and changes in prevalence of current
in the study was the time constraints that limit RTs’ in-
and some day smoking—United States, 1996–2001, MMWR. Apr
terventions.64 For example, only 68% of those randomized
11, 2003;52(14):303–307. Available at http://www.cdc.gov/mmwr(accessed 10/2/03).
to RT intervention were seen by the RT (vs 80% contacted
6. Center for Disease Control and Prevention. Ten great public health
by a professional counselor in another study) and only
achievements in the 20th century. 1900–1999. Office of Communi-
71% received telephone contact from the RT (vs 99% in
cation. Media Relations. Sep 13, 2001. Available at http://www.
another study with professional counselors).64 Cohn et al65
cdc.gov/od/oc/media/tengpha.htm (accessed 10/2/03).
reported an impressive 48% 6-week abstinence rate among
7. U.S. Department of Health and Human Services. Office of Applied
Studies, Substance, Abuse and Mental Health Services Administra-
participants in an RT-led smoking cessation program.
tion (SAMHSA). Tobacco use, income, and educational level. The
Overall, we conclude that RTs’ access to smokers makes
NHSDA Report. May 3, 2002. Available at http://www.samhsa.gov/
them attractive candidates to administer smoking cessation
oas/2k2/Tob/tob.htm (accessed 10/11/03).
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
8. Center for Disease Control and Prevention. Women and smoking, a
22. Dani JA, Ji D, Zhou FM. Synaptic plasticity and nicotine addiction.
report of the Surgeon General-2001. Pattern of tobacco use among
women and girls-fact sheet. Tobacco Information and Prevention
23. Corrigall WA, Coen KM. Selective dopamine antagonist reduce nic-
Source (TIPS). Mar 27, 2001. Available at http://www.cdc.gov/
otine self-administration. Psychopharmacology 1991;104:171–176.
tobacco/sgr/index.htm (accessed 10/2/03).
24. Corrigal WA, Coen KM & Adamson KL. Self–administered nicotine
9. Center for Disease Control and Prevention. Trends in cigarette smok-
activates the mesolimbic dopamine system through the ventral teg-
ing among high school students—United States 1991–2001. MMWR
mental area. Brain Res 1994;653:278–284.
25. Hughes JR, Higgins ST, Bickel WK. Nicotine withdrawal versus
preview/mmwrhtml/mm5119a1.htm (accessed 10/2/03).
other drug withdrawal syndromes: similarities and dissimilarities.
10. Center for Disease Control and Prevention. Annual smoking-attrib-
Addiction. 1994;(Nov):89(11):1461–1470.
utable mortality, years of potential life lost, and economic costs—
26. Heatherton TF, Kozlowski LT, Frecker RC, Fagerstrom KO. The
United States, 1995–1999. MMWR. Apr 12, 2002;51(14):300–303.
Fagerstrom test for nicotine dependence: a revision of the Fager-
Available at http://www.cdc.gov/mmwr/preview/mmwrhtml/
strom tolerance questionnaire. Br J Addict 1991;86(9):1119–1127.
27. Center for Disease Control and Prevention. Cigarette smoking among
11. Centers for Disease Control and Prevention. Smoking attributable
adults–United States, 2000. MMWR Highlights. Jul 26, 2002;51;29:
mortality, morbidity, and economic costs (SAMMEC): Adult
642–645. Available at http://www.cdc.gov/mmwr/ (accessed 10/7/
SAMMEC and Maternal and Child Health (MCH) SAMMEC soft-
ware, 2002c. Available at: http://www.cdc.gov/tobacco/sammec (ac-
28. Fiore, MC, Bailey WC, Cohen SJ, et al. Treating tobacco use and
dependence. Clinical Practice Guideline. Rockville, MD: U.S. De-
12. US Department of Health and Human Services. The health benefits
partment of Health and Human Services. Public Health Service. Jun
of smoking cessation: a report of the Surgeon General. Atlanta,
2000. Available at http://www.surgeongeneral.gov/tobacco/
Georgia: US Department of Health and Human Services, Centers for
Disease Control and Prevention, National Center for Chronic Dis-
29. Silagy C, Stead LF. Physician advice for smoking cessation. Co-
ease Prevention and Health Promotion, Office on Smoking and Health,
chrane Database Syst Rev 2001;(2):CD000165.
DHHS Publication No. (CDC) 90–8416.1990. Available at http://
30. Denny CH, Serdula MK, Holtzman D, Nelson DE. Physician advice
www.cdc.gov/tobacco/sgr/index.htm (accessed 10/2/03).
about smoking and drinking: are U.S. adults being informed? Am J
13. Buist AS, Connett JE, Miller RD, Kanner RE, Ownes GR, Voelker
HT. Chronic Obstructive Pulmonary Disease Early Intervention Trial
31. Rice VH, Stead LF. Nursing interventions for smoking cessation.
(Lung Health Study). Baseline characteristics of randomized partic-
Cochrane Database Syst Rev 2001;(3):CD001188.
ipants. Chest 1993;103(6):1863–1872.
32. Lancaster T, Stead LF. Individual behavioural counselling for smok-
14. Anthonisen NR, Connett JE, Murray RP. Smoking and lung function
ing cessation. Cochrane Database Syst Rev 2002;(3):CD001292.
of Lung Health Study participants after 11 years. Am J Respir Crit
33. Stead LF, Lancaster T. Group behaviour therapy programmes for
smoking cessation. Cochrane Database Syst Rev 2002;(3):CD001007.
15. US Department of Health and Human Services. Reducing the health
34. Stead LF, Lancaster T, Perara R. Telephone counseling for smoking
consequences of smoking: a report of the Surgeon General. Atlanta,
cessation. Cochrane Database Syst Rev 2003;(1):CD002850.
Georgia: US Department of Health and Human Services, Centers for
35. Ossip-Klein DJ, Giovino GA, Megahed N, Black PM, Emont SL,
Disease Control and Prevention, National Center for Chronic Dis-
Stiggins J, et al. Effects of a smoker’s hotline: results of a 10-county
ease Prevention and Health Promotion, Office on Smoking and Health,
self-help trial. J Consult Clin Psychol 1991;59(2):325–332.
1964 Surgeon Generals Report: pg 34. Available at http://www.
36. Lancaster T, Stead LF. Self-help interventions for smoking cessa-
cdc.gov/tobacco/sgr/index.htm (accessed 10/2/03).
tion. Cochrane Database Syst Rev 2002;(3):CD001118.
16. US Department of Health and Human Services. Smoking and health:
37. Simon JA, Carmody TP, Hudes ES, Snyder E, Murray J. Intensive
a report of the Surgeon General. Atlanta, Georgia: US Department of
smoking cessation counseling versus minimal counseling among hos-
Health and Human Services, Centers for Disease Control and Pre-
pitalized smokers treated with transdermal nicotine replacement: a
vention, National Center for Chronic Disease Prevention and Health
randomized trial. Am J Med 2003;114(7):555–562.
Promotion, Office on Smoking and Health, 1979 Surgeon Generals
38. Silagy C, Lancaster T, Stead L, Mant D, Fowler G. Nicotine replace-
Report. Pg xv. Available at http://www.cdc.gov/tobacco/sgr/
ment therapy for smoking cessation. Cochrane Database Syst Rev
17. US Department of Health and Human Services. Health consequences
39. Hughes JR, Stead LF, Lancaster T. Antidepressants for smoking
of smoking: nicotine addiction: a report of the Surgeon General.
cessation. Cochrane Database Syst Rev 2003;(2):CD000031.
Atlanta, Georgia: US Department of Health and Human Services,
40. Gourlay SG, Stead LF, Benowitz NL. Clonidine for smoking cessa-
Centers for Disease Control and Prevention, National Center for
tion. Cochrane Database Syst Rev 2000;(2):CD000058.
Chronic Disease Prevention and Health Promotion, Office on Smok-
41. Johnston AJ, Ascher J, Leadbetter R, Schmith VD, Patel DK,
ing and Health, 1988 Surgeon Generals Report. Pg ii. Available at
Durcan M, Bentley B. Pharmacokinetic optimization of sustained-
http://www.cdc.gov/tobacco/sgr/index.htm (accessed 10/2/03).
release bupropion for smoking cessation. Drugs 2002;62 Suppl
18. Pidoplichko VI, DeBiasi M, Williams JT, Dani JA. Nicotine acti-
vates and desensitizes midbrain dopamine neurons. Nature 1997;
42. Prochazka AV. New developments in smoking cessation. Chest 2000;
19. Leshner AI, Koob GF. Drugs of abuse and the brain. Proc Assoc Am
43. Pierce JP, Gilpin EA. Impact of over-the-counter sales on effective-
ness of pharmaceutical aids for smoking cessation. JAMA 2002;
20. Clark PB. Mesolimbic dopamine activation—the key to nicotine
reinforcement? Ciba Found Symp 1990;152:153–162: discussion
44. Murray RP, Bailey WC, Daniels K, Bjornson WM, Kurnow K, Con-
nett JE, et al. Safety of nicotine polacrilex gum used by 3,094 par-
21. Dani JA, De Biasi M. Cellular mechanisms of nicotine addiction.
ticipants in the Lung Health Study. Lung Health Study Research
Pharmocol Biochem Behav 2001;70(4) 439–446.
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
45. Hjalmarson A, Franzon M, Westin A, Wiklund O. Effect of nicotine
controlled trial. Addiction 2003;98(4):523–532.
nasal spray on smoking cessation: a randomized, placebo-controlled,
56. Ussher MH, West R, Taylor AH, McEwen A. Exercise interventions for
double-blind study. Arch Int Med 1994;154(22):2567–2572.
smoking cessation. Cochrane Database Syst Rev 2000;(3):CD002295.
46. Hjalmarson A, Nilsson F, Sjostrom L, Wiklund O. The nicotine inhaler
57. Stead LF, Hughes JR. Lobeline for smoking cessation. Cochrane
in smoking cessation. Arch Int Med 1997;157(15).1721–1728.
Database Syst Rev 2000;(2):CD000124.
47. Shiffman S, Dresler CM, Hajek P, Gilburt SJ, Targett DA, Stahs KR.
58. Hughes JR, Stead LF, Lancaster T. Anxiolytics for smoking cessa-
Efficacy of a nicotine lozenge for smoking cessation. Arch Int Med
tion. Cochrane Database Syst Rev 2000;(4):CD002849.
59. Lancaster T, Stead LF. Mecamylamine (a nicotine antagonist) for
48. Hand S, Edwards S, Campbell IA, Cannings R. Controlled trial of
smoking cessation. Cochrane Database Syst Rev 2000;(2):CD001009.
three weeks nicotine replacement treatment in hospital patients also
60. Lancaster T, Stead LF. Silver acetate for smoking cessation. Co-
given advice and support. Thorax; 2002;57(8):715–718.
chrane Database Syst Rev 2000;(2):CD000191.
49. Blondal T, Gudmundsson LJ, Olafsdottir I, Gustavsson G, Westin A.
61. Tashkin D, Kanner R, Bailey W, Buist S, Anderson P, Nides M, et
Nicotine nasal spray with nicotine patch for smoking cessation: ran-
al. Smoking cessation in patients with chronic obstructive pulmonary
domised trial with six year follow up. BMJ 1999;318(7179):285–
disease: a double-blind, placebo-controlled, randomized trial. Lancet
288. Erratum in BMJ 1999;318(7186):764
50. Jorenby D. Clinical efficacy of bupropion in management of smok-
62. Center for Disease Control and Prevention. Office of Smoking and
ing cessation. Drugs 2002;62 Suppl 2:25–35.
Health, National Center for Chronic Disease Prevention and Health
51. Jorenby DE, Leischow SJ, Nides MA, Rennard SI, Johnston JA,
Promotion. State Tobacco Activities Tracking and Evaluation
Hughes AR, et al. A controlled trial of sustained-release bupropion,
(STATE). 2000. Available at http://www2.cdc.gov/nccdphp/osh/state
a nicotine patch, or both for smoking cessation. N Engl J Med
63. Sockrider MM, Maguire GP, Haponik E, Davis A, Boehlecke B.
52. Abbot NC, Stead LF, White AR, Barnes J, Ernst E. Hypnotherapy
Attitudes of respiratory care practitioners and students regarding
forsmoking cessation. Cochrane Database Syst Rev 2000;(2):
pulmonary prevention. Chest 1998;114(4):1193–1198.
64. Stevens VJ, Glasgow RE, Hollis JF, Mount K. Implementation and
53. Hajek P, Stead LF. Aversive smoking for smoking cessation. Co-
effectiveness of a brief smoking-cessation intervention for hospital
chrane Database Syst Rev 2000;(2):CD000546.
patients. Med Care 2000;38(5):451–459.
54. White AR, Rampes H, Ernst E. Acupuncture for smoking cessation.
65. Cohn RC, Dodson D, French A, Ervin B, Ciarlariello S, Wilson TN.
Cochrane Database Syst Rev 2002;(2):CD000009.
A pilot smoking cessation program run by pediatric respiratory
55. Ussher M, West R, McEwen A, Taylor A, Steptoe A. Efficacy of
care practitioners for parents. Clin Pediatr (Phila) 2000;39(2):121–
exercise counseling as an aid for smoking cessation: a randomized
Discussion
bacco use. I think it’s called price elas-
2. Lewitt EM, Coate D. The potential for using
excise taxes to reduce smoking. J Health Econ
MacIntyre: MacIntyre:
dicate that as you raise cigarette taxes,
MacIntyre:
their cigarettes by the carton, they’re
ing the tax increase is the smugglers.
there. We chose to limit this report just
have a very low tax and they haulcigarettes off to New York and sell
Mannino: REFERENCES
1. Ross H, Chaloupka FJ. The effect of ciga-
rette prices on youth smoking. Health Econ
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
Heffner:
because that’s all we had back then. Stoller:
solute reduction rates; they’re not per-
that might justify the intervention. REFERENCE
1. Silagy C, Lancaster T, Stead L, Mant D,
Fowler G. Nicotine replacement therapy for
smoking cessation. Cochrane Database Syst
Heffner:
vices’ smoking cessation indicators. Stoller: Heffner: REFERENCE REFERENCE
1. Pierson DJ. The future of respiratory care.
Davis A, Boehlecke B. Attitudes of respira-
tory care practitioners and students regard-ing pulmonary prevention. Chest 1998;
Mannino: Enright:
ple don’t smoke in the first place.
is added to the baseline cessation rate.
ers receive an “attaboy”-type compli-
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
tioned prices; typically, increased taxes
sation, but in hospitals they don’t do a
sibly, some of those external factors are
Mannino:
there are 3 things that have worked, both
available in our health care system.
from starting. One is to increase the price
everyone to get involved in their com-munities and support ordinances to limit
Enright:
tucky, in the heart of tobacco country, is
public places. Yet in Europe it’s still
is hard-hitting anti-smoking advertising:
have been pretty good models for that.
What we know doesn’t work are those
not to sell cigarettes to kids. That just
Wedzicha:
after the other, and it’s usually a mat-
ing to obtain. They don’t really work. Shrake:* Pierson:
certainly by far the major interven-
Operating Officer, American Association forRespiratory Care, Dallas, Texas.
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
Bulgarian Chemistry and Industry, 74, No 4 ( 2003 ) 118–119 CONTENTS FOR VOLUME 74 G. VISSOKOV: Nanoscience and nanotechnology research directions in chemical industries . 1H.-J. BART, D. KAMENSKI: Modelling the kinetics of the reactive solvent extraction of zinc withZH. BALGARANOVA, L. PHILLIPOV: Stabilisation of aniline by addition of hydrazine .19G. N. VASSILEV: Synthesis, chemical
www.abbeyvetservices.co.uk/newsletters/oct07.htmA Case of a Nictitans Gland Carcinoma in a Cat • Latest news • Case of interest • Our Details • Biopsy tips • Side Story • Journal Articles A seven-year-old domestic short haired cat presented with a protruding mass from the third • Site Downloads eyelid of the left orbit but also involving the upper and lower eyelid. The
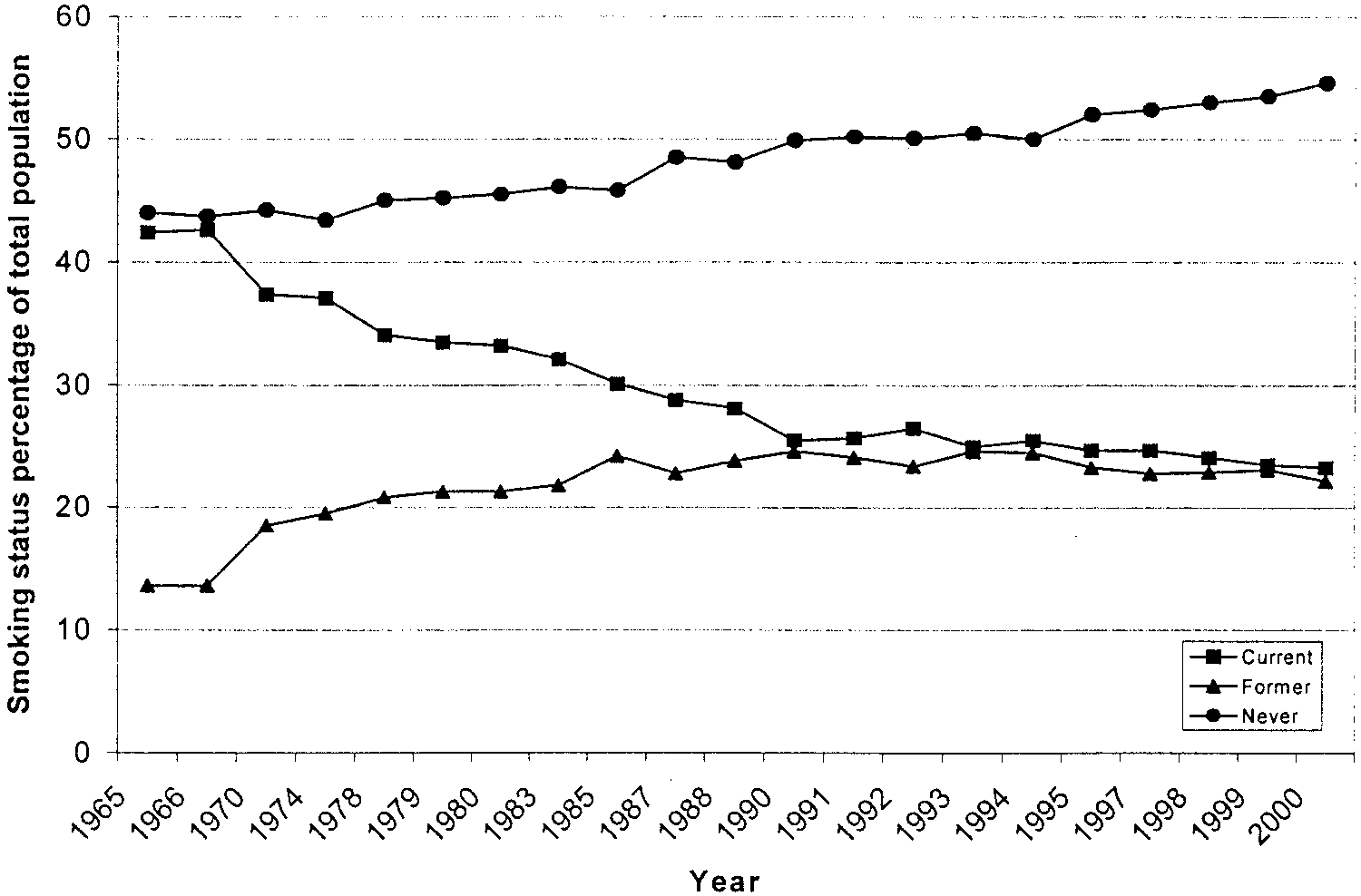 Fig. 1. Percentage of adult current, former, and never smokers. (Adapted from Reference 4.)
Introduction
Fig. 1. Percentage of adult current, former, and never smokers. (Adapted from Reference 4.)
Introduction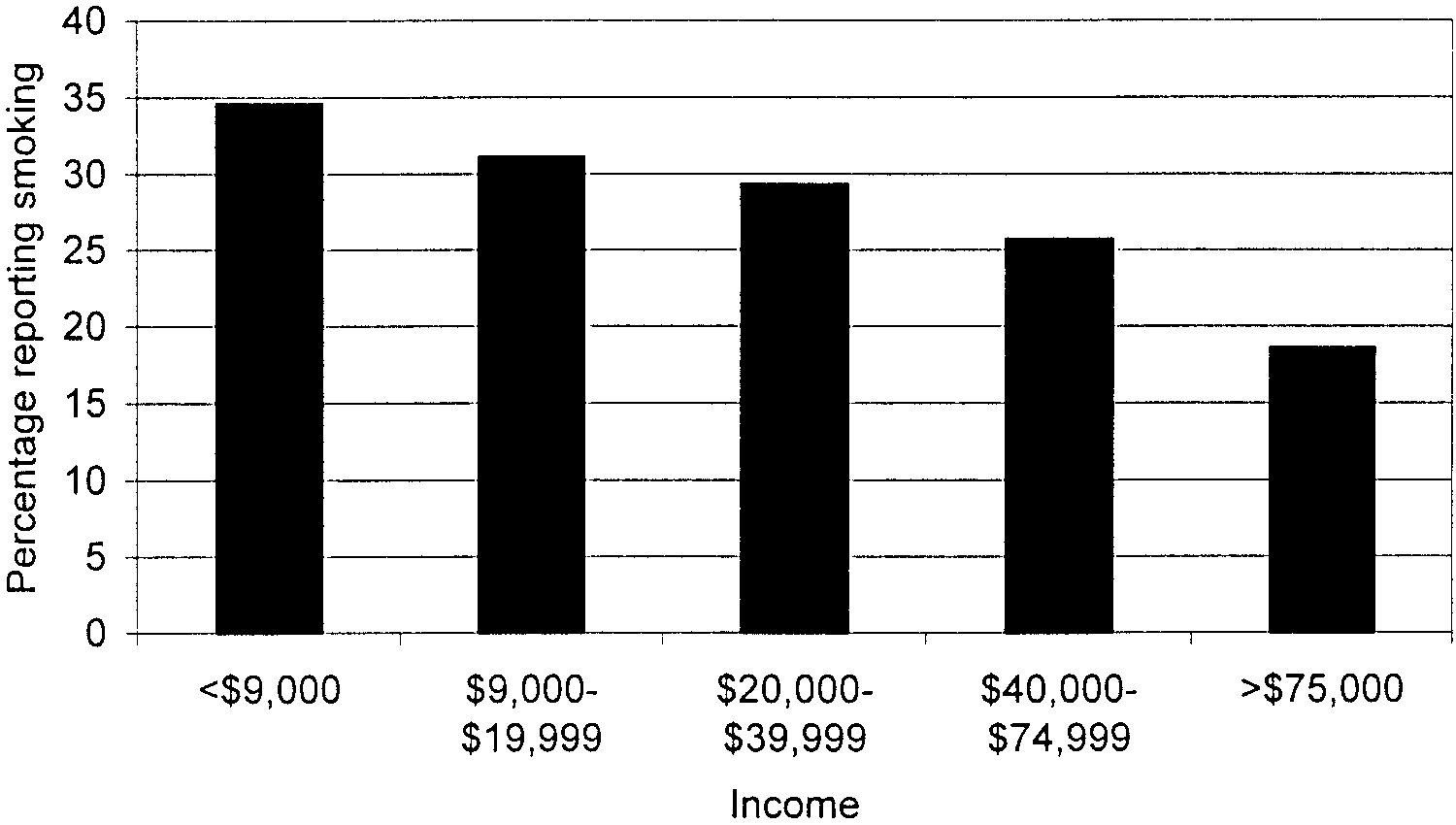
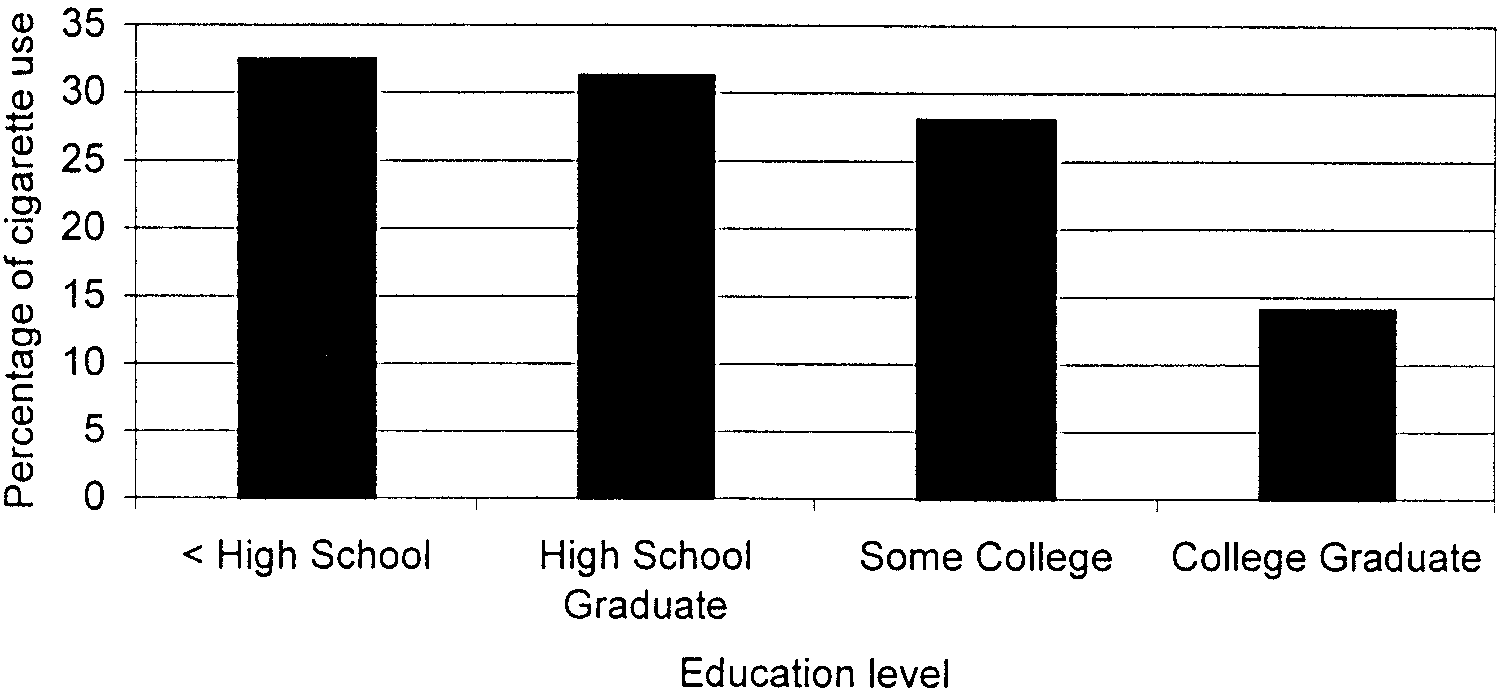 Fig. 2. Percentage of people Ն 18 years old who reported smoking in the past month, by combinedtotal family income, 1999 –2000. (Adapted from Reference 7.)
Fig. 3. Percentage of people Ն 18 years old who reported smoking in the past month, by educationlevel, 1999 –2000. (Adapted from Reference 7.)
1990s to a peak of 36.4% in 1997 and since decreased
smoking.10 Smoking also increases the risk of death in
to 28.5% in 2001 (29.2% among boys versus 27.7%
many illnesses. Table 1 shows the relative risk of smok-
ing-attributable morbidity and mortality from various con-
Because smoking is common, the economic impact is
ditions, largely including respiratory, cardiovascular, and
profound. In 1998 the direct medical cost of smoking
neoplastic diseases.11 Table 2 shows estimates of the num-
was estimated to be $75.5 billion, with productivity
ber of deaths attributed to smoking. Notably, the 35,053
losses estimated at $82 billion and smoking-related neo-
second-hand-smoke-related deaths are not included in those
natal costs estimated at $366 million.10 When all ex-
penses are combined, they represent a total of $3,391
Smoking confers a risk of serious illness, and smoking
per smoker per year, which amounts to approximately
cessation offers health benefits, which is evident in Table
8% of all annual health care expenditures in the United
1: former smokers have lower relative risk of death in all
disease categories.11 For example, compared to never-
The morbidity and mortality attributed to smoking are
smokers, men who are current or former smokers have a
also substantial. For example, between 1995 and 1999
higher relative risk of death from cancer of the trachea,
approximately 440,000 deaths annually were attributed to
lung, or bronchus (23.26 times higher in current smokers
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
Relative Risk of Death: Current Smokers Versus Former
decline (30.2 mL/y among men and 21.5 mL/y amongwomen) than active smokers (66 mL/y among men and
and 8.7 times higher in former smokers).11 The 1990 re-
port of the United States Surgeon General on the healthbenefits of smoking cessation concluded that people who
Nicotine Addiction
Fig. 2. Percentage of people Ն 18 years old who reported smoking in the past month, by combinedtotal family income, 1999 –2000. (Adapted from Reference 7.)
Fig. 3. Percentage of people Ն 18 years old who reported smoking in the past month, by educationlevel, 1999 –2000. (Adapted from Reference 7.)
1990s to a peak of 36.4% in 1997 and since decreased
smoking.10 Smoking also increases the risk of death in
to 28.5% in 2001 (29.2% among boys versus 27.7%
many illnesses. Table 1 shows the relative risk of smok-
ing-attributable morbidity and mortality from various con-
Because smoking is common, the economic impact is
ditions, largely including respiratory, cardiovascular, and
profound. In 1998 the direct medical cost of smoking
neoplastic diseases.11 Table 2 shows estimates of the num-
was estimated to be $75.5 billion, with productivity
ber of deaths attributed to smoking. Notably, the 35,053
losses estimated at $82 billion and smoking-related neo-
second-hand-smoke-related deaths are not included in those
natal costs estimated at $366 million.10 When all ex-
penses are combined, they represent a total of $3,391
Smoking confers a risk of serious illness, and smoking
per smoker per year, which amounts to approximately
cessation offers health benefits, which is evident in Table
8% of all annual health care expenditures in the United
1: former smokers have lower relative risk of death in all
disease categories.11 For example, compared to never-
The morbidity and mortality attributed to smoking are
smokers, men who are current or former smokers have a
also substantial. For example, between 1995 and 1999
higher relative risk of death from cancer of the trachea,
approximately 440,000 deaths annually were attributed to
lung, or bronchus (23.26 times higher in current smokers
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
Relative Risk of Death: Current Smokers Versus Former
decline (30.2 mL/y among men and 21.5 mL/y amongwomen) than active smokers (66 mL/y among men and
and 8.7 times higher in former smokers).11 The 1990 re-
port of the United States Surgeon General on the healthbenefits of smoking cessation concluded that people who
Nicotine Addiction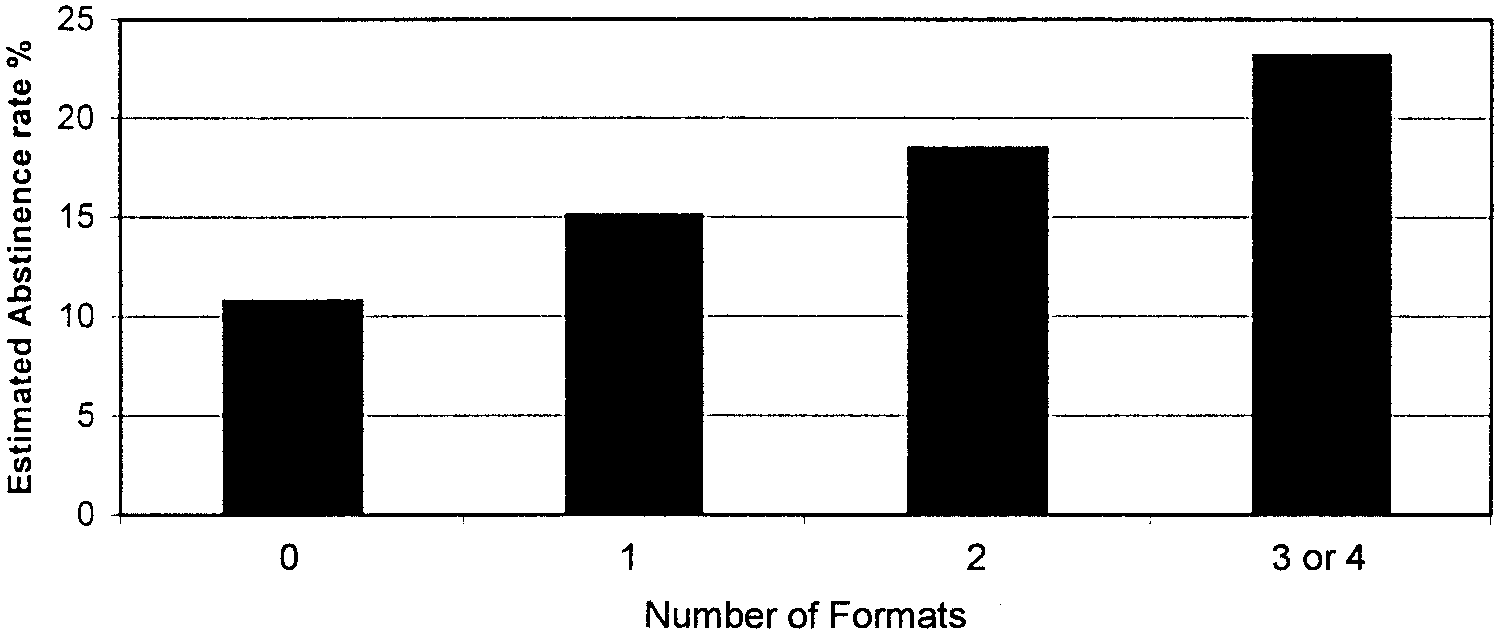
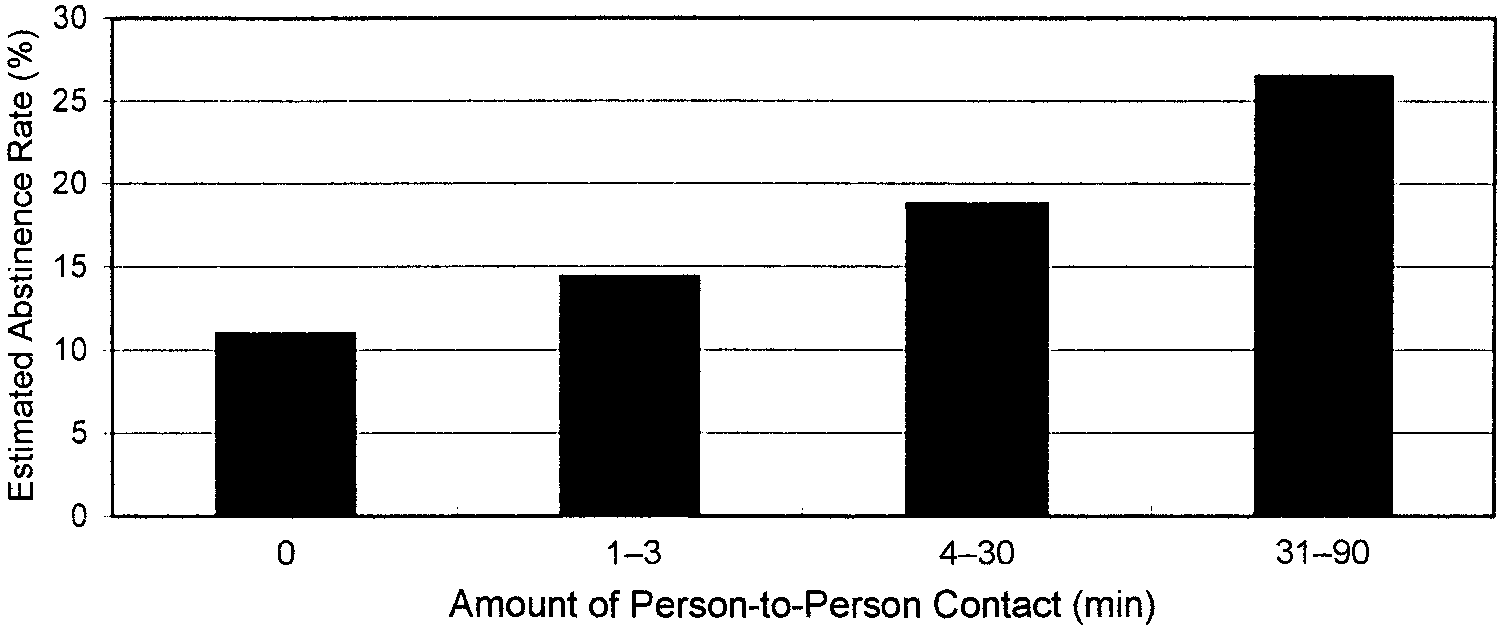
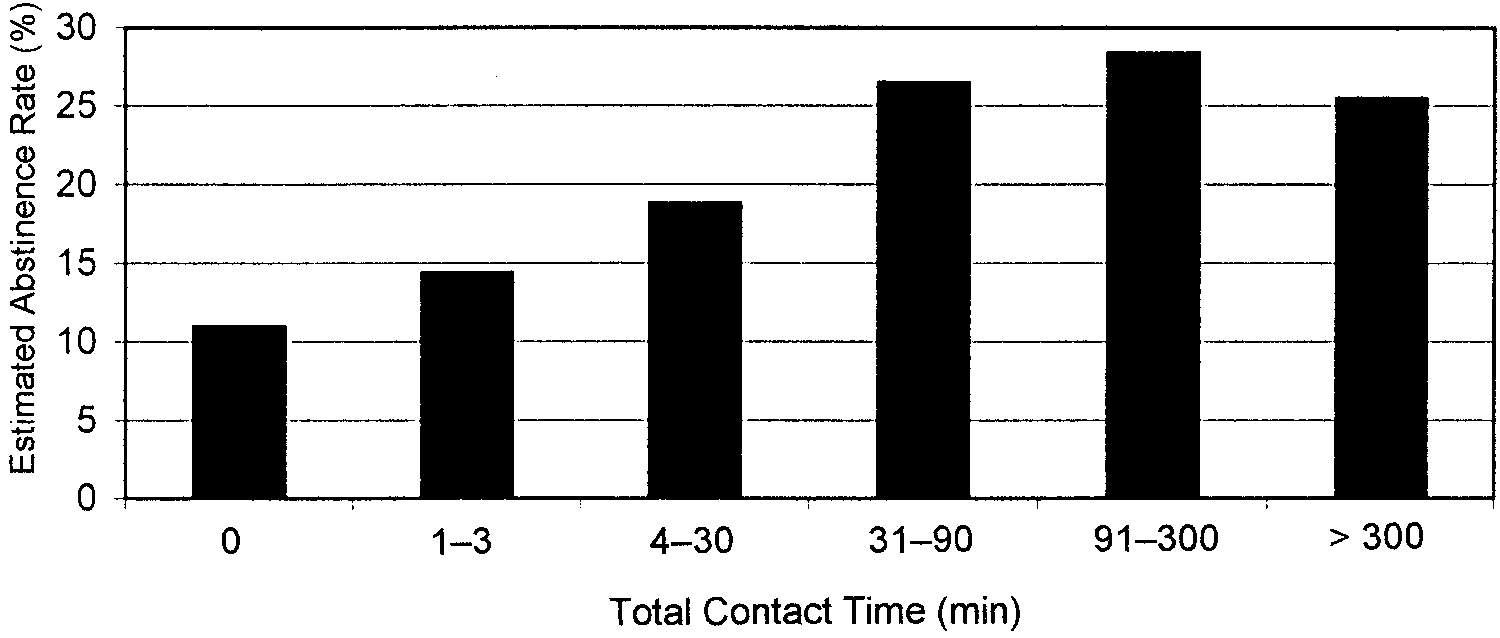 Fig. 4. Meta-analysis of estimated cigarette-smoking abstinence rates relative to number of smokingcessation formats used. The formats included self-help, proactive counseling, group counseling, andindividual counseling (n ϭ 54). (Adapted from Reference 28.)
Fig. 5. Estimated cigarette-smoking abstinence rates relative to the duration of the individual coun-seling session (n ϭ 43 studies). (Adapted from Reference 28.)
Fig. 6. Meta-analysis of estimated cigarette-smoking abstinence rates relative to the total amount ofcontact time (n ϭ 35 studies). (Adapted from Reference 28.)
considered low intensity if Յ 10 min and high intensity
with one follow-up.28 Based on these definitions, increased
if Ͼ 10 min with a follow-up appointment,30 whereas phy-
intensity of nursing intervention did not significantly in-
sician interventions were defined as minimal intensity if Յ
crease cessation rates (low intensity OR 1.67, CI 1.14 –
20 min with one follow-up visit and intensive if Ͼ 20 min
2.45, high intensity OR 1.47, CI 1.26 –1.72),30 whereas
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
Fig. 4. Meta-analysis of estimated cigarette-smoking abstinence rates relative to number of smokingcessation formats used. The formats included self-help, proactive counseling, group counseling, andindividual counseling (n ϭ 54). (Adapted from Reference 28.)
Fig. 5. Estimated cigarette-smoking abstinence rates relative to the duration of the individual coun-seling session (n ϭ 43 studies). (Adapted from Reference 28.)
Fig. 6. Meta-analysis of estimated cigarette-smoking abstinence rates relative to the total amount ofcontact time (n ϭ 35 studies). (Adapted from Reference 28.)
considered low intensity if Յ 10 min and high intensity
with one follow-up.28 Based on these definitions, increased
if Ͼ 10 min with a follow-up appointment,30 whereas phy-
intensity of nursing intervention did not significantly in-
sician interventions were defined as minimal intensity if Յ
crease cessation rates (low intensity OR 1.67, CI 1.14 –
20 min with one follow-up visit and intensive if Ͼ 20 min
2.45, high intensity OR 1.47, CI 1.26 –1.72),30 whereas
RESPIRATORY CARE • DECEMBER 2003 VOL 48 NO 12
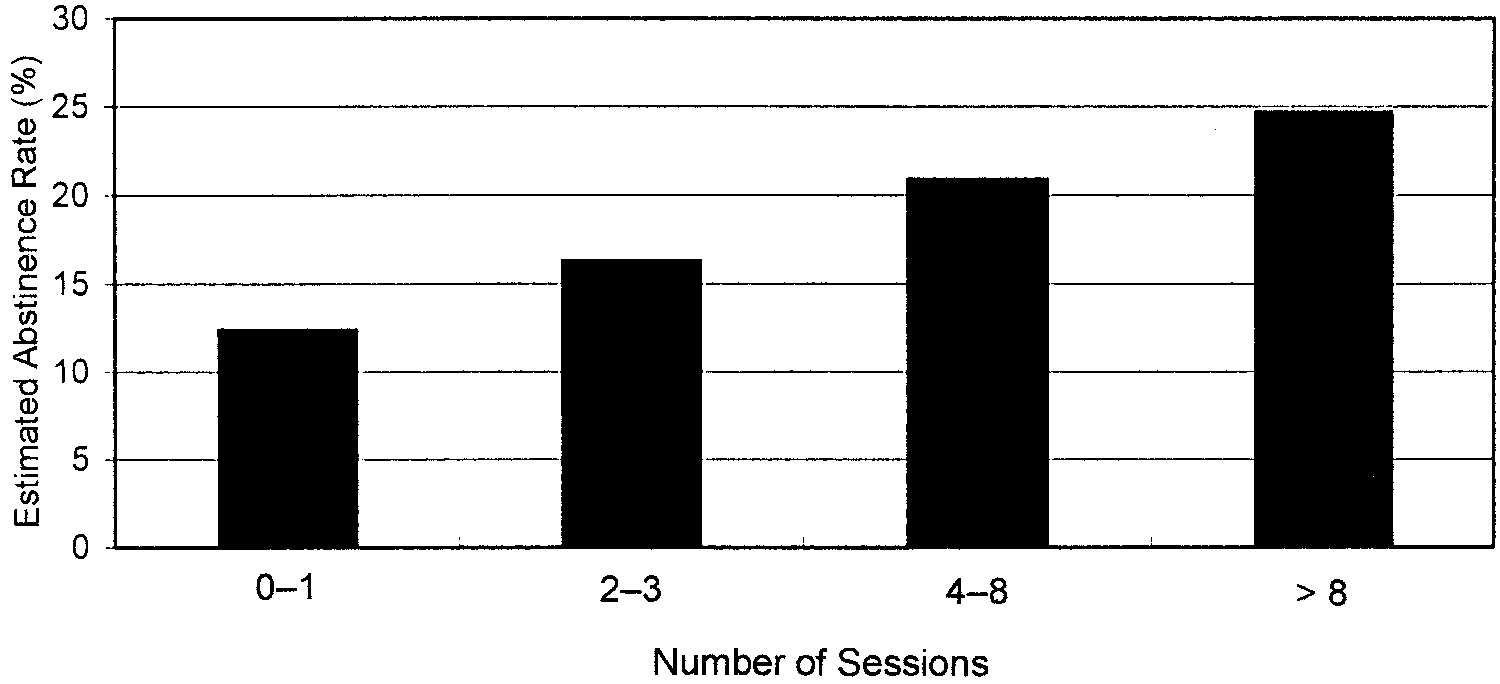 Fig. 7. Estimated cigarette-smoking abstinence rates relative to the number of counseling sessions(n ϭ 43 studies). (Adapted from Reference 28.)
increasing intensity of physician intervention did modestly
cations assist in smoking cessation, and some are available
increase the smoking cessation rate (OR 1.67, CI 1.45–
over-the-counter, caution is advised not to overestimate
1.98).28 In contrast, in an analysis of 3 trials involving
their efficacy and undermine the power of will in quitting.
Fig. 7. Estimated cigarette-smoking abstinence rates relative to the number of counseling sessions(n ϭ 43 studies). (Adapted from Reference 28.)
increasing intensity of physician intervention did modestly
cations assist in smoking cessation, and some are available
increase the smoking cessation rate (OR 1.67, CI 1.45–
over-the-counter, caution is advised not to overestimate
1.98).28 In contrast, in an analysis of 3 trials involving
their efficacy and undermine the power of will in quitting.