Kamagra enthält Sildenafilcitrat als pharmakologisch aktiven Bestandteil. Dieser hemmt selektiv die Phosphodiesterase-5 und erhöht dadurch die Konzentration von cGMP im Corpus cavernosum. Der Effekt ist zeitlich begrenzt, da die Halbwertszeit von Sildenafil etwa vier Stunden beträgt. In der galenischen Form als Mundgel erfolgt die Resorption besonders rasch, was zu einem schnelleren Wirkeintritt führt. Der Abbau erfolgt überwiegend hepatisch über CYP3A4, wobei ein aktiver Metabolit entsteht, der zur Gesamtwirkung beiträgt. Typische Nebenwirkungen ergeben sich aus der Vasodilatation, darunter leichte Kopfschmerzen und nasale Kongestion. In klinischen Beschreibungen wird kamagra oral jelly im Zusammenhang mit der schnelleren Absorption erwähnt.
Microsoft word - hf fact sheet - final
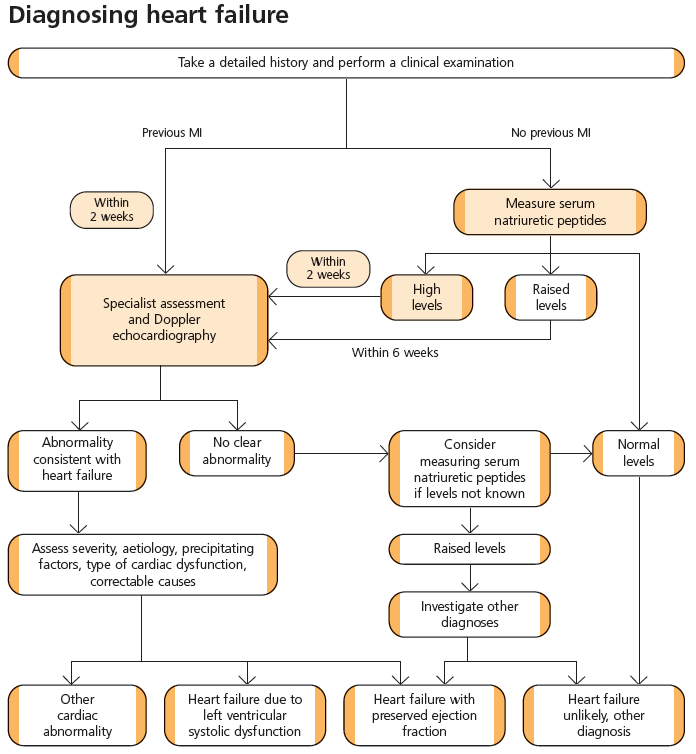
Symptoms and signs of heart failure Other investigations:
Signs: tachycardia, displaced apex, gallop rhythm, elevated
JVP, leg and sacral oedema, hepatomegaly. ascites.
Serum natriuretic peptides: Expensive test, please do not use as breathlessness screen !
NTPro-BNP High > 2000 pg/ml (236pmol/l) > 400 pg/ml (>116 pmol/l) Raised 400-2000 pg/ml (47-236pmol/l) 100-400pg/ml (29-116 pmol/l) Normal < 400pg/ml (47pmol/l)
Other causes of elevated BNP/NT-BNP include ischaemia, tachycardia, LVH and chronic renal failure. BNP may be normal in very well controlled heart failure.
Differential diagnoses to consider: Aetiology
Drug induced ankle swelling esp calcium ch blockers
NYHA Classification I no limitations, no symptoms with ordinary physical activity II slight limitation, symptoms with ordinary activity III marked limitation, symptoms with less than ordinary activity IV breathless at rest, any physical activity increases symptoms Symptoms: dyspnoea, fatigue, palpitations Diastolic HF (Heart Failure with Preserved Ejection Fraction - HFPEF) Just because LV function is normal, doesn’t mean it isn’t heart failure but only consider if HF-PEF if BNP elevated. Due to reduced ventricular filling in diastole eg
References: NICE Chronic Heart Failure August 2010, NICE Cardiac Resynchronisation Therapy 2007; Map of Medicine.
stiff ventricle or loss of atrial kick in AF. Typical picture is elderly hypertensive with
Timing recommendations may vary according to local circumstances but should be an aspiration.
fluid retention. Difficult to diagnose, echocardiogram may show ‘diastolic markers’
Further references available on request. This isn’t perfect, there are bits missing; there is only so much you can fit on
or left ventricular hypertrophy but absence of these doesn’t necessarily rule it out.
one sheet of A4. Comments please andrew.gallagher@gp-P81056.nhs.uk ; Dr.Seed@bfwhospitals.nhs. uk Oct 2010
Drug Treatment for Heart Failure Due to LVSD ACE inhibitors •
Start low and titrate upwards at intervals of every 2 weeks
Measure urea, creatinine and electrolytes with each dosage increment
Up-titration to be limited by symptomatic low blood pressure and renal function only if creatinine increases by > 50% or to > 200mmol/l.
Beta-blockers •
‘Start low and go slow’, dosage increments every 2-4 weeks
Monitor P, BP and clinical status after each titration
Warn patients that they may experience transient mild symptomatic deterioration but should improve with continued treatment
Switch stable patients on βB for co-morbidty to a βB licensed for heart failure, 50mg of atenolol is approx equivalent to 10mg bisoprolol
Up-titration to be limited by symptomatic low blood pressure or by bradycardia (if symptomatic or heart rate < 50)
Most patients with COPD without reversibility will tolerate
Effective and safe in elderly, PVD, DM, ED.
Aldosterone antagonists •
Option if symptomatic in spite of optimised treatment esp in NYHA III-IV
Monitor renal profile at 1w, 1m and every 6m if on ACEI/ARB
Consider as alternative to ACEI if intolerant
Consider addition to ACEI if unable to take βB, care with renal function!
On specialist advice in addition to ACEI and βB if persistent symptoms
ACEI+βB+ either ARB or aldosterone antagonist, NOT both
Digoxin •
Usual dosage 125mcg; no need to monitor levels
Aspirin • Target doses Ramipril
Candesartan 32 mg daily Nebivolol 10mg daily
Monitoring Monitor all patients. Include: •
Clinical assessment of functional capacity, fluid status, cardiac rhythm (min at least pulse), cognitive status and nutritional status
Re-iterate lifestyle advice especially diet, exercise, smoking
Lifestyle advice Drugs to avoid CRT (resynchronisation pacing +/- ICD)
Review of drug treatment include need to change and monitoring for
* Broad QRS and low EF = HIGH risk* Exercise: encourage regular exercise within
Minimum of urea, electrolytes, creatinine, eGFR
Monitor at short intervals (days to 2 weeks) if clinical condition or drug
Diet: encourage salt free diet
treatment has changed, otherwise monitor at least 6 monthly.
Smoking: strongly advise patients not to smoke Alcohol: advise patients with alcohol related Diastolic heart failure/HF-PEF Palliative Care phase if….
are referred to a HF specialist for treatment
optimisation and consideration of device
Sexual activity: be prepared to discuss
Currently no trial evidence for ACEIs or
Vaccination: offer annual vaccination against
beta blockers but look for an excuse to use
NB. CRT without ICD is relatively cheap and
has significant short term symptom benefit as
well as mortality benefit , often appropriate
Driving: consult DVLA guideline re HGV/PSV
in the elderly. …….please check QRS duration.
(c) Deutscher Apotheker Verlag, Stuttgart Krankenhauspharmazie AABG: Preisgünstige Therapie- alternativen nach § 115c SGB V Vergleichstabellen zu inhalierbaren Glucocorticoiden und inhalierbaren Beta2-Sympathomimetika im Gesamtkontext der Behandlung des Asthma bronchiale Nils Keiner, Verena Handwerk und Dominic Fenske im Auftrag der AABG-Arbeits-gruppe ADKA e.V. Inhalierbare Glucoco
De beurs van Nürnberg - 2012 1. De algemene sfeer De cijfergegevens over het aantal deelnemers en bezoekers variëren weinig tegenover vorige jaren, maar deze speelgoedbeurs blijft leidinggevend op wereldniveau. De crisis is wel duidelijk aanwezig en er wordt duidelijk bespaard op allerlei randanimatie. Dit jaar kregen de adolescenten alle aandacht: als '4Teens' - eigenlijk de lee

 Symptoms and signs of heart failure
Symptoms and signs of heart failure 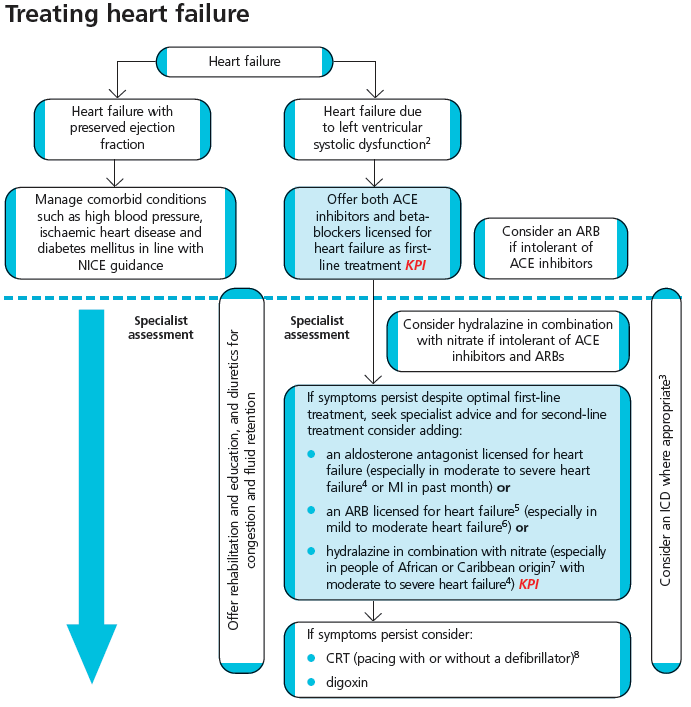 Drug Treatment for Heart Failure Due to LVSD
Drug Treatment for Heart Failure Due to LVSD